Article Text

Abstract
Immune checkpoint inhibitors (ICIs) are the standard of care for the treatment of several cancers. While these immunotherapies have improved patient outcomes in many clinical settings, they bring accompanying risks of toxicity, specifically immune-related adverse events (irAEs). There is a need for clear, effective guidelines for the management of irAEs during ICI treatment, motivating the Society for Immunotherapy of Cancer (SITC) to convene an expert panel to develop a clinical practice guideline. The panel discussed the recognition and management of single and combination ICI irAEs and ultimately developed evidence- and consensus-based recommendations to assist medical professionals in clinical decision-making and to improve outcomes for patients.
- antineoplastic protocols
- guidelines as topic
- immunotherapy
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The introduction of new cancer immunotherapies for the treatment of metastatic cancer and for the adjuvant therapy for high-risk primary disease has enabled long-term, potentially curative responses in subsets of populations of patients with cancer. Immune checkpoint inhibitors (ICIs) are antibodies designed to block key regulatory signals that dampen immune responses, counteracting immune suppression in the tumor microenvironment and thus enabling tumor-reactive T cells to mount an effective anticancer response. Currently, US Food and Drug Administration (FDA)-approved ICIs fall into two major classes: those that target the programmed cell death protein 1 (PD-1) and programmed death-ligand 1 (PD-L1) (antibodies to the PD-(L)1 axis) and those that target the cytotoxic T lymphocyte antigen-4 (CTLA-4) in the context of the CTLA-4-CD28 axis (anti-CTLA-4 antibodies).1 These therapies have been approved for the treatment of a wide variety of cancer types. A study of ICI usage estimated that in 2018, 44% of patients with metastatic solid or hematological tumors in the US were eligible for treatment with ICIs.2 ICIs are also a focus of active drug development, and a number of ongoing trials are evaluating novel antibodies or testing approved ICIs in combination with other treatment modalities including chemotherapies or targeted agents. The use of ICIs as adjuvant therapy has been approved for high-risk melanoma and esophageal and gastroesophageal junction (GEJ) cancers, and studies of peri-operative checkpoint blockade (including in the neoadjuvant setting) are ongoing for a wide variety of other cancers. Because ICIs are used across the spectrum of disease from early to late stage, the risks of treatment (including the potential for long-lasting side effects) should be weighed against the goals of therapy.
As with any modality, treatment with ICIs can result in adverse events (AEs). AEs related to the immunological mechanism of action of immunotherapy are commonly referred to as immune-related AEs (irAEs). AEs, including irAEs, are graded according to a standard scale of severity such as the Common Terminology Criteria for Adverse Events (CTCAE v5.0),3 which also assists in comparing toxicities across trials. A systematic review found that patients treated with anti-PD-(L)1 inhibitors developed irAEs at a rate of 74% (14% grade ≥3), those treated with anti-CTLA-4 inhibitors at a rate of 89% (34% grade ≥3), and those treated with combination ICIs at a rate of 90% (55% grade ≥3).4 Importantly, the presentation of common irAEs (eg, thryoiditis, dermatitis, etc) differs from that of chemotherapy-related AEs. In addition, the timing of irAEs is far less predictable, with the potential for events to occur and persist long after cessation of treatment. The difference in expected frequencies of AEs between immunotherapy and chemotherapy or other modalities is typically attributed to the unique mechanism of action of ICIs.4 5
A number of guidelines detail recommendations for the management of immunotherapy-related toxicities, including the American Society for Clinical Oncology (ASCO), the European Society for Medical Oncology (ESMO), the National Comprehensive Cancer Network (NCCN), and a prior consensus statement from the Society for Immunotherapy of Cancer (SITC).6–9 The overall goal of any guideline, including this one, is to assist in clinical decision-making to provide the best outcomes for patients. Guidelines from different organizations should be complementary in helping providers care for their patients. Since the publication of the 2017 consensus statement on toxicity management from SITC, rapid progress in the field of immunotherapy leading to expansion in the number of clinical trials and analyses of toxicities have resulted in a concordant increase in the data available about irAEs, including additional insight on optimal management strategies as well as a new appreciation for uncommon presentations such as ICI-associated celiac disease. Coupled with ever-expanding FDA approvals for new therapies and indications, and enhanced public awareness of immunotherapy, these new data necessitated the development of updated clinical practice guidelines. As the leading member-driven international organization devoted to advancing the science and application of cancer immunotherapy, SITC assembled an expert panel to develop evidence- and consensus-based recommendations to provide guidance to clinicians in the management of ICI-associated toxicities. The expert panel discussed and generated recommendations on the diagnosis, treatment, and risk factors associated with toxicities occurring during ICI treatment. This manuscript reports the panel’s recommendations and provides guidance to medical professionals, with the goal of improving patient outcomes during and following treatment with ICIs. These recommendations are not intended to supplant sound clinical judgment, but to provide clinicians with the most current thinking on how experts manage AEs arising from treatment with ICIs. The full series of SITC clinical practice guidelines can be found via the SITC website.10 This guideline may be updated as new evidence becomes available.
Guideline development methods
The Institute of Medicine’s (IOM) Standards for Developing Trustworthy Clinical Practice Guidelines were used as a model to develop the recommendations in this manuscript. IOM standards dictate that guideline development is led by a multidisciplinary expert panel using a transparent process where both funding sources and conflicts of interest are readily reported. This clinical practice guideline is intended to provide guidance and is not a substitute for the professional judgment of individual treating physicians.
Conflict of interest management
As outlined by IOM standards, all financial relationships of expert panel members that might result in actual, potential, or perceived conflicts of interest were individually reported. Disclosures were made prior to the onset of manuscript development and updated on an annual basis. In addition, panel members were asked to articulate any actual or potential conflicts at all key decision points during guideline development, so that participants would understand all possible influences, biases, and/or the diversity of perspectives on the panel. Although some degree of relationships with outside interests are to be expected among experts, panel candidates with significant financial connections that may compromise their ability to fairly weigh evidence (either actual or perceived) were not eligible to participate in guideline development.
Recognizing that guideline panel members are among the leading experts on the subject matter under consideration and guideline recommendations should have the benefit of their expertize, any identified potential conflicts of interests were managed as outlined in SITC’s disclosure and conflict of interest resolution policies. As noted in these policies, panel members disclosing a real or perceived potential conflict of interest may be permitted to participate in consideration and decision-making of a matter related to that conflict, but only if deemed appropriate after discussion and agreement by the expert panel.
The financial support for the development of this guideline was provided solely by SITC. No commercial funding was received.
Recommendation development
Panel recommendations are based on literature evidence, where possible, and clinical experience, where appropriate.11 Consensus for the recommendations herein was generated by open communication and scientific debate in small-group and whole-group settings, surveying and responses to clinical questionnaires, as well as formal voting in consensus meetings.
For transparency, a draft of this clinical practice guideline was made publicly available for comment during the development process and prior to publication. All comments were evaluated and considered for inclusion into the final manuscript according to the IOM standard.
Evidence rating
The evidence-based and consensus-based recommendations of the panel were refined throughout the development process in order to obtain the highest possible agreement among the experts, however, the minimum threshold was defined as 75% approval among the voting members. Evidence supporting panel recommendations was graded according to the Oxford Centre for Evidence-Based Medicine (OCEBM) Levels of Evidence Working Group ‘The Oxford Levels of Evidence 2’ (2016 version). A summary of the OCEBM grading scale is mentioned in table 1. The level of evidence (LE) for a given recommendation is expressed in parentheses following the recommendation (eg, LE: 1). Recommendations without an associated LE were based on expert consensus.
Summary of ‘The Oxford Levels of Evidence 2’ (Adapted from OCEBM Levels of Evidence Working Group)
General recommendations
The same mechanisms by which ICIs exert antitumor effects are thought to be partially responsible for the development of irAEs—namely, self-reactive T cells escaping central tolerance due to inhibited immune checkpoints. Other mechanisms have been proposed, including epitope spreading and dysbiosis that causes microbiota-derived products to be exposed to innate immune cells, activating self-reactivity. Although certain irAEs require organ-specific management considerations, some overarching management principles apply to all ICI-related toxicity. While many irAEs resolve with interruption of therapy and/or immunosuppressives, cases that do not respond to first-line interventions should be managed in consultation with appropriate specialties (eg, cardiology, gastroenterology, neurology, rheumatology, etc). Organ-specific recommendations may be found in the later sections of this manuscript and general concerns for managing irAEs include patient selection and risk factors, expected timing, terminology, management, and possibility for overlapping toxicity, each of which is discussed below. Several ongoing trials are investigating the mechanisms responsible for specific irAEs, the impact of interventions to manage irAEs on ICI efficacy, and strategies to reduce the incidence of irAEs. However, no completed randomized controlled trials for irAE management have been published to date.
Patients with pre-existing autoimmune disorders have frequently been excluded from clinical trials evaluating ICIs, owing to concerns that autoimmune disorders could be exacerbated due to therapy. However, a systematic review of patients with pre-existing autoimmunity who received ICI therapy showed that these patients do not appear to develop de novo irAEs at an increased rate, but that flare-ups of existing autoimmunity are common during ICI treatment (occurring in 50% of patients).12 The frequency, severity, and timing of the toxicities associated with the patient population with underlying autoimmune conditions will soon be evaluated by an ongoing NCTN trial (ECTCN10204). Given the likelihood of autoimmune flare-ups, clinical decision-making on the use of ICIs for patients with existing autoimmunity should carefully weigh the severity and potential consequences of autoimmune disease exacerbation versus the potential benefits of ICI treatment. Additional guidance regarding patient selection may be found in tumor type-specific guidelines, including those published by SITC.13–17
The identification of reliable predictors for risk of irAEs is an ongoing area of investigation. In some studies, potential risk factors identified to be associated with increased irAE incidence include the presence of thymic tumors, elevated body mass index (BMI), specific human leukocyte antigen (HLA) genotypes, and baseline deviations from normal ranges in the levels of some cytokines such as interleukin (IL)-6 and IL-17.18–26 Of note, however, no readily available biomarkers with predictive value for the development of irAEs have been validated at the time of publication.
The terminology surrounding AEs may be confusing or inconsistent. Clinical trials may describe AEs, treatment-related AEs (TRAEs) or treatment-emergent AEs, and irAEs. The term ‘AEs’ refers to any adverse event, including those not related to treatment. ‘TRAEs’ encompasses any AE resulting from a therapy being administered and may include AEs from other treatments used in conjunction with ICIs. For the purposes of this manuscript, the authors have defined ‘irAE’ as any AE of likely immunological origin arising during or after treatment with an ICI, in accordance with the definition used in a number of clinical trials investigating ICIs.27 28 Grades of AEs are defined as in the CTCAE v5.0.3
Importantly, the timing of irAE emergence can differ notably from other TRAEs. While many irAEs typically occur in a short time-frame following administration of treatment (as with other TRAEs),29 30 irAEs can occur at any point during or after cessation of treatment (beyond 6–12 months).31 The exact mechanisms underlying this phenomenon are under active investigation. Finally, some irAEs may cause life-long effects, such as type 1 diabetes and thyroid destruction. Additionally, hypophysitis can disrupt normal gonadal/menstrual function and cause galactorrhea.32 Although autoimmune hypophysitis is rare in healthy women, the incidence may be higher in women with prior pregnancies.33 It is not known if immunotherapy affects fertility in women of childbearing age, nor if the risk is greater than that posed by standard chemotherapy agents. Additionally, ICI therapy is considered category D in pregnancy, and evidence from solid organ transplant recipients indicates that the risk of fetal malformation is greatly increased if patients are exposed to immunosuppressives such as mycophenolate,34 35 which are commonly used to manage irAEs. While three isolated case reports have been published of successful pregnancies carried to term while on ICI therapy for metastatic melanoma,36–38 adherence to pregnancy prevention is strongly encouraged during treatment.
Managment for irAEs also differs from those for AEs with conventional cancer therapies. Treatment for irAEs typically includes immunosuppression with corticosteroids or other immunosuppressive agents in addition to symptomatic treatments and withholding of ICI dose and/or permanent discontinuation based on irAE grade and resolution as clinically appropriate. For severe toxicities, consultation with a specialist is recommended.39 In contrast to conventional chemotherapy or molecularly targeted therapy, there is no known role for dose reduction of ICIs in the management of irAEs.
Systemic corticosteroids are commonly used as a first-line treatment for irAEs, and they may be associated with their own toxicities. Common toxicities resulting from long-term corticosteroid therapy include hypertension, osteoporosis (increasing risk of bone fractures), cataracts, hirsutism, stria distensae, weight gain, gastrointestinal (GI) dysfunction, insomnia and mental status changes, lower extremity edema, muscle weakness, metabolic dysfunction (notably, hyperglycemia and type II diabetes) and, most importantly, increased risk for infections (bacterial, fungal, and viral).40 41 Acute high-dose steroid use is also associated with toxicities, including gastritis, mental status changes, and hyperglycemia.42 43 Therefore, while physicians should monitor patients for ICI toxicities, they should also be aware of the potentially increased risk of overlapping toxicities if corticosteroids are used, such as diabetes or musculoskeletal toxicities (as discussed below), as well as the need for monitoring or prophylaxis related to corticosteroid toxicities. The subsequent use of other immunosuppressive agents to treat corticosteroid-refractory irAEs also carries potential risks, with which clinicians should familiarize themselves prior to administration. However, in patients who do not respond to initial corticosteroid therapy, second-line immunosuppressive therapy should be considered.
In many cases, ICI therapy may be temporarily interrupted due to toxicity. Once the toxicity has sufficiently resolved (generally to grade 1 symptoms or lower with ≤10 mg prednisone equivalents per day), patients may be re-challenged. A retrospective analysis of 40 patients with a variety of tumor types who were re-challenged with anti-PD-(L)1 ICIs found that 43% developed recurrences of prior irAEs and that 13% developed new irAEs.44 Another retrospective analysis of 38 patients with non-small cell lung cancer (NSCLC) who were re-challenged with ICIs found a rate of 26% for recurrent irAEs and 26% for new irAEs.45 In both of these studies, the rate of recurrence was higher in patients who had initially experienced a grade ≥3 irAE, although this difference did not reach statistical significance.44 45
A notable group of irAEs—myositis, myocarditis, and myasthenia gravis—are frequently seen in the same patients and deserve particular attention due to a high mortality rate. Myositis and myasthenia gravis share a number of overlapping symptoms (ocular, bulbar, axial, and respiratory pattern of weakness) and frequently occur in a cluster with myocarditis. Given the high rate of fatality for patients who develop myasthenia gravis (20%) or myocarditis (17%), suspicion of one or more of these irAEs should prompt evaluation for all three.46 47 A retrospective analysis of patients with skin cancer found that 32% of myositis cases were accompanied by myocarditis, and that 5% of myositis cases were accompanied by myasthenia gravis.48 A systematic analysis of patients that developed myasthenia gravis found that this irAE was accompanied by myositis and myocarditis at rates of 16% and 9%, respectively.46 Special considerations for the management of these three irAEs are discussed in more detail in the organ-specific sections of this manuscript. Additionally, studies are increasingly recognizing that multisystem irAEs can occur, and therefore it is important to be mindful of the possibility that different irAEs may occur concomitantly in the same patient.49
Specific considerations for important irAEs affecting a variety of organs and systems are discussed in individual sections later in the manuscript. The sections are generally ordered by expected frequency of clinical occurrence, from most to least common. A literature review of each specific toxicity is accompanied by recommendations regarding the diagnosis and/or management of that toxicity.
