

ABSTRACT
The typical chest radiographic and computed tomographic (CT) findings of COVID-19 include bilateral, multifocal parenchymal opacities (ground-glass opacities with or without consolidation, and crazy paving). In most cases, the opacities are predominantly in the peripheral and lower lung zones, and several have rounded morphology. However, these imaging findings are not pathognomonic for COVID-19 pneumonia and can be seen in the setting of other viral and bacterial infection as well as noninfectious causes such as drug toxicity and connective tissue disease. Most radiology professional organizations and societies recommend against performing routine screening CT to diagnose or exclude COVID-19.
INTRODUCTION
The lungs are the most common site of infection in COVID-19, and progression to respiratory failure is the most common cause of death. In this brief summary we describe the role of thoracic imaging in COVID-19.
CHEST RADIOGRAPHY IN COVID-19
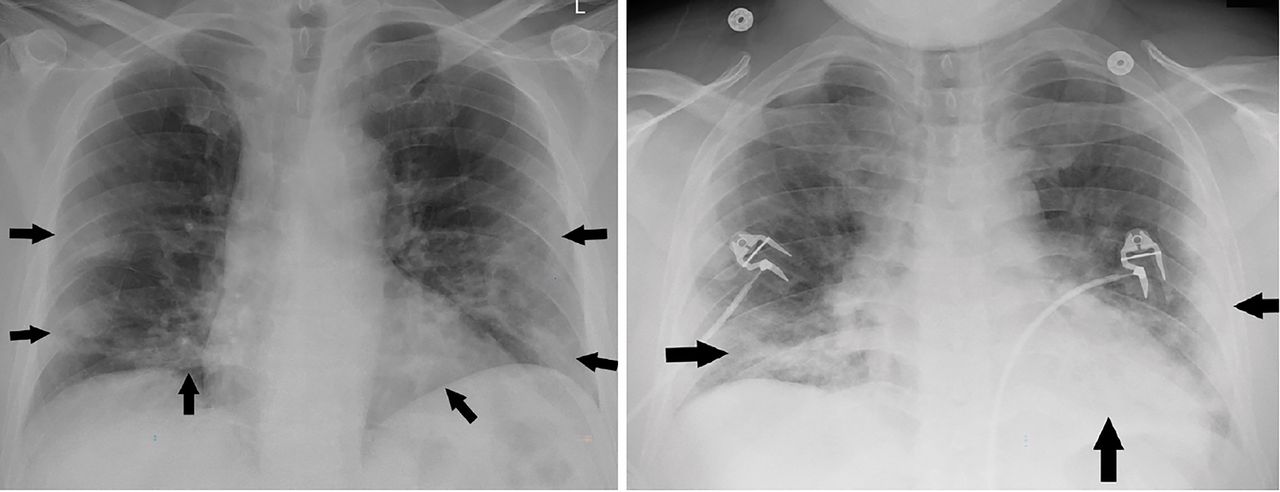
Chest radiography is considered an appropriate initial imaging diagnostic test for most patients with lower respiratory tract infection, including those suspected of having COVID-19. The radiographic abnormalities in COVID-19 mirror those on computed tomography (CT), demonstrating bilateral, peripheral, and mid-lower lung zone-predominant consolidation (Figure 1).1 However, in patients who have a high pretest probability of COVID-19, atypical findings such as diffuse interstitial changes or unilateral focal consolidation (Figure 2) should not dissuade the radiologist from suspecting an infection, including COVID-19, as a possible diagnosis.
