
The Underutilization, Adverse Reactions and Efficacy of Statins after Liver Transplant: A Meta-Analysis and Systematic Review

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
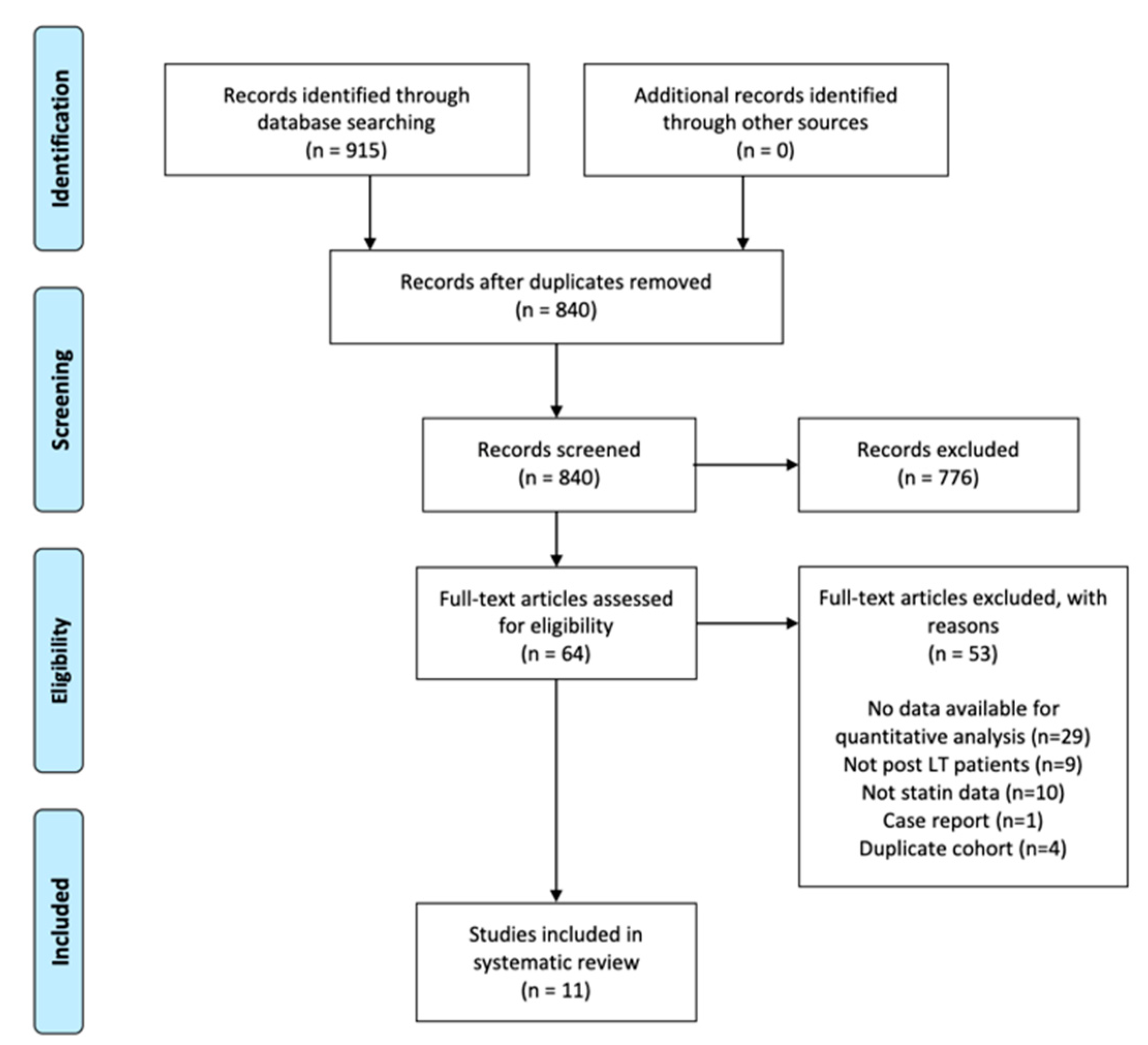
2.1. Search Strategy