General panel recommendations
The following recommendations are intended to form a generalized framework for the management of irAEs resulting from ICI treatment, including direction for at what grade of toxicity to hold and/or permanently discontinue therapy as well as optimal timing and dosing for administration of corticosteroids and/or other immunosuppressive agents. Exceptions to these recommendations or deviations from these general management principles may exist for certain toxicities. These exceptions will be noted in the individual toxicity sections of this manuscript.
Patients should receive dedicated education on irAEs by a medical professional and may receive additional materials such as informational booklets or reference cards.
Patients should be encouraged to use contraception while receiving immunotherapy. Fertility should be discussed prior to treatment.
The following tests should be performed prior to beginning ICI therapy: complete blood count (CBC) with differential, comprehensive metabolic panel (CMP), thyroid-stimulating hormone (TSH), free thyroxine (fT4). Urinalysis should be considered to evaluate for baseline kidney disease.
Consider performing a baseline electrocardiogram (EKG) on patients deemed at a higher risk for myocarditis (eg, cardiac comorbidities, diabetes mellitus, anti-PD-(L)1 with anti-CTLA-4 ICI combination therapy, etc). Baseline troponin testing may also be considered to provide information for evaluating potential future cardiac toxicity.
When beginning corticosteroid therapy, patients should be specifically counseled about potential toxicities, including hyperglycemia, mood disturbances, insomnia, gastritis, weight gain, and opportunistic infections (eg, Pneumocystis pneumonia) (LE: 140 41).
CBC with differential, CMP, TSH, and fT4 tests should be performed intermittently throughout the course of treatment in patients receiving ICI therapy.
Patients should be referred to a specialist when they experience toxicities of grade ≥3, if toxicities of any grade do not respond to steroid treatment, if toxicities require hospitalization or for selected lower-grade toxicities in which diagnosis or management advice is needed, such as neurological and rheumatological toxicities (eg, inflammatory arthritis not interfering with instrumental activities of daily living, mild pain with erythema, or joint swelling).
Diagnostic evaluation for all irAEs should attempt to rule out other possible etiologies (eg, diarrhea/colitis associated with Clostridium difficile infection), but treatment for irAEs should be initiated as is deemed clinically appropriate.
For patients with life-threatening autoimmune disorders, the decision to initiate ICI therapy should only be considered after a careful risk-benefit discussion between patient and provider, and consideration of alternative therapies. Consideration should include risks of autoimmune flares against the survival benefits of ICI therapies, especially in cancers with high expected rates of durable responses (LE: 112).
Patients with a history of non-life-threatening autoimmune disease should only receive ICIs after counseling on the possibility of exacerbation or flare-ups. These patients should be monitored closely for exacerbations of their existing autoimmunity while being treated with ICIs, and concurrent monitoring and treatment by an appropriate specialist should be considered (LE: 112).
Unless otherwise specified, patients experiencing grade 1 irAEs should be monitored for worsening symptoms, but may continue ICI therapy.
Unless otherwise specified, patients experiencing grade 2 irAEs should have ICI therapy temporarily withheld and be treated with corticosteroids depending on the toxicity in question.
The decision to re-challenge patients with ICIs may be complex. Factors that may cause clinicians to lean away from re-challenge include severe or life-threatening irAEs, requirement for prolonged or multiple immunosuppressants, and a history of long-term ICI therapy and/or patients with complete responses or prolonged clinical benefit.
Unless otherwise specified, patients who have experienced grade 2 irAEs may be re-challenged with ICI therapy if their signs and symptoms have resolved or are controlled with ≤10 mg of prednisone (or equivalent) per day (LE: 344 45).
The decision to re-challenge a patient who has experienced grade 3 or 4 irAEs should be risk-adjusted based on anticipated benefit with therapy versus the potential for toxicity (LE: 344 45).
Patients experiencing any grade of myositis, myocarditis, or neurological symptoms (such as myasthenia gravis):
Should be referred to a specialist.
Should be tested with a shared set of diagnostics, due to the possibility of overlapping symptoms and high risk to the patient.
Should have testing including erythrocyte sedimentation rate (ESR), C reactive protein (CRP), creatine kinase (CK), antibody tests (acetylcholine, muscle-specific kinase (MusK), striational), aldolase, troponin, EKG, nerve conduction, and electromyography (EMG).
Should receive frequent pulmonary assessment in addition to typical irAE treatment (ie, corticosteroids).
Gastrointestinal toxicity
Nausea
Nausea (sometimes with accompanying vomiting) is a relatively common ICI-associated AE, and occurs in 12% of patients being treated with PD-(L)1 inhibitors, 19% of patients being treated with CTLA-4 inhibitors, and 25% of patients being treated with combination CTLA-4 and PD-(L)1 inhibitors. Despite the frequent occurrence of low-grade nausea, events of grade ≥3 are rare and occur in 0%–2% of patients.4 While nausea and vomiting are not typically serious alone, they may be symptomatic of other conditions affecting the upper GI tract, which require intervention, including infection, GI metastases, endocrinopathy, or other irAEs such as gastritis or colitis. A number of effective options exist for the treatment of nausea, and the most appropriate agent depends on assessment of the individual patient.50 51
Upper GI adverse events
In addition to nausea, other irAEs of the upper GI tract have been observed, although they are rare. The irAEs that have been observed include gastritis,52 duodenitis,53 and esophagitis.54 55 In the largest case series on upper tract irAEs, gastric involvement was more common than duodenal involvement by both endoscopy and histology.56 Information on the management of these irAEs is sparse, but management techniques often resemble those used for diarrhea and colitis.
Diarrhea and colitis
Diarrhea is another common irAE. Diarrhea has been reported in approximately 44% (10% grade ≥3) of patients treated with combination CTLA-4 inhibitors and PD-(L)1 inhibitors, 36% (8% grade ≥3) of those treated with CTLA-4 inhibitors, and 11% of those treated with PD-(L)1 inhibitors (1% grade ≥3).4 57 Diarrhea merits close monitoring, since severe diarrhea alone is clinically concerning, and the presence of diarrhea may indicate colitis, another serious and potentially life-threatening irAE.
Colitis is inflammation of the colon, with diarrhea being a common symptom. The diagnosis of colitis may be inferred by symptoms, and alarm symptoms include pain and hematochezia. Colitis occurs in 16% (11% grade ≥3) of patients treated with combination ICIs, 8% (5% grade ≥3) of those treated with CTLA-4 inhibitors and 1% (1% grade ≥3) of those treated with PD-(L)1 inhibitors.4 58 A study of 182 patients with ICI-induced colitis showed that positive fecal lactoferrin and fecal calprotectin >150 μg/g of stool were both predictive of inflammation, as detected by endoscopic and histological findings.59 Fecal lactoferrin and calprotectin are more well-studied in the context of inflammatory bowel disease than in ICI-induced colitis. While data from ICI-induced colitis does correlate with endoscopic findings, this evidence is not currently strong enough to justify the use of these tests exclusively (ie, excluding endoscopy if fecal lactoferrin and calprotectin tests are negative). The incidence of immune-related GI AEs is higher in patients treated with combination anti-CTLA-4/anti-PD-(L)1 regimens compared with ICI monotherapy, but the rates of colitis do not vary between tumor types for patients receiving ICIs targeting the PD-1/PD-L1 axis.58
Colitis can lead to a number of complications, including bowel perforation, ischemia, necrosis, bleeding, and toxic megacolon. The median time until the onset of diarrhea or colitis is 5–10 weeks.29 60 Upon treatment of patients with corticosteroids, symptoms of diarrhea and colitis may be expected to improve or resolve in 1–2 weeks.61 62 In a retrospective study, 34% of patients who were re-challenged experienced recurrence of colitis, and risk factors for recurrence included initial treatment with anti-PD-(L)1 inhibitors, re-challenge with anti-CTLA-4 inhibitors, higher grade of colitis, requirement for immunosuppressive therapy during initial colitis, and longer duration of initial colitis.63 Patients who do not experience an improvement of their symptoms in 3–5 days should be considered steroid-refractory and may benefit from treatment with a tumor necrosis factor (TNF)-α antagonist antibody, such as infliximab or vedolizumab, which block α₄β₇ integrin, resulting in gut-selective anti-inflammatory activity.64–66 Notably, evidence is emerging that early administration of infliximab or vedolizumab (<10 days after symptom onset) may be associated with more favorable outcomes in immune-mediated colitis, including fewer hospitalizations, less frequent steroid taper failures, shorter courses of steroids, and shorter duration of symptoms compared with later treatment.67 There are currently no head-to-head studies comparing infliximab with vedolizumab for the management of ICI-induced colitis.
Immune-modulating medications such as infliximab and vedolizumab may be problematic in patients with latent viral or bacterial infections. Infliximab, for example, has received a black box warning from the FDA due to the risk of reactivation in patients with latent tuberculosis (TB) infection. However, evidence suggests that patients with HIV may safely receive infliximab,68 and that patients with TB, HIV, and hepatitis B virus (HBV) may safely receive vedolizumab.69–71
Colitis frequently merits examination by methods such as colonoscopy, flexible sigmoidoscopy, and/or computed tomography (CT) scan. The diagnosis of immune-related colitis (without diarrhea) is typically based on histology. In cases where factors such as suspected bowel perforation or toxic megacolon exclude performing a colonoscopy, a CT scan is an effective, non-invasive alternative.72 ICI-induced colitis may be inflammatory and possibly ulcerative, and may appear in multiple locations and patterns in the colon. Histological analysis of biopsies may also reveal patterns of immune infiltration associated with chronic, acute, or lymphocytic colitis.73 A prospective study of 37 patients with ICI-induced colitis found that patients treated with anti-CTLA-4 ICIs exhibited enrichment of CD4+ T cells, while those treated with anti-PD-(L)1 ICIs exhibited enrichment of CD8+ T cells.74
A number of risk factors have been identified that may predict the development of diarrhea and colitis. The gut microbiome of the patient may influence colitis development, with patients enriched in the phylum Bacteroidetes less likely to develop ICI-associated colitis and patients enriched in bacteria of the phylum Firmicutes more likely to develop colitis (although Firmicutes was also associated with enhanced overall survival (OS) and progression-free survival (PFS)).75 76 Prior treatment with non-steroidal anti-inflammatory drugs (NSAIDs) also increases the risk of colitis.77 Patients with an existing history of GI autoimmune disorders, particularly inflammatory bowel disease, exhibit flare-ups in a substantial minority of cases as a result of ICI therapy (although they may develop other irAEs).78–82
Although rare, new-onset celiac disease has been reported after ICI therapy. The initial presentation of ICI-associated celiac disease shares several features with duodenitis, with the most common presentation being abdominal pain, vitamin deficiencies, dermatitis herpitiformis, transaminase elevations, and constitutional symptoms. Diagnosis was established by the presence of tissue transglutaminase antibodies (tTG IgA). Among the eight patients who presented with new-onset celiac disease after ICI, improvement in signs and symptoms (including down-trending tTG IgA) was observed after a gluten-free diet was implemented as the sole intervention.83
Hepatitis
In the context of ICI therapy, hepatitis is often asymptomatic and typically manifests as an elevation in alanine transaminase (ALT) and/or aspartate transaminase (AST) serum levels.84 Of note, other sources of elevated ALT/AST include muscle, so some centers add on CK measurement to make sure myositis/myocarditis is not being missed if values are elevated. Hepatic toxicities typically manifest 1–15 weeks after treatment, although as with any irAE they may occur after delays of months or years.29 60 Hepatitis (defined as ALT/AST elevation) occurs in 5% (1% grade ≥3) of patients treated with PD-(L)1 inhibitors, 5% (2% grade ≥3) of patients treated with CTLA-4 inhibitors, and in 19% (9% grade ≥3) of patients treated with combination ICIs.4 Infliximab should not be used in patients with liver injury, given the risk for hepatotoxicity.85 Owing to their use in non-ICI-mediated autoimmune hepatitis, immunomodulatory agents such as tacrolimus and mycophenolate mofetil have been suggested as treatments for steroid-refractory ICI-mediated hepatitis.86 Biopsy can be considered to initially diagnose steroid-refractory ICI-induced hepatitis, or to help identify the cause of steroid failure.
Cholecystitis and cholangitis
Cholecystitis and cholangitis are forms of hepatobiliary toxicity that are rarely associated with ICI therapy. A number of case reports have described isolated cases of each disease after ICI therapy.87 Due to a low number of total cases, however, it is difficult to estimate the incidence and causal relationship with immunotherapy, if any, of these irAEs. One case series that included >4000 patients estimated the incidence of suspected cholecystitis associated with any ICI as <1%88 and another retrospective analysis of medical records of 91 patients treated with nivolumab reported a cholangitis incidence of 3% (3 cases).89 Emerging evidence is suggesting that biliary complications may represent a distinct presentation associated with anti-PD-(L)1 therapy and that cholangiopathic irAEs may be more prone to steroid-refractoriness.90 91 Case reports have emerged of the successful use of tocilizumab to manage steroid-refractory biliary irAEs,92 93 however, due to relatively sparse data further studies are needed to determine true incidence rates and optimal interventions.
Pancreatitis
ICI therapy may cause elevated levels of lipase or amylase. However, diagnosis of acute pancreatitis as an ICI-related irAE is rare.94 The clinical diagnosis of pancreatitis requires at least two of three features to be present: elevated lipase to more than 3 times upper limit of normal (ULN), epigastric pain consistent with pancreatitis, and characteristic radiographic imaging.95 Because patients with elevated amylase or lipase are often otherwise asymptomatic for pancreatitis, few cases of ICI-related acute pancreatitis have been documented.94 Additionally, no association has been demonstrated between the degree of lipase elevation and the severity or prognosis of pancreatitis.
In a retrospective analysis of 2,279 patients monitored for lipase elevation, patients receiving anti-PD-(L)1, anti-CTLA-4, or combination ICI therapies exhibited grade ≥3 lipase elevation (ie, >2–5 times ULN with symptoms or >5 times ULN without symptoms) at rates of 4%, 2%, and 8%, respectively. Of the patients with grade ≥3 lipase elevation, 61% exhibited no other symptoms of pancreatitis, while 39% exhibited at least one other typical symptom of acute pancreatitis. The median time from ICI therapy initiation to peak measured lipase elevation was 146 days in patients treated with anti-PD-(L)1 therapy, 69 days in patients treated with anti-CTLA-4 therapy, and 110 days for patients treated with combination ICI therapy (p=0.03). In these cases, symptoms typically resolved to grade ≤1 within roughly 50 days, regardless of steroid usage. Risk factors for adverse outcomes resulting from acute pancreatitis (eg, chronic pancreatitis, diabetes) included longer duration of ICI therapy, history of smoking, and history of hyperlipidemia. The administration of intravenous (IV) fluids during acute pancreatitis was associated with better long-term outcomes, but for patients with grade 3 or 4 acute pancreatitis, the use of corticosteroids does not appear to improve outcomes and management should include consultation with a GI specialist.96
GI toxicity panel recommendations
The following recommendations are intended to be used within the framework of toxicity management, including direction for what grade of toxicity to hold and/or permanently cease treatment, considerations for life-threatening toxicities, as well as recommendations on optimal timing and dosing for administration of corticosteroids and/or other immunosuppressive agents by grade of AE, discussed in the General panel recommendations section. Any GI-specific exceptions or additional considerations to the general toxicity management principles are noted in the recommendations below.