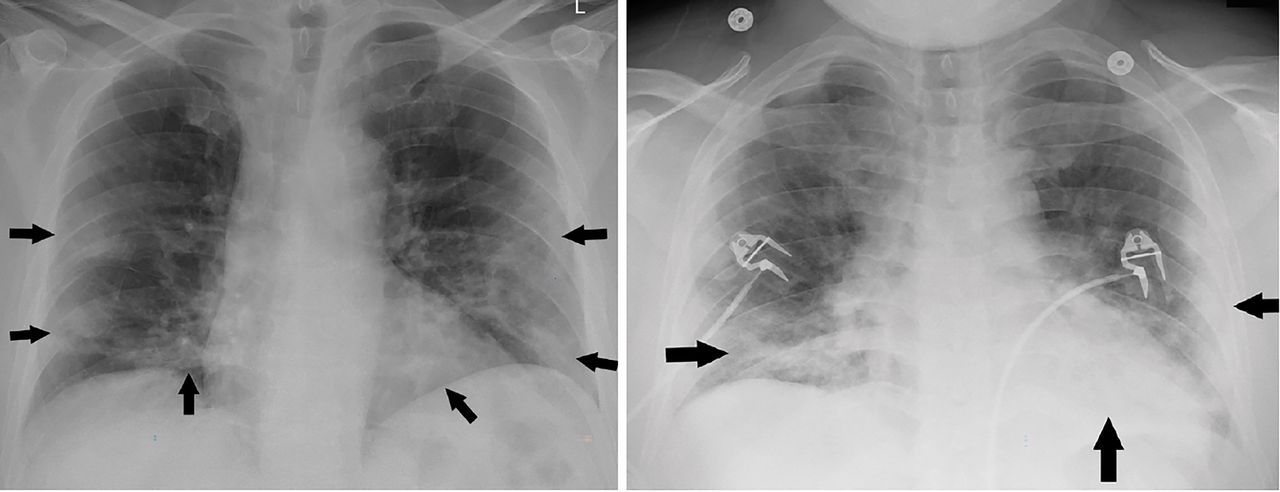
Portable chest radiographs of a patients with COVID-19 demonstrating classic bilateral, multifocal peripheral airspace opacities in the midlower lung zones.
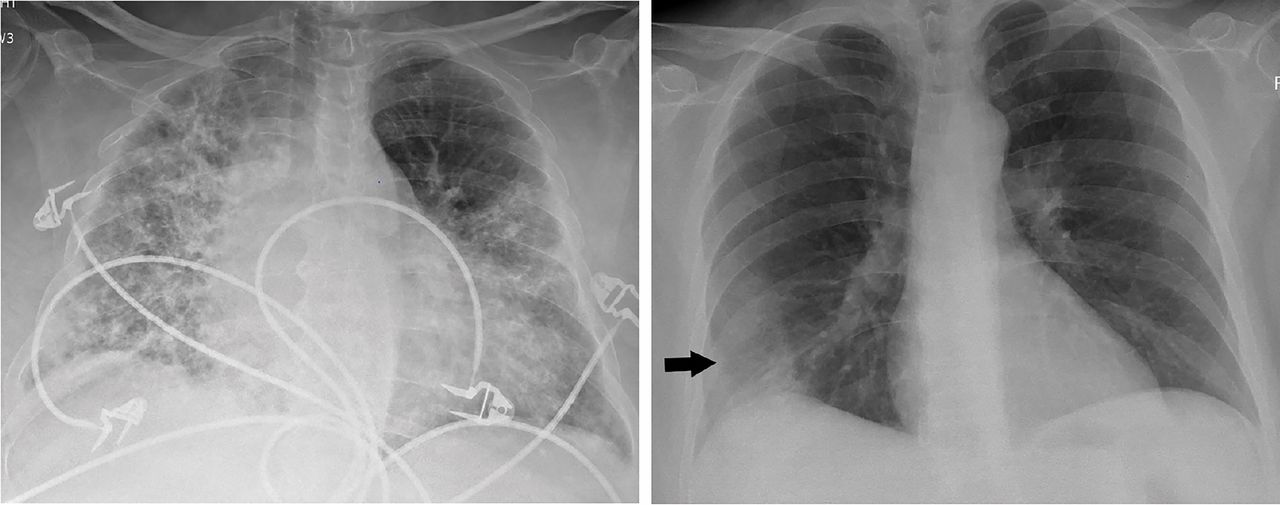
Portable chest radiographs of patients with COVID-19 demonstrating atypical features of diffuse bilateral interstitial changes (A) and unilateral consolidation (B).
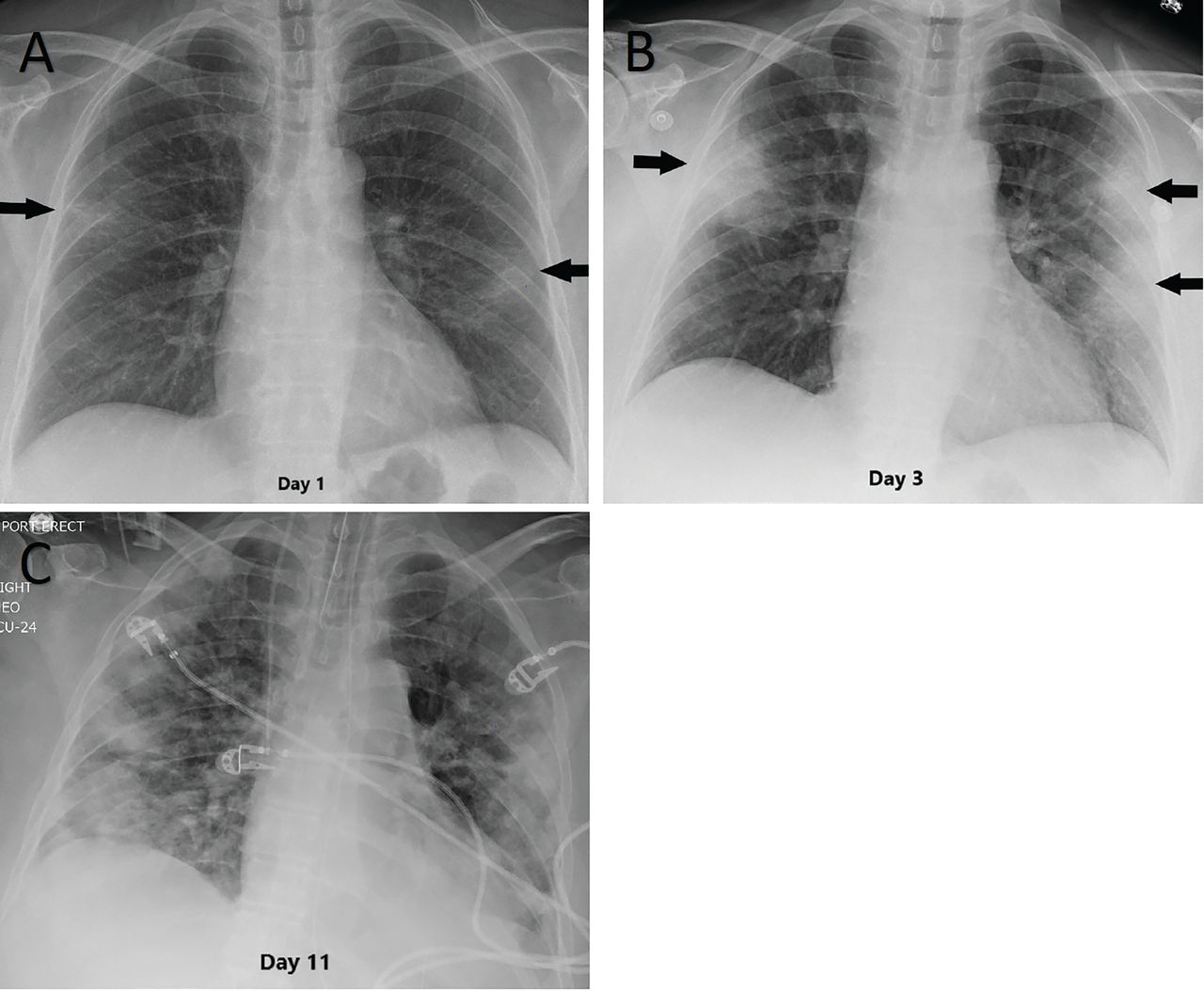
In patients with progressive disease, the density and extent of parenchymal changes typically increase over time (Figure 3). The severity of chest radiographic findings peaks 10 to 12 days after the onset of symptoms.1

Serial chest radiographs in a 53-year-old woman with COVID-19 demonstrate peripheral opacities on the day of onset of symptoms (A) with rapid worsening by day 3 (B). The patient was subsequently intubated, with the peak severity of parenchymal findings on day 11 (C).