Nausea
Patients who develop ICI-related nausea and vomiting of grade ≥2 should receive antiemetics (LE: 150 51). If no response to these therapies is observed within 5–7 days, esophagogastroduodenoscopy should be considered. Corticosteroids are not recommended for ICI-related nausea and vomiting.
Diarrhea and colitis
Diagnostic workup for grade 1 diarrhea or colitis symptoms should include CBC, CMP, and fecal lactoferrin.
Additional workup should be performed for patients with diarrhea or colitis symptoms of grade ≥2, and these additional tests should include fecal calprotectin, and stool infectious analysis (stool ova and parasite, C. difficile and cytomegalovirus (CMV) testing via polymerase chain reaction (PCR) if available or if high index of suspicion is present, among other infectious studies (eg, COVID-19)). Serum TSH and celiac serologies (antitransglutaminase antibodies with total IgA level) may also be considered, if clinical suspicion of ICI-induced celiac disease is present.
Abdominal CT scan should be obtained in patients with signs and symptoms of colitis complications, such as bowel perforation or toxic megacolon. Flexible sigmoidoscopy and/or colonoscopy with biopsy should be performed for patients with diarrhea or colitis symptoms of grade ≥3 or with persistent (≥5 days) diarrhea or colitis symptoms of grade 2 (LE: 472–74).
ICIs may be temporarily withheld (instead of discontinued) in patients experiencing grade ≥3 diarrhea or colitis symptoms. These patients may be re-challenged with ICIs if their symptoms are stable (grade ≤1 or baseline) with <10 mg/day of prednisone (or equivalent) (LE: 463).
Close monitoring for recurrence of diarrhea or colitis symptoms is recommended after re-challenging patients with ICI therapy.
Corticosteroids should be started in patients experiencing diarrhea or colitis symptoms of grade ≥2. The initial dose of prednisone should be 1 mg/kg/day (or equivalent) for grade 2 diarrhea or colitis and 1–2 mg/kg/day for grades 3 and 4. Grade 4 diarrhea or colitis should initially be treated with IV corticosteroids. Corticosteroids should be tapered within 4 weeks after improvement of diarrhea or colitis symptoms to grade ≤1 (LE: 161).
Prior to administration of infliximab or vedolizumab, patients should be tested for HBV, HIV, and TB. Administration of infliximab or vedolizumab should not be delayed if test results are pending.
If diarrhea or colitis symptoms do not respond to corticosteroid therapy within 3–5 days, if diarrhea or colitis symptoms recur after tapering corticosteroids, or if there is severe ulcerative presentation on colonoscopy, 3 doses of infliximab (5 mg/kg) should be administered at 0, 2, and 6 weeks (LE: 165) to reduce the risk of colitis recurrence.
If diarrhea or colitis symptoms persist after the second dose of infliximab treatment, the third dose should be held and 3 doses of vedolizumab (300 mg) should be administered at 0, 2, and 6 weeks (LE: 197).
If no clinical improvement is observed following immunosuppressive therapy in patients with grade ≥3 diarrhea or colitis, a repeat endoscopy with infectious workup (C. difficile and CMV) should be performed. Repeat endoscopy should be performed prior to resuming ICI therapy.
If diarrhea or colitis symptoms recur following corticosteroid taper, they should be evaluated and treated in the same manner as the first episode.
Hepatitis
Liver biochemical tests (aka liver function tests (LFTs)) should be checked prior to each ICI infusion. Diagnostic workup for grade ≥2 liver toxicity should include ALT, AST, alkaline phosphatase, prothrombin time/international normalized ratio (PT/INR) serum bilirubin, iron studies, autoimmune hepatitis panel (antinuclear antibody (ANA), antineutrophil cytoplasmic antibody (ANCA), antimitochondrial antibody (AMA), peripheral ANCA (p-ANCA), and antismooth muscle antibody (ASMA)), and viral hepatitis panel.
For patients experiencing liver toxicity of grade ≥3, abdominal imaging (eg, CT, magnetic resonance imaging (MRI), etc) should be considered if the patient has pre-existing liver disease or if there is concern of disease progression/liver metastases.
LFTs should be rechecked weekly for patients experiencing grade 1–2 liver toxicities, and should be rechecked every 1–2 days for patients with liver toxicities of grade ≥3.
Corticosteroids should be administered to patients experiencing liver toxicity of grade ≥2. Grade 2 liver toxicity should be treated initially with prednisone 0.5–1 mg/kg/day (or equivalent), and grades 3 and 4 should be treated initially with methylprednisolone 1–2 mg/kg/day (or equivalent). Corticosteroids should be tapered over a period of 4–6 weeks after LFTs revert to grade ≤1 (LE: 186).
If ALT or AST results do not improve to grade ≤1 within 10–14 days of corticosteroid initiation, or if liver toxicity recurs after steroid taper, mycophenolate mofetil (1–2 g divided two times per day) may be given (LE: 498). Infliximab should not be used in patients with liver toxicity, given the risk for hepatotoxicity (LE: 186 99). Other agents that could be considered include tacrolimus and antithymocyte globulin (ATG).
If ALT or AST results do not improve to grade ≤1 within 10–14 days of administration of mycophenolate mofetil, liver biopsy should be considered and possible CMV infection should be ruled out by PCR, if available.
Cholecystitis and cholangitis
Patients who develop ICI-related acute cholecystitis or cholangitis should not receive steroids and should instead receive typical treatments for these diseases. Diagnosis of these conditions should result in a patient being referred to a GI specialist and/or surgeon.
Pancreatitis
In patients with clinical symptoms of pancreatitis, workup for acute pancreatitis should include amylase, lipase, CBC, CMP, triglycerides, and abdominal CT scan. ICI therapy should be held if acute pancreatitis is confirmed until resolution of symptoms and CT findings.
Patients with persistent (>4 weeks) or recurrent symptoms of acute pancreatitis should receive repeat abdominal CT with contrast to evaluate for possible consequences of acute pancreatitis. These patients should also be evaluated for non-pancreatic etiologies of lipase or amylase elevation.
Patients with elevated lipase or amylase but no other symptoms of acute pancreatitis should be monitored closely for the development of acute pancreatitis but should continue on immunotherapy.
Prednisone (0.5–1 mg/kg/day) or equivalent may be considered in patients with acute pancreatitis if no improvement of symptoms occurs within 3–5 days of supportive treatment (IV fluids and analgesics). These patients should also be referred to a GI specialist.
Fatigue
Fatigue is a common AE that occurs both in response to ICI therapy and as a result of cancer.100 Fatigue is also frequently a symptom of other forms of ICI toxicity, including adrenal insufficiency, hypothyroidism, hypophysitis, hepatitis, renal insufficiency, pneumonitis, neurological toxicities, and anemia.101–108 Fatigue occurs in 21% (1% grade ≥3), 25% (2% grade ≥3), and 36% (4% grade ≥3) of patients treated with anti-PD-(L)1, anti-CTLA-4, and combination ICIs, respectively.4 Fatigue is most likely to occur after the first month following initiation of ICI therapy.109
Fatigue may be mechanistically linked to inflammation and is strongly influenced by a number of psychosocial factors such as history of depression or childhood adversity.110 111 Following the conclusion of ICI therapy, many patients report long-term fatigue.112 For patients experiencing cancer-related fatigue during or after treatment, evidence regarding pharmaceutical treatments is mixed.113–119 The available evidence is further complicated by significant placebo responses in clinical trials of medications for patients with cancer with fatigue.120 Non-pharmaceutical strategies such as exercise, psychological interventions, energy conservation and monitoring, and acupuncture are more strongly supported by clinical trial results.113 121–128
Fatigue panel recommendations
The following recommendations are intended to be used within the framework of toxicity management discussed in the General panel recommendations section, including direction for what grade of toxicity to hold and/or permanently cease treatment, considerations for life-threatening toxicities, as well as recommendations on optimal timing and dosing for administration of corticosteroids and/or other immunosuppressive agents by grade of AE. Any fatigue-specific exceptions or additional considerations to the general toxicity management principles are noted in the recommendations below.
Evaluation for patients with new or worsening ICI-related fatigue should include CBC, CMP, TSH, fT4, morning cortisol, and adrenocorticotropic hormone (ACTH).
If other organ-specific toxicities are ruled out, ICI-related fatigue should be managed similarly to cancer-related fatigue.
Patients with fatigue should also be evaluated for comorbidities that commonly cluster with fatigue, including pain, insomnia, depression, and anxiety.
Patients experiencing fatigue should be evaluated for comorbid conditions that may contribute to fatigue, including hypoxemia, obstructive sleep apnea, anemia, heart failure, liver insufficiency, renal insufficiency, reduced pulmonary function, electrolyte disturbance, thyroid dysfunction, adrenal insufficiency, nutritional deficiency, or sedating medications.
Management of fatigue may include non-pharmacological strategies such as energy conservation, energy-level diaries, moderate-intensity aerobic exercise, cognitive behavioral therapy, and nutritional evaluation, which have been shown to be helpful in cancer-related fatigue and are likely to be helpful for ICI-related fatigue (LE: 1120–122 124–128).
Skin toxicity
Dermatological toxicities are one of the most common categories of irAE. They are also one of the earliest to appear, at an average of 3–4 weeks after the start of treatment.29 The most common skin irAEs do not frequently reach grade ≥3 severity; however, more serious toxicities, including Stevens-Johnson syndrome/toxic epidermal necrolysis (SJS/TEN), bullous rashes, and toxic epidermal necrolysis have been reported in rare instances.129–133 Common manifestations of skin toxicities associated with ICI therapy are shown in figure 1.

Manifestations of immune checkpoint inhibitor (ICI)-associated skin toxicity. (A) bullous pemphigoid rash; (B) lichenoid dermatitis; (C) vitiligo; (D) pruritus; (E) psoriaform dermatitis; (F) maculopapular rash.
Rash
Patients treated with ICIs commonly develop rashes, although these rashes do not frequently rise to grade ≥3 severity. Patients develop rashes at a rate of 23% (1% grade ≥3), 10% (<1% grade ≥3), and 41% (5% grade ≥3) in response to therapy with anti-CTLA-4, anti-PD-(L)1, and combination ICI therapies, respectively.4 A variety of rashes have been recorded, including maculopapular, eczema or atopic dermatitis, lichenoid rash, blistering disorders, and pruritus or acneiform; all of these subtypes are often combined as “rashes” in reports of irAE incidence. Rash typically presents early in treatment, with onset from 2–5 weeks after first ICI treatment.134 Rash is often accompanied by pruritus.
Pruritus
Pruritus is a very common irAE, and often occurs in conjunction with rashes or other skin toxicities but may also present with no obvious skin lesions in 50% of cases. Treatment with anti-PD-(L)1, anti-CTLA-4, and combination ICIs is associated with pruritus rates of 15% (0% grade ≥3), 25% (1% grade ≥3) and 34% (2% grade ≥3), respectively.4 Management may include topical corticosteroids, oral antipruritics, and systemic immunomodulators. One retrospective analysis that included a total of 285 patients treated with ICIs across three centers and encompassing 427 skin irAEs found that most cases of pruritus (n=17) showed moderate to substantial improvement in symptoms after the administration of γ-aminobutyric acid (GABA) analogs pregabalin and gabapentin.135
Vitiligo
Vitiligo frequently presents concurrently with other irAEs, and especially with other skin irAEs. Vitiligo has been documented primarily in patients with melanoma,136 137 and appears to be associated with response to immunotherapy and survival in patients with melanoma.138 139 However, vitiligo in patients with other types of cancer has been reported, and it is possible that these cases are under-reported due to a lack of systematic skin evaluation outside of patients with melanoma.140–142 A systematic review found that patients treated with ipilimumab (anti-CTLA-4) developed vitiligo at a rate of 4%, those treated with nivolumab (anti-PD-1) at 9%, and those treated with pembrolizumab (anti-PD-1) at 6%.143
Uncommon skin toxicities
More uncommon, potentially severe or life-threatening cutaneous irAEs have been observed in patients treated with ICIs. These include pemphigus, pemphigoid, lichenoid rash, and SJS/TEN.144–146 Diagnosing and distinguishing between these irAEs may require the use of the salt-split skin technique on a skin biopsy sample, which uses skin separated between the epidermis and dermis to enable direct immunofluorescence analysis.147 Pemphigoid appears to be largely associated with anti-PD-(L)1 ICIs,136 148 149 and is less common with anti-CTLA-4 ICIs (primarily appearing in a small number of case reports).150 151 Pemphigoid occurs in an estimated 1% of patients receiving anti-PD-(L)1 therapy.148
SJS/TEN is rare and can be life-threatening, and SJS/TEN has been reported in patients treated with anti-PD-1 and anti-CTLA-4 inhibitors.131 152–154 SJS/TEN is accompanied by mucosal involvement (ocular, oral, or anogenital). SJS/TEN may be rapid and acute, or may appear progressively from a less severe skin toxicity, such as lichenoid eruptions that fail to respond to typical therapies.
Skin toxicity panel recommendations
The following recommendations are intended to be used within the framework of toxicity management, including direction for at what grade of toxicity to hold and/or permanently cease treatment, considerations for life-threatening toxicities, as well as recommendations on optimal timing and dosing for administration of corticosteroids and/or other immunosuppressive agents by grade of AE, discussed in the General panel recommendations section. Any skin-specific exceptions or additional considerations are noted in the recommendations below.
For patients with pruritus without rash, treatment with high-potency topical corticosteroids and GABA agonists may be considered (LE: 4135).
Workup for patients with potential ICI-related rash (grade <3) should include CBC with differential, CMP, assessment of the percentage body surface area involved by the rash, assessment of special features (eg, bullous formation, mucosal involvement), and patient history of allergy or atopy. Referral to a dermatologist should be considered.
Workup for patients with potential ICI-related rash (grade ≥3) should also include referral to a dermatologist and possible skin biopsy.
Rash with blisters, mucosal involvement, or bullous formation should trigger suspicion of lichenoid rash, pemphigus, pemphigoid, or SJS/TEN and follow-up testing, including skin biopsy with direct immunofluorescence studies and serum antibodies to desmogleins 1 and 3, bullous pemphigoid antigens 1 and 2, and indirect immunofluorescence studies in salt-split skin. ICI therapy should be interrupted until resolution or significant improvement of symptoms.
If ICI-related rash does not respond to topical or oral corticosteroids, is grade ≥3, or is intolerable, a dermatological consultation is recommended.
Grade ≥2 dermatological events (rash, pruritus) may recur after steroid taper. Therefore, a dermatological consultation or use of a steroid-sparing agent is recommended (rituximab for pemphigus (LE: 1155) or bullous pemphigoid (LE: 4156), dupilumab for eczema (LE: 1157), infliximab for lichenoid rash, and omalizumab for urticaria/pruritus (LE: 1158 159)).
Patients who have experienced grade 3 ICI-related rash may be re-challenged with ICIs. Rash that does not respond to immunosuppressive therapy should underscore the possibility of an infection and corresponding cultures should be obtained.
Musculoskeletal toxicity
Arthralgia
Arthralgia in numerous sites can occur during ICI therapy. In addition to being a toxicity induced by ICI therapy, arthralgia is also a known consequence associated with some cancers, chemotherapeutics, and radiation.160–163 This complicates the reporting and attribution of arthralgia, since it may be difficult to distinguish the source of arthralgia in the context of ICI cancer therapy. A systematic review reported arthralgia in 1%–43% of patients enrolled in ICI clinical trials.164 In some cases, arthralgia may be a symptom of a more serious inflammatory AE such as inflammatory arthritis.
Myalgias
Similar to arthralgia, it is difficult to accurately report on the incidence of ICI-induced myalgia, since myalgia can also occur due to cancer. Myalgia occurs in 2%–21% of patients participating in ICI clinical trials.164 Myalgias can be an isolated AE, or can be associated with inflammatory myositis.165 166
Arthritis
Inflammatory arthritis is an ICI-associated AE. Patients with ICI-associated arthritis have clinically heterogeneous presentations; some patients have symptoms that are similar to rheumatoid arthritis, others have psoriatic arthritis-like symptoms, and in some rare instances, there are symptoms of a reactive arthritis.164 167–170 In addition to arthralgia, arthritis may be accompanied by symptoms such as joint stiffness and swelling and can affect patients’ ability to perform activities of daily living. Synovitis, tenosynovitis, and/or enthesitis can be detected on physical examination. Patients are mostly seronegative for rheumatoid factor and anti-cyclic citrullinated peptide (anti-CCP) antibodies, but cases of seropositivity have been reported.169 171 172 In a systematic review of ICI-related inflammatory arthritis, 1%–7% of clinical trial participants developed arthritis.164
Polymyalgia rheumatica
Symptoms of ICI-induced polymyalgia rheumatica (PMR) include joint pain and stiffness (primarily in the shoulders and hips), and may rarely be accompanied by giant-cell arteritis (GCA), in which case visual symptoms must be assessed.173 174 Assessment of the incidence of PMR is difficult because the majority of studies of musculoskeletal irAEs are observational and retrospective. The median time to onset of PMR is 12 weeks, and the majority of cases respond well to corticosteroids.175 Patients with corticosteroid-refractory PMR may derive benefit from non-steroidal agents such as methotrexate, hydroxychloroquine, or tocilizumab.
Dry mouth and sicca syndrome
Dry mouth (or xerostomia) may occur as a separate irAE, or it may be a symptom of another irAE such as ICI-induced sicca syndrome.176 Dry mouth may also be linked to infections such as oral candidiasis—this is of particular concern in patients treated with ICIs, since oral corticosteroid use (commonly used to combat some ICI toxicities) is a risk factor for oral candidiasis.29 177 178 Dry mouth may be the cause of complications including infection and dental pathologies, including the loss of teeth, in severe cases of sicca syndrome.178 179 For this reason, it is important to account for the possibility of infection during diagnosis and monitoring. A systematic review determined that many clinical trials did not report the overall incidence of dry mouth, but that incidence varies from 3%–24% depending on the study.174 For initial management of dry mouth or painful sores, oral rinses with doxepin mouthwash or diphenhydramine-lidocaine-antacid mouthwash (sometimes called ‘magic mouthwash’) have been shown to reduce radiotherapy-related mucositis pain,180 181 but data are lacking on their efficacy in ICI-treated patients. Sialogogue therapy, cevimeline, pilocarpine, or other systemic acetylcholinergic agents have been anecdotally reported as helpful when symptoms are persistent and bothersome and refractory to topical mouth rinses.
ICI-induced sicca syndrome may feature severe symptoms, including dry eyes and dry mouth. Sicca accompanied by true Sjögren syndrome (typically with the presence of ANAs, anti-Ro, and/or anti-La antibodies) is rare, occurring at a rate of <1% in a registry study of grade ≥2 irAEs.167 The median time to onset of dry mouth, indicative of sicca syndrome, is 70 days. Patients who develop sicca syndrome often do not experience full resolution of their symptoms, and they may require long-term care for salivary hypofunction as well as being at risk for loss of teeth.176
Vasculitis
Vasculitis resulting from ICI treatment is a rare irAE and has been reported involving large vessels, medium vessels, small vessels, and the central nervous system.182 183 GCA, a type of large vessel vasculitis, has been seen with PD-(L)1 and CTLA-4 blockade and may be associated with PMR symptoms. No deaths have been attributed to ICI-induced vasculitis, and symptoms in each case resolved following withholding of ICIs and/or corticosteroid therapy. Induction with rituximab or cyclophosphamide have also been used in addition to steroids. Vasculitis typically occurs at a median of 3 months following initial ICI treatment.182 In those patients with suspected GCA, a low threshold for temporal artery biopsy in consultation with a rheumatologist and urgent corticosteroids may be warranted due to risk of visual loss.
Myositis
Myositis is a rare, potentially serious irAE, occurring in 1% of patients treated with anti-PD(L)1 ICIs and <1% of patients treated with anti-CTLA-4 ICIs.46 Little systematic data exist regarding the occurrence of myositis during treatment with other ICIs. Myositis is often associated with other serious muscular and neurological dysfunction, including myocarditis (9% of patients with ICI-associated myositis) and myasthenia gravis (9% of patients with ICI-associated myositis).46 Fatalities in patients with myositis may arise from associated irAEs such as myocarditis, or may occur directly as a result of myositis, particularly if there is diaphragmatic or respiratory muscle involvement. Symptoms of myositis include restricted eye movement, problems with speaking or swallowing, muscle weakness in the limbs, and myalgia. Some patients are asymptomatic, but exhibit elevated levels of CK. Conversely, some symptomatic patients present with normal CK levels. Myositis may require continued monitoring and/or follow-up treatment—in one analysis, 50% of myositis cases were ongoing or had resulted in sequelae at the end of the 5-year observation period.48
Musculoskeletal toxicity panel recommendations
The following recommendations are intended to be used within the framework of toxicity management, including direction for what grade of toxicity to hold and/or permanently cease treatment, considerations for life-threatening toxicities, as well as recommendations on optimal timing and dosing for administration of corticosteroids and/or other immunosuppressive agents by grade of AE, discussed in the General panel recommendations section. For suspected myositis, myocarditis, and myasthenia gravis, there is a possibility of overlapping symptoms, and therefore patients should be evaluated with a shared set of diagnostics, as described in more detail in the General panel recommendations section. Any additional musculoskeletal-specific exceptions or additional considerations are noted in the recommendations below.
Patients with grade ≥2 (or persistent) rheumatological irAEs such as inflammatory arthritis, PMR/GCA, vasculitis, myositis, or sicca syndrome should be referred to a rheumatologist for choice and interpretation of diagnostic testing as well as management recommendations.
Inflammatory arthritis and PMR
Initial diagnostic evaluation for patients with possible inflammatory arthritis should include ESR, CRP, rheumatoid factor, anti-CCP and ANA, and joint count and radiological investigation of the affected joint(s) where appropriate (with X-ray, MRI, or ultrasound) in consultation with a rheumatologist.
Initial diagnostic evaluation for possible PMR should include ESR and CRP.
Corticosteroid dosing for inflammatory arthritis and PMR may start at 10–20 mg/day of prednisone equivalents for grade 2 symptoms. For grade ≥3 symptoms, higher dosages of 40–60 mg/day of prednisone equivalents may be required (LE: 1184 185).
Treatments for patients with inflammatory arthritis that requires long-term treatment or does not respond to corticosteroids may include TNF-α inhibitors (eg, infliximab), methotrexate, leflunomide, hydroxychloroquine, sulfasalazine, or IL-6 receptor (IL-6R) inhibitors (eg, tocilizumab), depending on the circumstances (LE: 1186–190). Decisions regarding this medication selection depend on severity, comorbidities, and anticipated time to efficacy, and should be managed by a rheumatologist.
Dry mouth and sicca syndrome
Patients with possible sicca syndrome should consult with a rheumatologist, oral medicine specialist, or dentist.
Patients with grade ≥2 sicca syndrome may be treated with 20–40 mg/day of prednisone equivalents, subsequently tapered over 4–6 weeks (LE: 1191). An oral rinse containing dexamethasone may also be considered.
Myositis
Patients with possible myositis should consult with a rheumatologist or neurologist and be monitored for signs of myocarditis or myasthenia gravis.
Grade 1 myositis that presents with elevated CK and muscle weakness should be managed as grade 2. Oral corticosteroids may be offered as well as analgesia with acetaminophen or NSAIDs if no contraindications are present.
Patients with grade 3 myositis should be referred to a rheumatologist or neurologist. Hospitalization may be considered for severe weakness.
For patients with grade 3 myositis, ICIs should be held until myositis is grade ≤1 while off immune suppression and permanently discontinued if there is any evidence of myocardial involvement. Prednisone should be initiated at 1 mg/kg or equivalent.
For patients with grade 3 myositis and muscle weakness severely limiting mobility, cardiac or respiratory involvement, or dysphagia, 1–2 mg/kg of methylprednisolone IV or higher-dose bolus may be considered as well as plasmapheresis or intravenous immunoglobulin (IVIG) (LE: 3192).
If symptoms of myositis and CK levels do not improve or worsen after 4–6 weeks, other immunosuppressant therapy, such as methotrexate, azathioprine, or mycophenolate mofetil may be considered (LE: 3192). Rituximab has been used in primary myositis but caution is advised given its long biological duration.
Vasculitis
Evaluation for patients with suspected vasculitis should include CBC with differential, CMP, ESR, CRP, ANCA, serum complement (C3/C4), serology for viral hepatitis, serum cryoglobulins, urinalysis, and blood cultures (to rule out endocarditis).
Evaluation for vasculitis of grade ≥2 should include biopsy of the affected organ(s), or imaging through CT or MRI if biopsy is not possible.
Ophthalmological toxicity
The most common ocular irAEs are dry eyes and uveitis, but a number of additional pathologies have been reported, including neurological toxicities affecting the optic nerve and cranial nerves related to eye movement (eg, optic neuropathy), pathologies of the muscles surrounding the eye (eg, extraocular muscle myopathy), and other inflammatory events (eg, keratitis, orbitopathy).46 193–198 Untreated ocular toxicities may lead to vision loss, highlighting a need for prompt recognition and appropriate management. Ocular pathologies similar to ICI-induced irAEs may also arise as a result of cancer (eg, infections or metastasis to the eye or orbit) or pre-existing autoimmune disease.199
Dry eyes
Dry eyes may be an AE in their own right or may be a symptom of another AE such as sicca syndrome.168 The dry eye syndrome associated with ICI treatment may be severe enough to cause corneal perforation.200 The incidence of dry eyes in prospective trials ranges from 1%–24%.201
Uveitis
Uveitis typically presents with symptoms such as eye redness, pain, photophobia, floaters, and blurred vision.196 202 Uveitis induced by ICI therapy may be anterior, posterior, or panuveitis.203–209 Uveitis occurs at a rate of <1%–6% in clinical trials, based on a systematic review of the literature.201 It is important to note that symptoms of uveitis may not reflect the potential severity of the condition, and that uveitis can also occur as a result of infectious causes or metastasis to the eye. Therefore, a careful assessment is necessary to exclude other causes that require different treatment and to ensure proper management is initiated to prevent vision loss.210–212 Metastasis to the eye is especially concerning, since the eye is an immune-privileged site and could conceivably be difficult to treat with immunotherapies.212 Several steroid-sparing agents for non-infectious uveitis have been investigated outside of the context of ICI therapy, including methotrexate, mycophenolate mofetil (which did not demonstrate superiority to methotrexate),213 and secukinumab.214
Opthamological toxicity panel recommendations
The following recommendations are intended to be used within the framework of toxicity management, including direction for at what grade of toxicity to hold and/or permanently cease treatment, considerations for life-threatening toxicities, as well as recommendations on optimal timing and dosing for administration of corticosteroids and/or other immunosuppressive agents by grade of AE, discussed in the General panel recommendations section. Any opthamological-specific exceptions or additional considerations are noted in the recommendations below.
Ophthalmological consultation by a specialist is crucial for accurate and proper diagnosis, grading, and management. ICI-related ophthalmological AEs of note include dry eyes, uveitis, iritis, conjunctivitis, serous retinal detachment, and optic neuritis.
Eye symptoms of visual disturbance; red, painful, dry, or irritated eyes; double vision; droopy or puffy eyelids; and difficultly moving the eyes that are grade 1–2 in any patient undergoing immunotherapy should prompt the clinician to consider ophthalmological referral if available.
Eye symptoms of visual disturbance; red, painful, dry or irritated eyes; double vision; droopy or puffy eyelids; and difficultly moving the eyes that are grade ≥3 in any patient undergoing immunotherapy should prompt immediate ophthalmological referral.
If ocular or bulbar symptoms are present (eg, difficulty moving eyes), MRI of the brain (including pituitary cuts) should be conducted.
Initiation of systemic or topical treatment with corticosteroids for eye symptoms should occur under the guidance of an ophthalmologist, unless systemic steroids are needed for non-ophthalmological issues. Over-the-counter agents such as artificial tears may be used for symptom management as clinically appropriate.
Steroid treatment may worsen ocular conditions that are due to infection and can manifest with similar symptoms (eg, herpetic keratitis/uveitis) or may mask accurate diagnosis and grading when the patient is examined by an ophthalmologist.