Unfortunately, most bacterial pneumonias also present as consolidation, and it is difficult to distinguish them from viral infections on chest radiography. The subtleties of rounded morphology and crazy paving associated with COVID-19 can only be appreciated on CT and not plain chest radiographs. Cavitation within an airspace consolidation likely suggests a superadded infection.
Moreover, chest radiography has a high false-negative rate, especially in the early stage of infection, and should not be used as a screening tool to rule out COVID-19. In fact, baseline radiography has a lower sensitivity (69%) than initial reverse transcriptase polymerase chain reaction testing (91%).1
THROUGH-GLASS RADIOGRAPHY TO AVOID SPREADING THE VIRUS
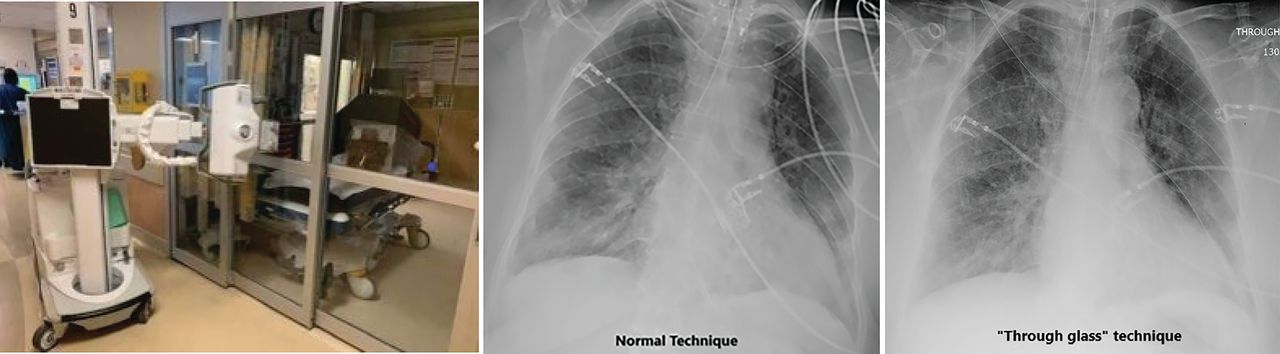
During the pandemic, our hospital (as well as many others in the United States) has employed a method of obtaining portable radiographs in cases of confirmed or suspected COVID-19 through the glass wall of the patient’s room in the intensive care unit and in the emergency department. With some minor technical modifications, the chest radiographs taken “through glass” are comparable to those obtained by the standard method (Figure 4). This technique has the potential to reduce the consumption of personal protective equipment by radiology technicians and to reduce the risk of machine contamination.2
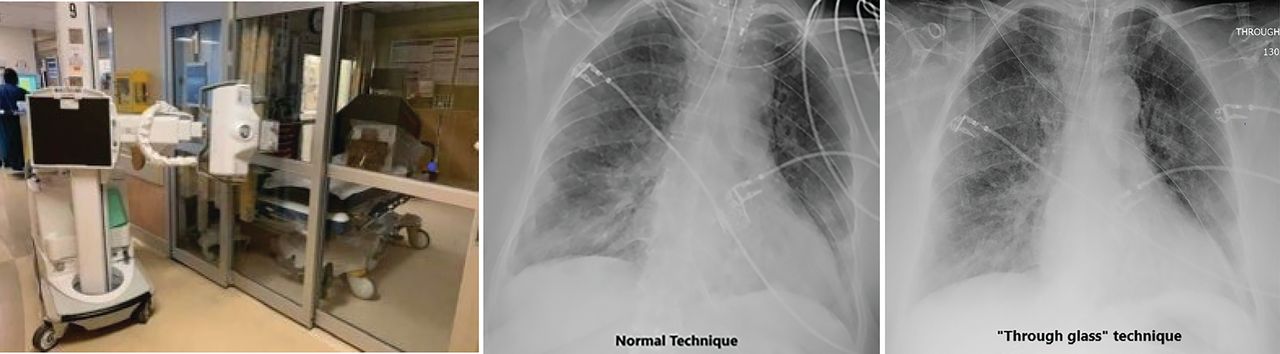
(Left) Setup for obtaining chest radiographs through the glass wall of the room of a patient with suspected or confirmed COVID-19. (Middle) A radiograph obtained in the conventional manner. (Right) A radiograph obtained by the “through-the-glass” method.