Endocrine toxicity
It is notable that a number of endocrine toxicities persist even after therapeutic intervention for the irAE and the conclusion of ICI therapy, especially in the case of thyroid dysfunction. This is commonly attributed to permanent organ damage or impairment due to autoimmunity.215 216 It is also important to understand that, although rare, polyglandular endocrinopathies are possible, potentially complicating diagnosis and treatment.217–221
Hypothyroidism and hyperthyroidism
Hypothyroidism and hyperthyroidism are frequently asymptomatic or exhibit ambiguous symptoms, necessitating routine monitoring of parameters such as TSH and total T3/fT4 levels.222–224 Hypothyroidism is the more common of the two toxicities, occurring in about 8% of patients receiving anti-PD-(L)1 therapy, 3% of patients receiving anti-CTLA-4 therapy, and 15% of patients receiving combination ICI therapy. Grade ≥3 hypothyroidism is rare, occurring in roughly 0%–2% of patients receiving combination ICI therapies.4 The standard of care for the treatment of hypothyroidism is levothyroxine.225
Hyperthyroidism occurs less frequently, in 5% of patients treated with anti-PD-(L)1 inhibitors and 4% of patients treated with anti-CTLA-4 inhibitors.4 Rarely, ICI therapy may lead to Graves’ disease.226 Symptoms of elevated thyroid hormone may also appear transiently and evolve into hypothyroidism215 as a result of patients experiencing thyrotoxicosis during the course of thyroiditis, due to the destruction of thyroid follicles and necrosis.227 Hypothyroidism frequently occurs following this transient hyperthyroidism, as a sequela of ongoing thyroiditis—roughly 90% of patients who develop thyrotoxicosis do not recover full thyroid function, requiring long-term levothyroxine replacement. The median time to thyrotoxicosis is 5 weeks, and the median time to hypothyroidism is 10 weeks.215
Hypophysitis
Hypophysitis is an uncommon but important irAE, and is often accompanied by symptoms such as fatigue, nausea, vomiting, weakness, headache, and gonadotrophic deficiency (including loss of libido or erectile dysfunction).228 229 ICI-induced hypophysitis is most frequently manifested as secondary adrenal insufficiency due to ACTH deficiency, and less commonly due to TSH, follicle-stimulating hormone (FSH), and luteinizing hormone (LH) deficiency.216 230 Because hypophysitis can be induced through both ICI therapy and through the appearance of pituitary metastases, it is vital that a brain scan (preferably a pituitary-protocol MRI) be conducted to distinguish hypophysitis from alternative causes of headache, including brain metastases.231 Typical findings on MRI indicative of ICI-associated hypophysitis include geographic hypoenhancing lesions in the anterior lobe of the pituitary gland.232 It is further important to note that cortisol and ACTH test results may be inaccurate if patients are receiving steroids at baseline, for example, in patients with lung cancer treated with concurrent chemo and checkpoint inhibitors accompanied by dexamethasone premedication.
Hypophysitis occurs in 1% of patients treated with anti-PD-(L)1 ICIs and in 4% of patients treated with anti-CTLA-4 ICIs (0% and 2% grade ≥3, respectively).4 Patients receiving ICI combination therapy develop hypophysitis at a rate of 9%–11%.233 In an analysis of 689 patients who developed ICI-related hypophysitis, the median time between ICI treatment initiation and diagnosis of hypophysitis was 76 days.234
Primary adrenal insufficiency
Rarely, in addition to secondary adrenal insufficiency caused by disruption of the pituitary gland, irAEs have been noted in which the adrenal glands are directly damaged following ICI therapy, leading to primary adrenal insufficiency.235 As with secondary adrenal insufficiency, primary adrenal insufficiency can lead to life-threatening adrenal crisis due to vasodilatory shock.236 The symptoms of adrenal insufficiency, like other endocrinopathies, can be non-specific and difficult to diagnose without additional testing. Symptoms may include, nausea, loss of appetite, weight loss, fatigue, light-headedness, hypoglycemia, and hypotension.236–238 Primary adrenal insufficiency is rare in ICI-treated patients and would be associated with high serum ACTH levels in conjunction with low morning serum cortisol.101 However, morning cortisol and ACTH levels are not always definitive—an ACTH stimulation test is considered the standard of care assessment for adrenocortical insufficiency.
Adrenal insufficiency is not a common ICI-associated irAE, but it necessitates vigilance and close monitoring due to the possibility of adrenal crisis. Adrenal insufficiency occurs in 1% of patients treated with anti-PD-(L)1 or CTLA-4 therapies, and is estimated to occur at a rate of 5% in patients treated with combination ICIs.4 233 In a review of case reports, the median onset of adrenal insufficiency measured from the first dose of ICI therapy was 10 weeks.235
Type I diabetes mellitus
Type I diabetes mellitus (T1DM) induced by ICI therapy is rare, but frequently serious. The incidence of ICI-induced diabetes is estimated at approximately 1%.239 240 T1DM may develop shortly after the beginning of ICI treatment or as much as 1 year following the start of treatment.241 242 Diabetes occurs at a rate of <1%–2% in patients treated with anti-PD-(L)1 inhibitors.233 Diabetes has occurred in patients treated with anti-CTLA-4 inhibitors, but this is a very rare occurrence.243 Often, the initial presentation is fulminant T1DM and diabetic ketoacidosis (DKA). However, patients may be asymptomatic or present with symptoms such as fatigue, nausea, vomiting, weight loss, polyuria, or polydipsia.241 243 Autoantibodies indicative of T1DM are found in up to 53% of cases, with the majority being anti-glutamic acid decarboxylase (GAD-65) antibodies,244 although insulin autoantibodies have also been reported.240 Almost all patients with T1DM require insulin therapy for management.
Endocrine toxicity panel recommendations
The following recommendations are intended to be used within the framework of toxicity management, including direction for at what grade of toxicity to hold and/or permanently cease treatment, considerations for life-threatening toxicities, as well as recommendations on optimal timing and dosing for administration of corticosteroids and/or other immunosuppressive agents by grade of AE, discussed in the General panel recommendations section. Any endocrine-specific exceptions or additional considerations are noted in the recommendations below.
Patients experiencing endocrine toxicities should be treated with hormone replacement, and immunotherapy should generally be continued as soon as patients are stable (often without interruption). Management of thyroid toxicities and T1DM generally do not require the use of corticosteroid therapy.
Hypothyroidism and hyperthyroidism
Thyroid function (TSH, fT4) should be tested every 4–6 weeks during ICI treatment, and should continue to be tested every 6–12 months following the conclusion of ICI treatment.
Patients with elevated TSH and normal fT4 should receive repeat TSH and fT4 testing routinely, and if this pattern persists without hypothyroidism symptoms then levothyroxine treatment should be considered. Levothyroxine should be administered to patients with hypothyroidism at 1.5–1.6 μg/kg/day for young, healthy patients, and should be administered at 25 or 50 μg/day for patients >65 years of age or with heart disease.
Patients with symptoms of hypothyroidism and/or with elevated TSH and low fT4 should be tested for morning cortisol to identify possible concurrent adrenal insufficiency.
Patients with low TSH and normal fT4 should receive repeat TSH and fT4 testing routinely, and if symptoms of hyperthyroidism or high fT4 develop patients should be treated with beta-blockers. Patients with asthma or chronic obstructive pulmonary disease should be treated with cardioselective beta-blockers such as atenolol or metoprolol.
Patients with persistently low TSH and high fT4 should be evaluated for hyperthyroidism and Graves’ disease etiology.
Hypophysitis
Patients with low TSH and normal or low fT4 should be tested for ACTH levels and morning cortisol to identify possible hypophysitis.
Patients with low ACTH levels and low morning cortisol should be tested for FSH, LH, TSH, fT4, and sex hormones to evaluate possible hypophysitis.
If symptoms of acute hypophysitis are observed, immunotherapy should be interrupted and corticosteroids administered (LE: 4245).
Patients with hypophysitis should receive replacement hydrocortisone at 10–12 mg/m2/day.
Patients on hydrocortisone therapy should be encouraged to have a medical alert device, and the patient and caregivers should be educated on the possibility of stress doses of steroids (administered during hospitalization or severe illness), emergency use of parenteral dexamethasone or hydrocortisone.
Adrenal insufficiency
Patients with suspected primary adrenal insufficiency should be tested for AM cortisol and CMP in addition to ACTH stimulation testing.
If adrenal insufficiency of any grade is diagnosed, immunotherapy should be temporarily withheld and steroid replacement therapy should be started.
Patients with adrenal insufficiency should be monitored for signs of adrenal crisis, such as hemodynamic instability.
For patients who develop adrenal insufficiency, a medical alert bracelet should be provided.
Type I diabetes mellitus
Patients with new-onset diabetes (type I) should be tested for hemoglobin A1c, C-peptide, autoantibodies and counseled on diabetes management, including diet and lifestyle changes, glucose monitoring, and insulin treatment. If patients experience severe hyperglycemia or DKA on ICIs, they should be hospitalized.
Patients with hyperglycemia should be evaluated for DKA and ICIs should be held until DKA is resolved.
Neurological toxicity
In a systematic review of neurological irAEs, overall incidence for patients treated with anti-PD-(L)1, anti-CTLA-4, and ICI combinations was measured at 6%, 4%, and 12%, respectively. However, the majority of these irAEs were non-specific, grade 1 or 2 events. The incidence of events grade ≥3 in this review of the literature was below 1% for all neurological irAEs.246 Another single-institution study found an incidence of 1.5%, with 28 patients with neurological irAEs grade ≥3 among 1,834 patients treated with ICIs over a 6-year period.247 Neurological irAEs have the potential to be fatal or to cause lasting (sometimes permanent) impairment of neurological function.46 248 249 The symptoms of neurological irAEs are frequently overlapping and may be ambiguous. Additionally, toxicity may involve the peripheral nervous system or the central nervous system. For example, both myasthenia gravis and peripheral neuropathy may involve muscle weakness, a symptom shared with other irAEs such as myositis. Neurological irAEs typically occur within the first 3 months after starting ICIs.46 192
Myasthenia gravis
Myasthenia gravis is a significant neurological toxicity with a high potential for patient fatality.46 193 Patients present with fatigable or fluctuating muscle weakness, generally involving proximal muscles (neck and shoulder) more than distal muscles. There may be diaphragmatic weakness resulting in respiratory compromise. Bulbar and ocular muscles are commonly affected in myasthenia gravis resulting in ptosis, extraocular movement abnormalities leading to double vision, facial weakness, and difficulty swallowing. Autoantibodies against the acetylcholine receptor (AChR) or MusK may be present in ICI-related myasthenia gravis, but toxicity can occur independent of positive serology. One retrospective analysis that included 47 total patients with ICI-related myasthenia gravis reported serological positivity rates by anti-AChR antibody and anti-MuSK antibody of 66.7% (30/45) and 5.3% (1/19), respectively.250 Patients with myasthenia gravis may also develop myocarditis and/or myositis as part of a potentially dangerous combination of pathologies.46 251 Patients treated with anti-PD-(L)1 ICIs are at greater risk of developing myasthenia gravis than patients treated with anti-CTLA-4 ICIs.46 The standard of care for myasthenia gravis includes IVIG and plasma exchange (PLEX), and in patients with autoimmune myasthenia gravis also includes high-dose pulse corticosteroids.252–254
Encephalitis
ICIs may result in encephalitis at an incidence estimated to be <1%. Patients may present with a wide range of symptoms including altered behavior, confusion, short-term memory impairment, agitation, speech abnormality, and seizures. Treatment with anti-PD-(L)1 monotherapies or with combination ICIs is associated with a higher risk of encephalitis compared with treatment with anti-CTLA-4 ICIs.46 Rarely, patients have been found to have positive autoimmune encephalitis or paraneoplastic neurological syndrome antibodies.255–257
Peripheral neuropathy
Peripheral neuropathies may be observed in a number of different phenotypic presentations, including painful small fiber sensory type and cranial neuropathies,258 259 as well as sensorimotor presentations more typical of classic immune-mediated phenomena, such as Guillain-Barré syndrome.46 260 Guillain-Barré syndrome is more common in patients treated with anti-CTLA-4 or combination anti-CTLA-4 plus anti-PD-1 ICIs when compared with patients treated with anti-PD-(L)1 ICIs alone.46 Guillain-Barré syndrome, or ascending polyradiculoneuropathy, can develop soon after ICI treatment is started, usually within the first 3 cycles. Patients may develop early lower back or thigh pain followed by ascending weakness, sensory loss, and areflexia as the main symptoms. Facial weakness and extraocular movement impairment as a result of cranial neuropathies may occur. There may also be dysregulation of autonomic nerves. Nerve root enhancement and thickening may be seen on imaging.
Patients may develop other acute neuropathies, including painful sensory neuropathy and isolated cranial mononeuropathies, especially of the facial and abducens nerves.258 Patients with painful neuropathies may require pain management.
Aseptic meningitis
Patients may present with headache, neck stiffness, photophobia, low-grade fever, and nausea. Typically, mental status is normal in these patients (in contrast with encephalitis). As with any case of meningitis, the possibility of infectious meningitis must be seriously considered during diagnosis and treatment and leptomeningeal metastasis should also be ruled out. Patients with headache should also have hypophysitis ruled out. Meningitis is associated more frequently with anti-CTLA-4 and anti-CTLA-4 plus anti-PD-(L)1 combination therapies than with anti-PD-(L)1 monotherapies.46
Neurological toxicity panel recommendations
The following recommendations are intended to be used within the framework of toxicity management, including direction for at what grade of toxicity to hold and/or permanently cease treatment, considerations for life-threatening toxicities, as well as recommendations on optimal timing and dosing for administration of corticosteroids and/or other immunosuppressive agents by grade of AE, discussed in the General panel recommendations section. For suspected myositis, myocarditis, and myasthenia gravis, there is a possibility of overlapping symptoms, and therefore patients should be evaluated with a shared set of diagnostics, as described in more detail in the General panel recommendations section. Any other neural-specific exceptions or additional considerations are noted in the recommendations below.
Patients diagnosed with neurological irAEs should be referred to a specialist, regardless of severity.
Patients with ocular myasthenia of grade ≤2, non-Guillain-Barré polyneuropathy of grade ≤2 (LE: 2261–263), or aseptic meningitis (LE: 4264–266) of any grade should receive 0.5–1 mg/kg/day of prednisone or equivalent depending on severity.
Patients with any grade of encephalitis or Guillain-Barré syndrome should receive pulse-dose methylprednisolone at 1000 mg IV daily for 3–5 days, and should additionally receive IVIG or PLEX.252–254
Patients with any grade of myasthenia symptoms should have a neurology consultation. Workup should include diagnostic antibody testing for myasthenia gravis and evaluation for concurrent myositis, myocarditis, and thyroid dysfunction. Electrodiagnostic studies may be performed to distinguish myasthenia gravis from myositis. Pulmonary function should be assessed with negative inspiratory force (NIF) and vital capacity (VC).
Workup for patients with suspected aseptic meningitis should include MRI of the brain and pituitary with and without contrast, lumbar puncture (LP), cortisol, and ACTH.
Patients with suspected aseptic meningitis should receive antibiotics until bacterial meningitis can be ruled out.
Workup for patients with suspected encephalitis should include MRI of the brain, LP, CBC, CMP, autoimmune encephalopathy and paraneoplastic panels of blood and cerebrospinal fluid (CSF), PCR for infectious encephalitis, thyroid panel, and electroencephalogram (EEG).
If ICI-related encephalitis does not respond to pulse-dose corticosteroids, patients may receive IVIG (2 g/kg in divided doses over the course of 5 days), PLEX (one session every other day for 5–7 cycles), or rituximab (375 mg/m2 weekly infusion for 4 weeks) (LE: 1253).
Patients with suspected ICI-related encephalitis should receive empirical antiviral treatment until viral encephalitis can be ruled out.
Workup for patients with suspected Guillain-Barré syndrome should include MRI of the spine to rule out a compressive lesion, LP, EMG, nerve conduction studies, and ganglioside antibody panel of blood and CSF.