COMPUTED TOMOGRAPHY IN COVID-19
The CT features of COVID-19 pneumonia are not pathognomonic and are similar to those of pneumonia due to other coronaviruses such as SARS and MERS as well as other bacterial and viral infections, most notably influenza pneumonia. Moreover, noninfectious etiologies such as drug toxicities and connective tissue disease may produce similar imaging findings. Hence, integration of the clinical presentation, exposure history, prevalence of COVID-19 in the community, and personal risk factors are of paramount importance in suspecting and making the diagnosis.
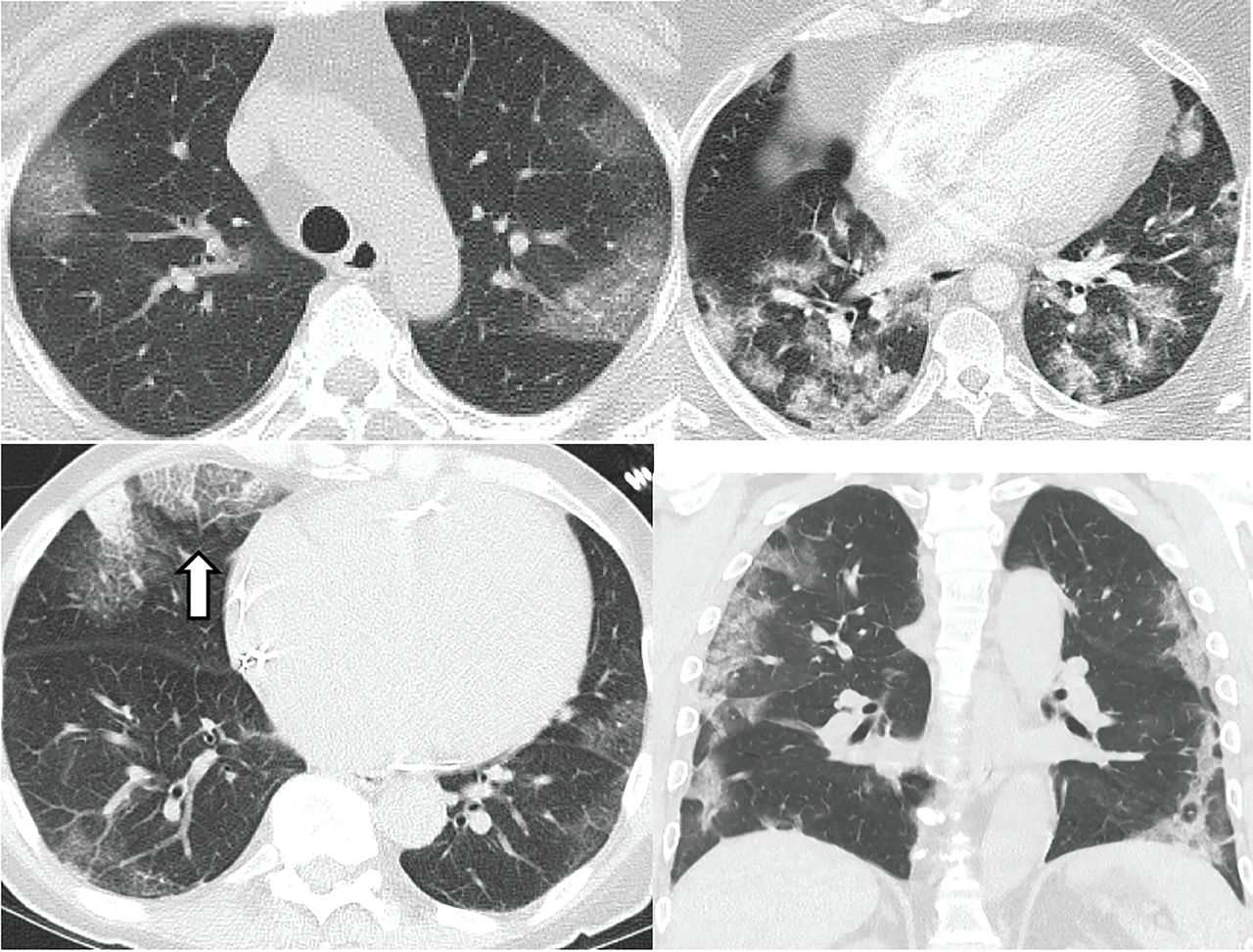
The most characteristic CT findings of COVID pneumonia are ground-glass opacities with or without consolidation and superimposed interlobular septal thickening (crazy-paving appearance). A reverse halo (central ground-glass opacities with an interrupted peripheral rim of consolidation) has also been described, especially in the later stages of the disease. These lung opacities are frequently bilateral, multilobar, posterior, peripheral, and basilar in distribution and often rounded in morphology (Figure 5).3–9
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Typical computed tomographic imaging features of COVID-19. Unenhanced axial images of the lungs of four different patients with COVID-19 demonstrate bilateral, multifocal, peripheral ground-glass opacities, and consolidation, most with rounded morphology. “Crazy paving” (ground-glass opacities with superimposed interlobular septal thickening and intralobular lines) is seen in (C) (white arrow).