Patients diagnosed with Guillain-Barré syndrome should always permanently discontinue ICI therapy, and should receive IVIG or PLEX with corticosteroid therapy (LE: 1254). These patients should receive frequent pulmonary assessments.
Workup for patients with (non-Guillain-Barré) suspected peripheral neuropathy should include MRI of the spine, EMG nerve conduction, and blood work including B12, serum protein electrophoresis (SPEP), hemoglobin A1c, B6, ESR, CRP, and folic acid.
Patients diagnosed with painful peripheral neuropathy should receive neuropathic pain medication such as gabapentin, pregabalin, or duloxetine until neuropathy resolves (LE: 1267–269).
If ocular or bulbar symptoms are present, MRI of the brain should be conducted.
Patients diagnosed with myasthenia gravis should discontinue ICI therapy and should receive IVIG or PLEX with corticosteroid therapy and pyridostigmine. These patients should receive frequent pulmonary assessments (LE: 1252). For patients with grade 2 myasthenia gravis, in addition to consultation with neurology and discontinuation of ICI, corticosteroids should be administered (prednisone, 1–1.5 mg/kg oral or equivalent daily) and tapered based on symptom improvement. Pyridostigmine may be considered, starting at 30 mg orally three times a day and gradually increase to a maximum of 120 mg orally four times a day as tolerated and based on symptoms (LE: 1252).
Patients with grade 3 or 4 myasthenia gravis should be admitted to the hospital and may need ICU-level monitoring. ICIs should be permanently discontinued, and frequent pulmonary function assessments and daily neurological review should be performed. Corticosteroids should be continued (LE: 3252). Additionally, IVIG 2 g/kg over 5 days (0.4 g/kg/day) or plasmapheresis for 5 days may be considered.
Pulmonary toxicity
The term ‘pneumonitis’ can refer to a number of disease states involving inflammation of the lung tissue.270 In some clinical trials, pneumonitis is used as a blanket term to describe nearly any pulmonary toxicity, which can include related pathologies such as interstitial lung disease (ILD), while in other trials pneumonitis has a more specific definition. Pre-existing interstitial lung abnormalities are risk factors for the development of ICI-induced ILD.271 For the purposes of this manuscript, pneumonitis is defined broadly as lung tissue inflammation.
Pneumonitis
Pneumonitis is a relatively common irAE that is associated with lower rates of patient survival.102 272 Symptoms include dyspnea, persistent cough, chest pain, fever, and hypoxia (potentially leading to respiratory failure).273 Patients with pneumonitis may also be asymptomatic, yet show detectable inflammation on CT scan.273 274 Radiological findings with ICI-associated pneumonitis may vary, with distinctive features seen on imaging, including discrete patchy or confluent consolidation with or without air bronchograms and predominantly peripheral or subpleural distribution, ground-glass opacities, centrilobular nodules, bronchioloitis-like appearance with tree-in-bud micronodularity or patterns that do not clearly fit within other classifications.273 Characteristic CT scans showing common presentations of ICI-associated pneumonitis are shown in figure 2.

{kind=link}
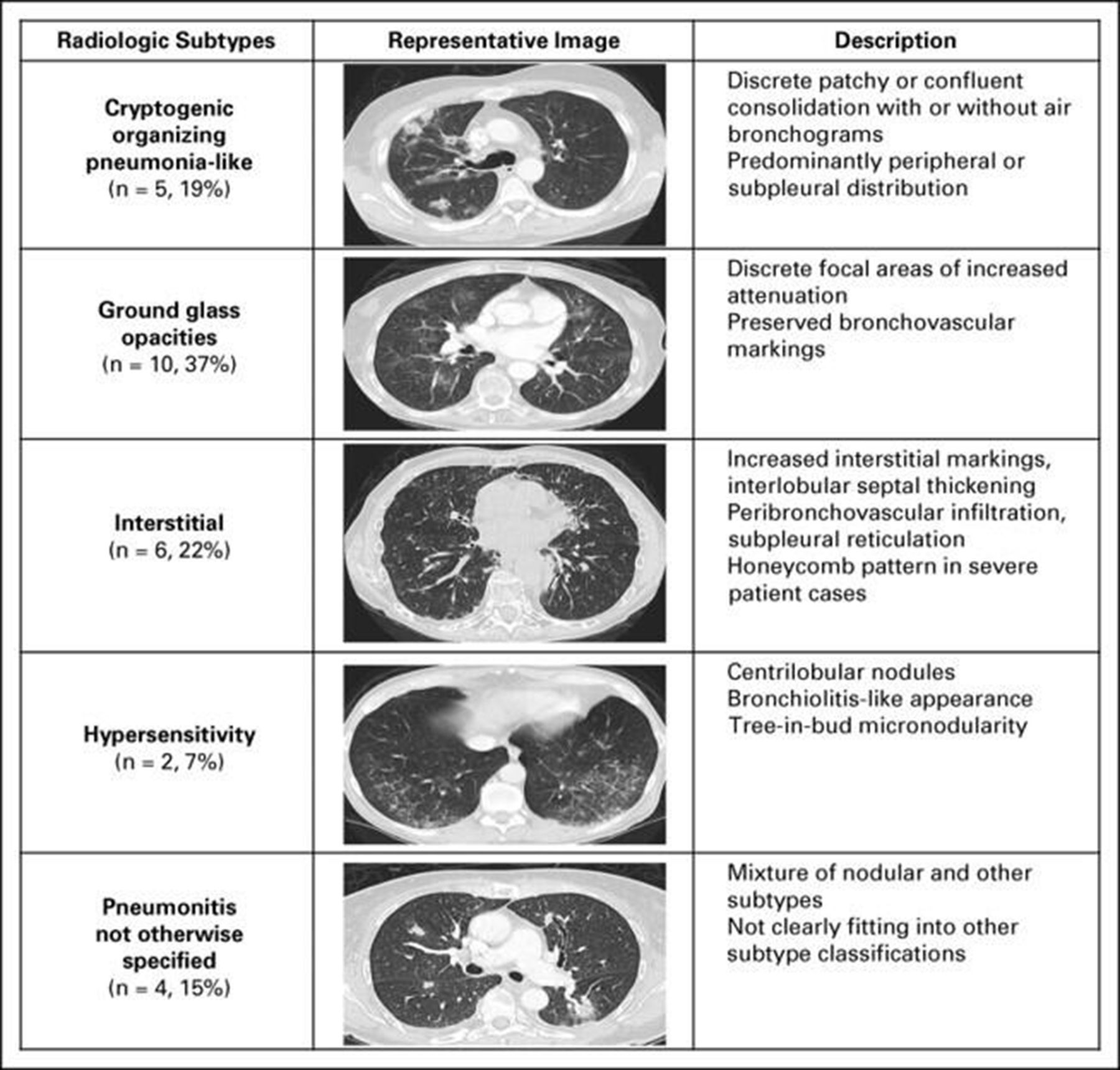{kind=link}
Manifestations of ICI-associated pneumonitis. Radiological features of pneumonitis associated with anti-programmed cell death protein-1/programmed death-ligand 1 therapy stratified into five distinct phenotypes. (From Naidoo et al273, JCO, 2017)
Pneumonitis is associated with the expansion of inflammatory T cell subsets, in both bronchoalveolar lavage samples and from direct tissue samples of pneumonitis-related lesions.275 276 In published meta-analyses, patients with NSCLC or renal cell carcinoma (RCC) have a higher risk of developing pneumonitis compared with patients with melanoma following treatment with PD-(L)1 inhibitors.277 Recent literature indicates that a history of asthma and/or smoking may predispose patients to developing higher grade pneumonitis with ICI therapy.278 Other risk factors that influence the incidence of ICI-associated pneumonitis include prior curative-intent radiotherapy and squamous tumor histology.279 280 Pneumonitis that does not improve with corticosteroid treatment may also be more common in patients who are former or active smokers, or those who have underlying lung conditions.273
Pneumonitis occurs in 4% of patients receiving PD-(L)1 inhibitors (1% grade ≥3) and 1% of patients receiving anti-CTLA-4 therapy (1% grade ≥3).4 The rate of pneumonitis in patients treated with combination ICIs is significantly higher than the rate for patients treated with ICI monotherapies, at 7% (2% grade ≥3).277 A systematic review also determined that PD-1 inhibitors cause pneumonitis at a higher rate than PD-L1 inhibitors in patients with NSCLC.281 Notably, the incidence of pneumonitis recorded in clinical trials may be lower than that observed in routine clinical practice. A retrospective study at a single institution recorded an incidence of 19%, with 12% of patients experiencing pneumonitis of grade ≥3.280 An analysis of ICI-treated patients that developed pneumonitis found that the median onset of pneumonitis is 3 months, and in one clinical trial the median time to resolution of symptoms was 3–4 weeks.273 282
Recurrent pneumonitis following improvement of symptoms has been observed both in patients who were re-challenged with ICI therapy and in patients who were not, demonstrating the need for careful monitoring of all patients with ICI-induced pneumonitis after resolution of symptoms. In a small sample of patients who were re-challenged with ICI therapy following complete clinical resolution of pneumonitis (n=12), 25% developed recurrent pneumonitis that resolved by reinstating the same initial intervention: withholding of ICIs (grade 1) and/or corticosteroid treatment (grade 2).273 In recent studies, pneumonitis has also been found to assume a chronic course in approximately 2% of patients with NSCLC or melanoma treated with ICIs.283 Patients with steroid-refractory ICI-induced pneumonitis may benefit from mycophenolate mofetil or high-dose IVIG (hdIVIG), although this has only been reported in case studies.280 284 Based on its application in other immune-mediated lung diseases, cyclophosphamide might also be expected to provide benefit in steroid-refractory pneumonitis.285 286 However, little data exist that directly tests the use of cyclophosphamide in this treatment context. One study of 120 patients with chronic hypersensitivity pneumonitis (CHP) found that those who were able to tolerate a full course of infusions with cyclophosphamide (6 infusions at 600 mg/m2) appeared to stabilize in their decline in lung function.287 Other approaches that have been reported include anti-cytokine agents. Infliximab (5 mg/kg, IV) has been used to treat patients with ICI-induced pneumonitis, with mixed results from a number of case reports.273 288–290 A study of the IL-6R antagonist antibody tocilizumab (4 mg/kg, IV) for the treatment of nivolumab-associated irAEs also showed potential benefit in the setting of grade ≥3 pneumonitis.291 An ongoing prospective study through ECOG-ACRIN will compare the efficacy of IVIG versus infliximab for steroid-refractory pneumonitis (NCT04438382).
Sarcoidosis
Due to the rarity of ICI-associated sarcoidosis, it is difficult to definitively assess the incidence of this irAE.292 However, it is important that clinicians recognize the possibility of sarcoidosis, since the formation of granulomas associated with this irAE may resemble disease progression or recurrence.292 293 Sarcoidosis may arise in a number of sites within the body, most commonly the lymph nodes (71% of cases), lungs (60% of cases), and skin (55% of cases). Sarcoidosis occurs at a mean of 9 months following the start of ICI treatment, and symptoms resolve in a mean of 4 months.292 Because sarcoidosis is usually asymptomatic and may mimic progressive disease, especially with lymph node involvement, biopsy may be considered in the differential.
Pulmonary toxicity panel recommendations
The following recommendations are intended to be used within the framework of toxicity management, including direction for at what grade of toxicity to hold and/or permanently cease treatment, considerations for life-threatening toxicities, as well as recommendations on optimal timing and dosing for administration of corticosteroids and/or other immunosuppressive agents by grade of AE, discussed in the General panel recommendations section. Any pulmonary-specific exceptions or additional considerations are noted in the recommendations below.
Patients with pre-existing autoimmune ILD should be referred to a specialist where possible before initiation of ICI therapy for the consideration of pulmonary function tests (PFTs) and risk assessment (LE: 3271).
Patients with suspected pneumonitis should be examined via high-resolution CT of the chest. If the CT scan is negative, PFTs should be considered to identify a potential functional deficit (LE: 4273).
If PFTs are indicated, they should include spirometry and diffusing capacity of the lungs for carbon monoxide (DLCO).
Patients experiencing grade 2 pneumonitis should receive 1–2 mg/kg/day prednisone (or equivalent), tapering over 4–6 weeks. For pneumonitis of grade ≥3, patients should receive 1–2 mg/kg/day methylprednisolone IV or equivalent, tapering over 4–6 weeks (LE: 3294).
If high-dose corticosteroid therapy does not improve pneumonitis symptoms within 72 hours (or if symptoms are life-threatening), options include (in no particular order) mycophenolate mofetil (1–1.5 g two times per day, tapering in consultation with a pulmonary specialist (LE: 3295 296)), hdIVIG (2 g/kg in divided doses over 2–5 days, per institutional guidelines (LE: 4284)), infliximab (5 mg/kg, one dose with optional repeat 14 days later (LE: 4273 288–290)), cyclophosphamide (LE: 3285), or tocilizumab (LE: 4291).
If patients have experienced grade 2 pneumonitis, they may be re-challenged with ICIs upon complete resolution of symptoms. These patients should be monitored through more frequent consultations with their physician (LE: 4273).
Infusion reactions
Infusion reactions are relatively infrequent for the majority of ICIs, typically occurring in <10% of patients. Infusion reactions occur in 4% of patients treated with anti-PD-(L)1 inhibitors and in 2%–6% of patients treated with ipilimumab, depending on the infusion regimen used.58 297 A systematic review found that all patients treated with anti-PD-1 or anti-PD-L1 ICIs developed infusion reactions of grade ≥3 at a rate of <1%, those treated with anti-PD-L1 ICIs specifically at 2%, and those treated with anti-CTLA-4 or combination ICIs at 0%.298 However, avelumab causes a markedly higher incidence of infusion reactions compared with other ICIs, in the range of 21%–29% (0%–3% grade ≥3).137 299 While this difference may be due to unique features of avelumab in comparison to other ICIs, it may also be due to differences in the definition of infusion reactions in the safety analyses of clinical trials examining avelumab. For example, a pooled safety profile of patients enrolled in two clinical trials aggregated all infusion reactions, drug hypersensitivity, hypersensitivity reactions, signs and symptoms of infusion reactions occurring on the same day or the day after infusion, and possible signs and symptoms of infusion reactions occurring on the day of infusion into the category of infusion reactions.300 Treatment with nivolumab may also result in a higher incidence of infusion reactions when administered to patients with Hodgkin lymphoma, from 14%–20% incidence (0% grade ≥3).301
Infusion reactions are typically short-lived. The time frame of infusion reaction onset is typically immediate (during infusion) to up to 1 hour post-infusion. Symptoms of infusion reactions include chest tightness, cough, wheezing, rigors, back pain, tongue swelling, dizziness, rash, pruritus, fever, dyspnea, angioedema, tachycardia, hypotension or hypertension, and, rarely, anaphylaxis. While infusion reactions are typically not severe and rarely exceed grade 2, more serious reactions can be potentially fatal, especially when anaphylaxis is present. While specific data regarding treatment of ICI-related infusion reactions are limited, protocols for the general management of infusion reactions to monoclonal antibodies (of which ICIs are a subset) are applicable.302
Infusion toxicity panel recommendations
The following recommendations are intended to be used within the framework of toxicity management, including direction for at what grade of toxicity to hold and/or permanently cease treatment, considerations for life-threatening toxicities, as well as recommendations on optimal timing and dosing for administration of corticosteroids and/or other immunosuppressive agents by grade of AE, discussed in the General panel recommendations section. Any infusion reaction-specific exceptions or additional considerations are noted in the recommendations below.
If a patient experiences an infusion reaction, the infusion should be stopped for at least 30 minutes and supportive medications (including steroids, antihistamines, and beta-agonists) should be administered. Following this, the infusion may be restarted for reactions that were grade ≤2.
If a patient has experienced a prior infusion reaction, premedication (eg, corticosteroids, NSAIDs, antihistamines) should be used to mitigate possible reactions during subsequent infusions.
If a patient has experienced an infusion reaction to an ICI, switching to another ICI (that is approved for use in the same indication) may be considered to reduce the likelihood of subsequent infusion reactions.
Renal toxicity
Like pulmonary toxicities, renal toxicities can appear as a wide variety of pathologies that exhibit highly overlapping symptoms, although tubulointerstitial nephritis (TIN) is the most common.104 303 Typically, TIN manifests as reduced renal function, indicated by rising serum creatinine (Cr), low-grade proteinuria, and sterile pyuria in roughly 50% of cases. Rarely, ICIs lead to the development of glomerular disease. Patients who develop minimal change disease, focal segmental glomerulosclerosis, or membranous nephropathy often present with nephrotic syndrome. Conversely, patients with nephritic lesions (eg, pauci-immune crescentic glomerulonephritis (GN) due to ANCA vasculitis) present with hematuria, subnephrotic proteinuria, and impaired renal function.104 303–305
Acute kidney injury
Acute kidney injury (AKI) describes a condition in which kidney function is severely impacted or lost and may occur via a number of etiologies including prerenal disease, acute tubular necrosis, TIN, autoimmune reactivation of membranous nephropathy, and glomerular diseases.104 304 306–308 AKI can be graded using the CTCAE scale but may also be graded with the Kidney Disease: Improving Global Outcomes (KDIGO) criteria, which defines AKI through the specific criteria of serum Cr levels and urine output, as opposed to the more vague criteria outlined in the CTCAE.309 The KDIGO criteria may enable more detailed classification of kidney disease, since KDIGO stages disease severity using both elevation above baseline and absolute thresholds in serum Cr levels, while the CTCAE only measures based on elevation above baseline.309 310 However, the majority of clinical trials use the CTCAE scale of severity, which may result in underestimation of the rate of AKI. Furthermore, AKI is common in patients receiving ICI therapy, but in most cases, it is not the direct result of ICI toxicity. It is important to differentiate between all-cause AKI (eg, due to hypovolemia or acute tubular necrosis (ATN)) and ICI-induced AKI to ensure appropriate management.311 With these limitations in mind, the recorded incidence of ICI-induced AKI in patients from pooled clinical trials receiving anti-PD-(L)1 ICIs was 2% and the incidence for patients receiving ipilimumab was 2%.304 312 Combination therapy with anti-PD-(L)1 and anti-CTLA-4 ICIs resulted in an AKI incidence of 5%.304 The majority of TIN cases are steroid responsive. Patients with steroid-refractory TIN may benefit from mycophenolate mofetil, based on its efficacy in non-ICI-induced cases of interstitial nephritis.313–315 Other options, including rituximab, have been explored for some glomerular and renal vasculitis diseases.308 316
Renal toxicity panel recommendations
The following recommendations are intended to be used within the framework of toxicity management, including direction for at what grade of toxicity to hold and/or permanently cease treatment, considerations for life-threatening toxicities, as well as recommendations on optimal timing and dosing for administration of corticosteroids and/or other immunosuppressive agents by grade of AE, discussed in the General panel recommendations section. Any kidney-specific exceptions or additional considerations are noted in the recommendations below.
Patients with possible ICI-related AKI should have a urinalysis and quantification of proteinuria with a spot urine protein:Cr ratio. It should be noted that normal urinalysis does not exclude TIN.
In cases of AKI with no clear alternative etiology, TIN should be suspected. Less commonly, ICI therapy can also cause glomerular lesions, which should be suspected in the setting of an active urinary sediment or heavy proteinuria.
In cases of potential ICI-related AKI, concomitant medications known to cause TIN (eg, NSAIDs, proton pump inhibitors, and some antibiotics) should be discontinued. If an antibiotic is implicated, and ongoing treatment of infection is required, an antibiotic from a different class should be used to treat the infection.
In patients with stage I AKI (Cr increase of >0.3 mg/dL or 1.5–1.9 times baseline), the ICI should be held while the patient undergoes evaluation and treatment of reversible causes (eg, hypovolemia). ICI therapy can be restarted if the AKI resolves. Nephrology referral should be considered for patients with progressive or persistent stage I AKI.
Patients with stage II or III AKI (Cr ≥2 times baseline) and/or significant (grade ≥2) proteinuria should have ICIs temporarily withheld and undergo expedited evaluation by a nephrologist.
Given the lack of specific clinical features for ICI-related AKI, renal biopsy should be strongly considered when feasible, particularly when a plausible alternative etiology for AKI exists or urine studies are suggestive of glomerular disease.
The first-line treatment for ICI-related TIN is glucocorticoids (LE: 3317). Patients with glomerular disease should receive standard therapy for the underlying lesion.
Patients with interstitial nephritis that does not respond to glucocorticoid therapy may receive infliximab or mycophenolate mofetil (LE: 4313–315).
Patients with renal allografts may receive ICIs, but only after extensive counseling on the associated risks and high probability of rejection and subsequent dialysis dependence (LE: 4318), particularly with anti-PD-(L)1 antibodies.
Cardiovascular toxicity
Myocarditis
Toxicities affecting the heart are uncommon with ICI therapy, but important due to the high mortality rate when they overtly develop. In a retrospective study of AEs in patients receiving ICIs, death occurred in 50% of patients who developed myocarditis and in 21% of patients who developed pericardial disease.319 Owing to the low number of events, data on incidence divided by drug and by specific cardiovascular toxicities (eg, myocarditis, pericardial disease) are limited. However, data gathered from an eight-center patient registry of 964 patients treated with ICIs found that the overall incidence of myocarditis was 1% (n=35). In the analysis, nearly all myocarditis cases had elevated troponins (94%) and an abnormal EKG (89%), while left ventricular ejection fraction (LVEF) was normal in 51% of cases. Among the 35 patients with myocarditis, 16 (46%) experienced a major adverse cardiac event, including ventricular arrythmias and complete heart block, cardiogenic shock, cardiac arrest, or cardiovascular death. In this analysis, myocarditis was associated with diabetes mellitus, sleep apnea, and high BMI, and occurred at a median onset of 34 days following the start of ICI therapy.47 The initial diagnosis for suspected cases of ICI-induced myocarditis typically looks for elevated troponin levels and EKG changes, followed by cardiac MRI, and finally the gold standard for myocarditis: endomyocardial biopsy (endovascular). Baseline and subsequently scheduled troponin levels can be obtained, but in asymptomatic patients there has been no evidence that this improves outcome or even provides an early indicator of possible myocarditis. Patients with myocarditis are generally initially treated with high-dose corticosteroids. Early treatment with steroids may be important, as shown in a retrospective analysis including 126 patients with ICI-induced myocarditis from 23 different sites that found administration of corticosteroids within 24 hours of admission led to a lower rate of major adverse cardiac events (7.0%) than treatment between 24 and 72 hours (34.3%) and >72 hours after intake (85.1%; p<0.001).320 Those resistant to corticosteroids may benefit from therapies including ATG, mycophenolate mofetil, abatacept, or alemtuzumab.47 321–323 A retrospective analysis of 60 patients who developed ICI-associated myocarditis found that those requiring second-line immunosuppressives had higher all-cause mortality than those treated with steroids alone (50% vs 21%; p=0.02). Moreover, infliximab use was associated with increased risk of death from cardiovascular causes (odds ratio (OR) 12.0; 95% CI 2.1 to 67.1; p=0.005).324
Thromboembolic events
Attribution of thromboembolic events to ICI therapy may be difficult, since these events may occur as a result of cancer.325 326 Venous thromboembolism (VTE), in fact, is one of the most common causes of mortality in patients with cancer.327 It is estimated that between 4% and 20% of patients with cancer will develop VTE.328 Case reports have recorded thromboembolic events that appear to be temporally associated with ICI therapy.329–331 However, attempts to estimate the overall incidence of thromboembolic events in ICI-treated patients (roughly 8% in a retrospective study by Gutiérrez Sainz et al332) have not distinguished between events induced by ICI therapy and events induced by the malignancy itself (or thromboembolic events induced by other therapies, such as chemotherapy). Regardless of the ultimate etiology of the thrombotic event, oral apixaban has been shown to be non-inferior to subcutaneous dalteparin in a multinational randomized trial,333 and subsequent meta-analyses support direct-acting oral anticoagulants as standard of care for cancer-associated venous embolisms.334
Cardiovascular toxicity panel recommendations
The following recommendations are intended to be used within the framework of toxicity management, including direction for at what grade of toxicity to hold and/or permanently cease treatment, considerations for life-threatening toxicities, as well as recommendations on optimal timing and dosing for administration of corticosteroids and/or other immunosuppressive agents by grade of AE, discussed in the General panel recommendations section. For suspected myositis, myocarditis, and myasthenia gravis, there is a possibility of overlapping symptoms, and therefore patients should be evaluated with a shared set of diagnostics, as described in more detail in the General panel recommendations section. Any additional cardiac-specific exceptions or additional considerations are noted in the recommendations below. Additional consideration for the management of cardiac-related AEs may be found in the series of American Heart Association (AHA)/American College of Cardiology (ACC) guidelines.
Myocarditis
A diagnosis of ICI-induced myocarditis should be considered in any patient developing new cardiac symptoms, new cardiac arrhythmias, new heart blocks, or cardiac lab findings (eg, asymptomatic troponin elevation) who has received an ICI therapy in the past 12 weeks. Suspicion of ICI-induced myocarditis should trigger hospital admittance and consultation with a cardiologist.
Patients with suspected ICI-induced myocarditis should undergo cardiac MRI if available (with or without right heart catheterization and myocardial biopsy), EKG, and testing for serum troponin levels.
Patients with suspected ICI-induced myocarditis should receive high-dose corticosteroids (1000 mg methylprednisolone IV or equivalent daily for 3–5 days, until troponin normalizes) as soon as possible once the diagnosis is considered likely, followed by 4–6 weeks 1–2 mg/kg prednisone taper. Permanent discontinuation of ICI therapy should be seriously considered.
If signs or symptoms do not respond to corticosteroid therapy within 24 hours, additional therapies such as ATG, mycophenolate mofetil, abatacept, or alemtuzumab should be considered as additional treatment (LE: 4321–323). Caution is advised against the use infliximab for steroid-refractory myocarditis (LE: 4324).
Management of cardiac irAEs should take place in a coronary care unit, with temporary pacemaker support available for rapid access if indicated.
Thromboembolic events
If a patient experiences an arterial thromboembolic event, they should be examined for possible vasculitis. If vasculitis is not detected, the patient may be re-challenged with ICIs.
Patients who experience a thromboembolic event or are deemed at risk for such should not receive steroids and should instead receive typical treatments for thromboembolism, such as low molecular weight heparin or a direct-acting oral anticoagulant (LE: 1334–337).
Hematological toxicity
While hematological toxicities are uncommon, they are important to consider due to their potential to become life-threatening. Referral to a hematologist for management should be considered on a case-by-case basis. Hematological toxicities take a large number of forms, including cytopenias, acquired coagulopathies, and macrophage activation-related conditions, among others.331 338–343 The most common ICI-induced hematological irAEs are thrombocytopenia and hemolytic anemia (HA).103 344 While it is difficult to assess the overall incidence of hematological irAEs due to low numbers of cases, a study of 745 patients treated with anti-PD-(L)1 ICIs reported an incidence of <1% for all hematological irAEs. When a small group of patients who had previously experienced hematological irAEs was re-challenged with ICI therapy (n=7), 43% of patients experienced a recurrent hematological irAE. While the majority of hematological irAEs resolve to symptoms grade <2 following a median of 2–9 weeks, a number of patients exhibit symptoms for significantly longer.344
Hemolytic anemia
HA associated with ICI therapy (autoimmune HA (AIHA)) is one of the most common ICI-associated hematological irAEs. AIHA occurs in patients treated with ICIs at a median of 50 days after the initiation of treatment.103 The median time for AIHA to resolve below grade 2 symptoms is 2 weeks.344 Treatment with anti-PD-(L)1 ICIs appears to present a significantly greater risk of AIHA than treatment with anti-CTLA-4 ICIs.345
Thrombocytopenia
Thrombocytopenia is a fairly common occurrence in patients with cancer, but the recorded incidence of immune-related thrombocytopenia (immune thrombocytopenia (ITP)) is low.346 Thrombocytopenia can result from cancer itself, chemotherapy, other medications, disseminated intravascular coagulation (DIC), radiation therapy, some infections, and pre-existing autoimmunity (particularly in patients with hematological cancers).347–356 Because patients may already be experiencing thrombocytopenia as a result of cancer or due to a number of oncological treatment regimens, it may be prudent to establish a baseline platelet count and monitor for additional drops below this value when beginning ICI therapy.357 The median time to onset for ITP is 41 days, and the median time for symptoms to resolve to below grade 2 is 4 weeks.103 344 Steroid-refractory ITP has been successfully managed with rituximab.358 359
Hemaphagocytic lymphohistiocytosis/macrophage activation syndrome
Hemaphagocytic lymphohistiocytosis/macrophage activation syndrome (HLH/MAS) is a hematological disorder involving inappropriate macrophage activation, with a high potential for lethality. The diagnostic criteria include cytopenias, hyperferritinemia (commonly in thousands of ng/mL), fever, splenomegaly, coagulopathy, LFT abnormalities, and elevation of soluble IL-2 receptor. Examination of bone marrow aspirate by a pathologist can also be important to identify potential HLH.360 361 HLH occurs at a median of 26 days, and is more common in patients treated with anti-CTLA-4 ICIs than anti-PD-(L)1 ICIs.103 The management of HLH/MAS is complex and not ‘one size fits all,’ potentially encompassing cytotoxic chemotherapies such as etoposide, cytokine modulation with agents such as anti-IL-6, and/or corticosteroids, depending on the etiology and patient characteristics.361
Aplastic anemia
Aplastic anemia (AA) is often a result of immune-related bone marrow failure, and manifests as pancytopenia. AA has a low rate of resolution and is frequently difficult to treat.344 ATG has been attempted as a salvage therapy in a patient who developed lethal AA after dual PD-1/CTLA-4 inhibition for metastatic melanoma that did not improve after granulocyte colony-stimulating factor (G-CSF), tranexamic acid, and repeated platelet transfusions,362 but data are lacking on optimal management and options are limited.