Over time, the ground-glass opacities may worsen with progressive consolidation and more lobes involved. The severity of the CT findings peaks 10 to 12 days after the onset of symptoms.5 A subset of hospitalized patients with COVID-19 (16.1% in one series) develop extensive lung disease with acute respiratory distress syndrome (ARDS).10
Gattinoni11 describes 2 different phenotypes in patients with COVID-19: “type L, “ characterized by low elastance, low ventilation-to-perfusion ratio, low lung weight, low recruitability, and CT findings of subpleural opacities; and “type H,“ characterized by high elastance, high ventilation-to-perfusion ratio, high lung weight, high recruitability, and CT findings of ARDS. Understanding the different pathophysiology is crucial for appropriate patient management.
As with most other viral pneumonias, features not typically seen in cases of COVID-19 include pleural effusions, lymphadenopathy, cavitation, and small discreet nodules (including centrilobular or tree-in-bud opacities).12,13
THE RADIOLOGICAL SOCIETY OF NORTH AMERICA CONSENSUS STATEMENT
The Radiological Society of North America (RSNA) published a consensus statement in March 2020 on standardized reporting of CT findings related to COVID-19. It had several goals, including to reduce uncertainty and variability in reporting findings potentially attributable to COVID-19 and to enhance the referring providers’ understanding of common radiographic findings.14
Typical features, according to the RSNA report, are lower lobe-predominant, peripheral-predominant, multiple, bilateral foci of rounded ground-glass opacities with or without crazy paving, peripheral consolidation, and a reverse halo perilobular pattern (seen later in the disease).
Indeterminate features are absence of typical features and the presence of multifocal, diffuse, perihilar, or unilateral ground-glass opacities with or without consolida tion lacking a specific distribution and are nonrounded or nonperipheral. Few very small ground-glass opacities with a nonrounded and nonperipheral distribution.
Atypical features are absence of typical or indeterminate features and the presence of isolated lobar or segmental consolidation without ground glass opacities, discrete small nodules (centrilobular, “tree-in-bud”), lung cavitation, or smooth interlobular septal thickening with pleural effusion.
Caveats. The statement advises including cautionary language in radiographic reports. If typical features of COVID-19 are present, for example, the statement advises mentioning that other processes can also cause a similar imaging pattern. If indeterminate features are seen, the statement points out that these features are nonspecific. Even if no findings are present to indicate pneumonia, it notes that CT may be negative in the early stages of COVID-19.
ROLE OF CT IMAGING IN COVID-19
The sensitivity of chest CT in detecting COVID-19 pneumonia has been reported to be 97%, the specificity 25% to 56%, and the accuracy 68% to 72%.9,12,15,16 CT findings may be negative in 20% to 25% of patients early in the course of the disease. Hence, a normal chest CT scan cannot exclude the diagnosis of COVID-19, especially early after the onset of symptoms.16 CT has been reported to become abnormal in more than 95% of cases after 5 to 6 days of infection.
The available literature suggests that CT imaging may be helpful in early detection of pneumonia in patients in whom COVID-19 is strongly suspected but who have an initial false-negative reverse transcription polymerase chain reaction (RT-PCR) screening test.12,17,18
CURRENT RECOMMENDATIONS
Most radiology professional organizations and societies as well as the US Centers for Disease Control and Prevention currently recommend against performing routine screening CT to diagnose or exclude COVID-19.14,19 CT is commonly indicated for hospitalized, symptomatic patients with worsening respiratory status or in patients with moderate to severe features of COVID-19 regardless of the COVID-19 test results.14,19 The societies also suggest that hospitals consider deploying portable radiography units in ambulatory care facilities for use when chest radiographs are considered medically necessary. The surfaces of these machines can be easily cleaned, avoiding the need to bring patients into radiography rooms.
FLEISCHNER SOCIETY STATEMENT
In a multinational consensus statement, the Fleischner Society states that in a resource-constrained environment (in which personal protective equipment or COVID-19 testing may not be available), imaging is indicated for medical triage of patients with suspected COVID-19 who present with moderate to severe clinical features and a high pretest probability of the disease.19
The report further states that imaging is not routinely indicated as a screening test for COVID-19 in patients without symptoms, nor for patients with mild features of COVID-19 unless they are at risk for disease progression. Imaging is indicated for patients with moderate to severe features of COVID-19 regardless of the COVID-19 test results, and for patients with COVID-19 and evidence of worsening respiratory status. In a resource-constrained environment where access to CT is limited, chest radiography may be preferred for patients with COVID-19 unless features of respiratory worsening warrant the use of CT.
Daily chest radiographs are not indicated in stable intubated patients with COVID-19. CT is indicated in patients with functional impairment or hypoxemia after recovery from COVID-19. And COVID-19 testing is indicated in patients incidentally found to have findings suggestive of COVID-19 on a CT scan.19
All patients undergoing imaging should be masked.20 Appropriate infection-control procedures should be followed before scanning subsequent patients.14
Footnotes
The statements and opinions expressed in COVID-19 Curbside Consults are based on experience and the available literature as of the date posted. While we try to regularly update this content, any offered recommendations cannot be substituted for the clinical judgment of clinicians caring for individual patients.
- Copyright © 2020 The Cleveland Clinic Foundation. All Rights Reserved.