Pure red cell aplasia
Pure red cell aplasia (PRCA) can be associated with either anti-CTLA-4 or anti-PD-(L)1 ICIs but occurs rarely. PRCA symptoms present at a median of 89 days following the start of ICI treatment.363
Neutropenia
ICI-related neutropenia typically occurs at a median of 10.5 weeks after the initiation of ICI therapy. As with any form of neutropenia, ICI-related neutropenia carries an increased risk of infectious complications.364
Hematological toxicity panel recommendations
The following recommendations are intended to be used within the framework of toxicity management, including direction for at what grade of toxicity to hold and/or permanently cease treatment, considerations for life-threatening toxicities, as well as recommendations on optimal timing and dosing for administration of corticosteroids and/or other immunosuppressive agents by grade of AE, discussed in the General panel recommendations section. Any hematological-specific exceptions or additional considerations are noted in the recommendations below.
Thrombocytopenia
Diagnostic workup for patients with possible ICI-related ITP should include CBC with differential, blood smear evaluation, DIC labs (PT/partial thromboplastin time (PTT)/fibrinogen/d-dimer), and LDH.
For patients with ICI-related ITP, treatment should follow hematological standard of care. Typically, this includes steroids (prednisone dose of 1 mg/kg oral or equivalent (LE: 1365)).
For patients with severe ITP, IVIG (0.5 g/kg/day for 5 days (LE: 1366) should be administered in addition to steroids. Rituximab may also be considered (LE: 2358 359).
Neutropenia
Diagnostic workup for patients with possible ICI-related neutropenia should include CBC with differential and blood smear evaluation.
For patients being treated with chemo-immunotherapy who develop neutropenia, it is important to differentiate between immune-related neutropenia and chemotherapy-induced myelosuppression.
For patients with immune-related neutropenia, treatment should follow hematological standard of care. Typically, this includes steroids (prednisone 1 mg/kg oral or equivalent) with G-CSF (LE: 3364 367).
Aplastic anemia and pure red cell aplasia
Diagnostic workup for patients with possible ICI-related AA, PRCA, or related pancytopenia/bone marrow failure should include CBC with differential, reticulocyte count, and blood smear evaluation.
For patients with ICI-related AA, additional immunosuppressive therapies beyond steroids should be used, such as cyclosporine. ATG may also be considered (LE: 4362).
For patients with PRCA, hematological standard of care includes steroids (LE: 3363).
For patients with steroid-refractory PRCA, additional immunosuppressive therapies such as cyclosporine may be required (LE: 3363). ATG may be also be considered (LE: 4362).
Hemaphagocytic lymphohistiocytosis
Diagnostic workup for patients with possible ICI-related HLH should include CBC with differential, blood smear evaluation, ferritin, and soluble IL-2 receptor. Because this condition is life-threatening, it should be suspected when symptoms arise and warrants early consultation with a specialist.
For patients with ICI-related secondary HLH, hematological consultation is required as this is a challenging condition to manage. Standard of care treatment typically involves steroids and immunosuppressives, such as etoposide or tocilizumab (LE: 3361 368).
Hemolytic anemia
Diagnostic workup for patients with possible ICI-related HA should include CBC with differential, reticulocyte count, blood smear evaluation, direct antiglobulin test (Coomb’s), and LDH with ADAMTS13 level.
For patients with ICI-related AIHA, treatment should follow hematological standard of care. Typically, this includes steroids (prednisone dose of 1 mg/kg oral or equivalent) (LE: 3369).
For patients with severe ICI-related AIHA that do not respond to steroids, IVIG (0.5 g/kg/day for 5 days) (LE: 3370) should be added.
Immune-relatedadverse events asscociated with ICI combination strategies
ICI combinations
Only one combination of ICIs is FDA-approved, nivolumab with ipilimumab, which has indications for the treatment of unresectable or metastatic melanoma, metastatic NSCLC, advanced RCC, hepatocellular carcinoma (HCC), microsatellite instability high (MSI-H) or mismatch repair deficient (dMMR) metastatic colorectal cancer, and mesothelioma.371 372 The dosing and timing for each ICI in the combination regimen is different across approved disease settings—for example, for HCC, ipilimumab is given at 3 mg/kg with nivolumab at 1 mg/kg every 3 weeks, whereas for metastatic NSCLC, ipilimumab is given at 1 mg/kg every 6 weeks with nivolumab 3 mg/kg every 3 weeks, and other schedules are approved as well. As discussed previously, combination ICI therapy generally results in a higher incidence of all-grade irAEs and of grade ≥3 irAEs. Combination therapy is also associated with higher rates of fatal toxicity—a meta-analysis encompassing >16,000,000 adverse drug reactions in records from 7 academic centers found that among the 613 fatal ICI-associated toxicities reported, the most common causes of death for combination anti-PD-(L)1/anti-CTLA-4 therapy were colitis (n=32; 37%) and myocarditis (n=22; 25%).373
Data are sparse for head-to-head comparisons of toxicities with ICI combination regimens at different dosing regimens in the same disease state. Of note, the phase IIIb/IV CheckMate 511 study, which enrolled patients with advanced melanoma, showed that combination regimens incorporating ipilimumab at 1 mg/kg are associated with fewer severe toxicities, despite comparable response rates. In the study, patients were randomized 1:1 to nivolumab at 1 mg/kg with 3 mg/kg ipilimumab or nivolumab at 3 mg/kg with ipilimumab at 1 mg/kg every 3 weeks for 4 doses. Objective response rates and PFS were not significantly different between the arms, however, the incidence of grade 3–5 TRAEs was significantly higher among the patients being treated with the higher dose of ipilimumab (48% vs 34%; p=0.006).374 Similarly, the CheckMate 040 trial, which randomized patients with HCC 1:1:1 to either nivolumab 1 mg/kg with ipilimumab 3 mg/kg every 3 weeks for 4 doses followed by nivolumab 240 mg every 2 weeks, nivolumab 3 mg/kg with ipilimumab 1 mg/kg every 3 weeks for 4 doses followed by nivolumab 240 mg every 2 weeks, or nivolumab 3 mg/kg every 2 weeks with ipilimumab 1 mg/kg every 6 weeks, found higher incidence of irAEs overall as well as more irAEs requiring discontinuation of treatment in the group receiving high-dose ipilimumab.375
ICI-chemotherapy combinations
An expanding number of specific combination regimens involving chemotherapy and ICIs have been approved by the FDA, including indications for breast cancer, head and neck squamous cell carcinoma, and lung cancer. Clinical trials involving ICI-chemotherapy combinations have reported toxicity profiles that generally correspond to the additive effects of each agent as monotherapy; combination regimens have not thus far resulted in new AE signals.376–380
ICI-targeted therapy combinations
ICIs in combination with a variety of small molecule tyrosine kinase inhibitors (TKIs) or anti-angiogenic antibodies have been approved in a variety of disease settings, such as HCC, RCC, NSCLC, and melanoma. The approved combination regimens involving TKIs with ICIs have generally thus far resulted in toxicity profiles similar to those of each agent administered as a monotherapy (eg, rash and diarrhea with TKIs, and hypertension with anti-vascular endothelial growth factor receptor (VEGFR) antibodies), although the combination of pembrolizumab with axitinib appeared to cause a higher incidence of grade ≥3 AEs.381 382 A multitude of ongoing studies are investigating ICIs with other small molecule inhibitors against a variety of targets. Other combinations, such as ipilimumab with vemurafenib,383 durvalumab with osimertinib,384 nivolumab with ademaciclib,385 and ipilimumab with dabrafenib and trametinib,386 have exhibited unexpectedly high rates of toxicity, leading to clinical trial discontinuations. Severe liver toxicity in addition to increased incidence of pneumonitis has been seen with the combination of epidermal growth factor receptor (EGFR) TKIs and anti-PD-(L)1 ICIs,384 387 emphasizing the need for caution in the application of combination immunotherapy regimens. The management of toxicities arising from combination regimens may be complex, and thus consultation with appropriate specialists (eg, cardiology in cases of cardiac AEs with ICI/VEGFR TKI combinations) should be top-of-mind.
ICI combinations panel recommendations
The following recommendations are intended to be used within the framework of toxicity management, including direction for at what grade of toxicity to hold and/or permanently cease treatment, considerations for life-threatening toxicities, as well as recommendations on optimal timing and dosing for administration of corticosteroids and/or other immunosuppressive agents by grade of AE, discussed in the General panel recommendations section. Any exceptions specific to combination ICI therapies or additional considerations are noted in the recommendations below.
Patients receiving combination ICI therapies should be counseled on the increased risk of toxicities, including long-term or delayed toxicities (LE: 14), especially when ipilimumab is given at 3 mg/kg as opposed to 1 mg/kg (LE: 2374). These patients may also be monitored more frequently for signs and symptoms of irAEs.
Patients should be counseled to monitor their blood pressure routinely while being treated with pembrolizumab and axitinib (LE: 2381).
Patients experiencing hypertension while being treated with combination immunotherapy and axitinib should be prescribed medication to control their hypertension, and axitinib may be held if hypertension is grade ≥2.
In patients being treated with combination therapies, it is important to attribute the source of an AE to the appropriate drug or condition. If an AE can be attributed to a non-ICI etiology, the dose of the ICI should be maintained and appropriate supportive care should be initiated.
If the origin of an AE cannot be attributed with confidence, referral to an appropriate specialist can be considered if further diagnostic testing may impact treatment decisions.
Conclusions
Rapid progress in the development and implementation of ICIs has been accompanied by an increased need for effective diagnosis and management of ICI-induced toxicity. Continued clinical trials will hopefully provide additional data on the incidence of, and risk factors contributing to, these diverse AEs. An important area of research is translational studies aimed at developing validated predictive biomarkers for early identification of at-risk patients. Ideally, future research will continue to improve the management of ICI-induced toxicity and result in improvements to standardized protocols for their diagnosis, monitoring, and resolution. As the field evolves, these guidelines may be updated.
Ethics statements
Acknowledgments
The authors acknowledge SITC staff for their contributions including Ben Labbe, PhD and Sam Million-Weaver, PhD for medical writing, and Emily Gronseth, PhD; Angela Kilbert; and Lionel Lim for project management and editorial support. Additionally, the authors wish to thank the society for supporting the manuscript development. In addition, SITC wishes to thank the American Society for Transplantation and Cellular Therapy (ASTCT) for providing a representative to serve on the SITC Immune Checkpoint Inhibitor-related Adverse Events Guideline Expert Panel.
References
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
Footnotes
Twitter @PAscierto
Contributors All authors served on the SITC Immune Checkpoint Inhibitor-related Adverse Events Guideline Expert Panel, drafted content, and provided critical review during the manuscript development. MSE and JRB provided leadership as Chairs of the Expert Panel and provided guidance on the manuscript structure and content and thus are first and last authors; all other authors contributed equally to the manuscript development and review and therefore are listed alphabetically by last name. JB was the patient advocate representative. All authors have read and approved the final version of this manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests PAA—Contracted research: Bristol-Myers Squibb, Roche, Array; Consulting fees: Bristol-Myers Squibb, Roche, Array, Novartis, Merck Serono, Pierre Fabre, Incyte, Medimmune, Sindax, AstraZeneca, Sun Pharma, Sanofy, Idera, Ultimovacs, Sandox, Immunocore, 4sc, Alkermes, Italfarmaco, Nektar, Boehringer-Ingelheim, Eisai, Regeneron; Travel support: MSD. JRB—Contracted research: AstraZeneca, Bristol-Myers Squibb, Genentech/Roche, Merck, RAPT Therapeutics, Inc, Revolution Medicines; Consulting fees: Amgen, Bristol-Myers Squibb, Genentech/Roche, Eli Lilly, GlaxoSmithKline, Merck, Sanofi, Regeneron; Data and safety monitoring board/committees: GlaxoSmithKline, Sanofi. JB—Partner consulting fees: AstraZeneca, Merck, Roche, Pfizer, Lilly, Daiichi, Seattle Genetics, Novartis. LCC—Consulting fees: AbbVie; Contracted research: Bristol-Myers Squibb, Merck, EMD Serono, Alkermes, Iovance, Merrimack, National Cancer Institute. DEG—Consulting fees: Samsung Bioepis, Catalyst Pharmaceuticals, Bristol-Myers Squibb Steering Committee, G1 Therapeutics; Contracted research: AstraZeneca, BerGenBio, Karyopharm, Bristol-Myers Squibb Steering Committee; Ownership interest: Gilead. DBJ—Consulting fees: Bristol-Myers Squibb, Catalyst Biopharma, Iovance, Jansen, Merck, Novartis, Oncosec; Contracted research: Bristol-Myers Squibb, Incyte. MEL—Contracted research: Veloce, US Biotest, Lutris, Paxman, Novocure Inc; Grant funding: National Cancer Institute Cancer Center support grant P30 CA008748, National Institute of Arthritis and Musculoskeletal and Skin Diseases grant U01AR0775; Royalty: Legacy Healthcare Services, Apricity Health, Azitra, Inc, Deciphera, Galderma Research and Development, Johnson and Johnson, NCODA, Novocure Inc, Kyowa Kirin Inc, Loxo, Merck Sharp and Dohme Corporation, Janssen Research & Development, Menlo Therapeutics, Novartis Pharmaceuticals Corporation, QED Therapeutics, F. Hoffmann-La Roche AG, Amgen Inc, AstraZeneca Pharmceuticals, Genentech Inc, Seattle Genetics, Lutris, Paxman Coolers, OnQuality Pharmaceuticals Ltd, Takeda Millenium. JN—Consulting fees: AstraZeneca, Bristol-Myers Squibb, Merck, Roche/Genentech; Contracted research: AstraZeneca, Merck; Non-CME services: Merck, Bristol-Myers Squibb, AstraZeneca. M-AP—Consulting fees: AbbVie, Bellicum, Celgene, Bristol-Myers Squibb, Incyte, Kite/Gilead, Merck, Novartis, Nektar Therapeutics, Omeros, and Takeda; Contracted research: Incyte, Kite/Gilead and Miltenyi Biotec; Ownership interest: NexImmune Member, DSMBs for Cidara Therapeutics, Servier and Medigene. IP—Consulting fees: Merck, Amgen; Ownership interest: Celldex; Partner ownership: Celldex. BDS—Consulting fees: Kite/Gilead, Juno/Celgene; Contracted research: ADC Therapeutics; NPI: 1215164884. SPS—Consulting fees: Takeda, GSK, Kura, Celgene, Daiichi-Sankyo. DS—Scientific advisory board: Allergan, Alimera, Biogen. JAS—Consulting fees: Array, Nektar, Bristol-Myers Squibb, Iovance, Curis; Contracted research: Bristol-Myers Squibb, Corvus, Caltera. HA-S, FBC, MSE, LH, EH, GAM, MN, RS, MT—Nothing to disclose. SITC staff: SMW—Shares owned: Pacific Biosciences of California Inc, Editas Medicine. EG, AK, BL, LL—Nothing to disclose.
Provenance and peer review Not commissioned; externally peer reviewed.