2.2. Study Selection and Extraction
2.3. Statistical Analysis and Quality Assessment
3. Results
3.1. Summary of Included Articles
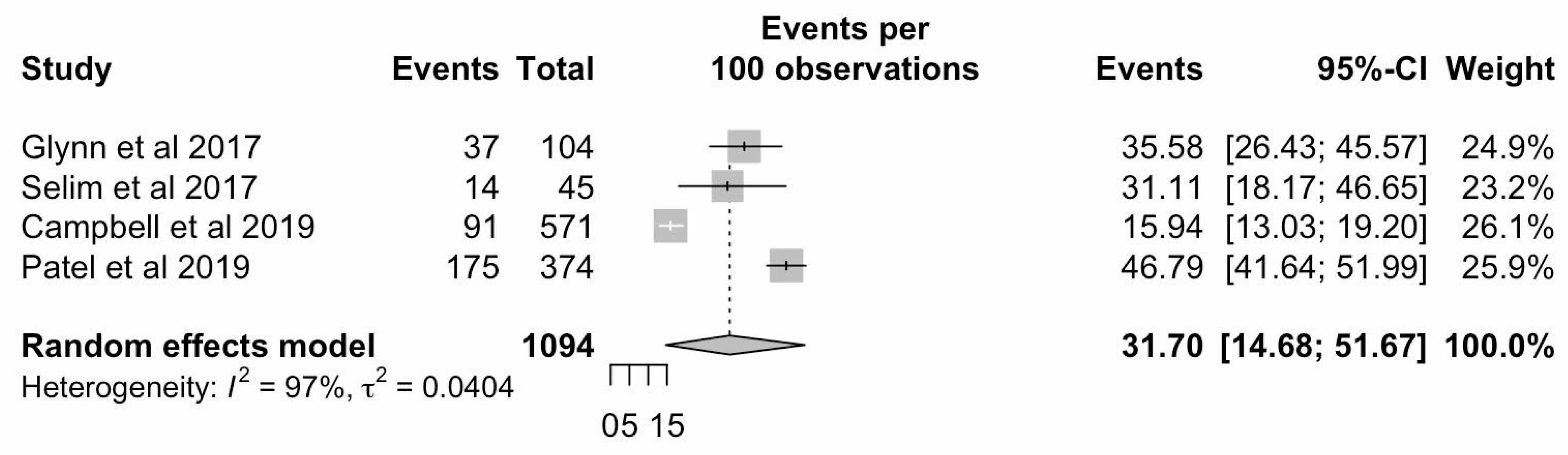
3.2. Indications and Utilization
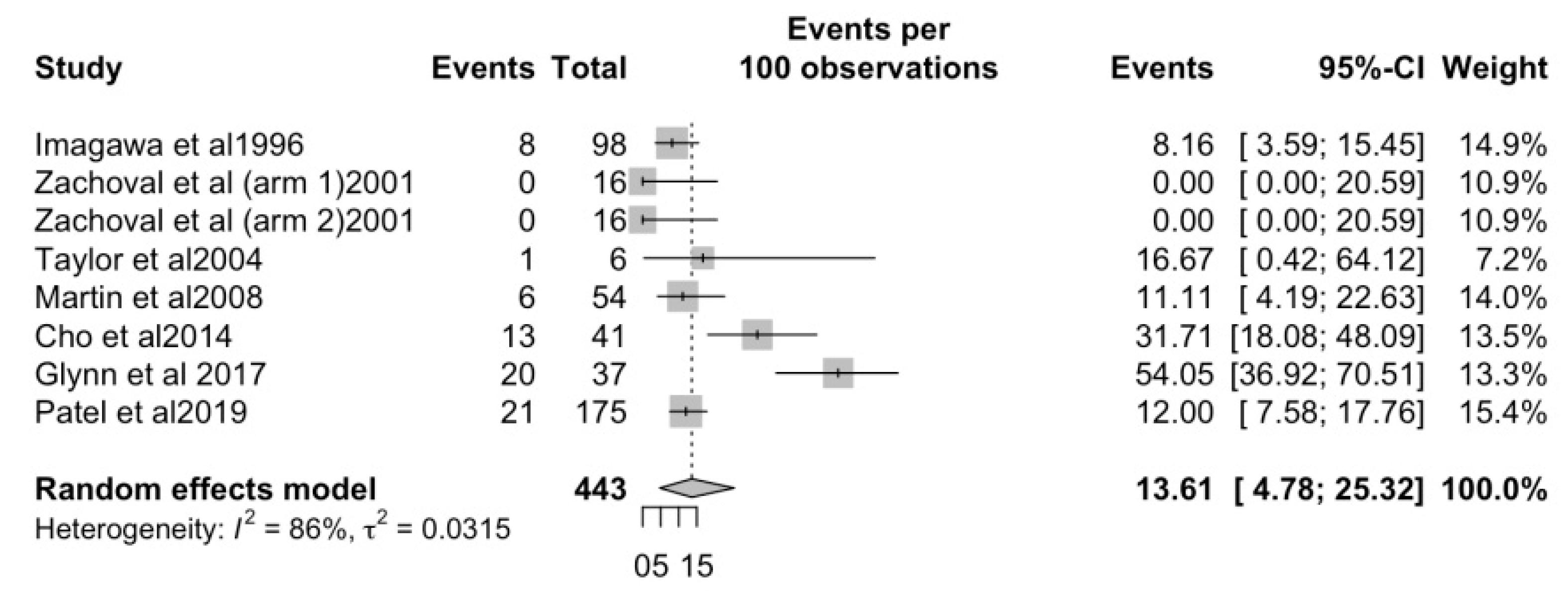
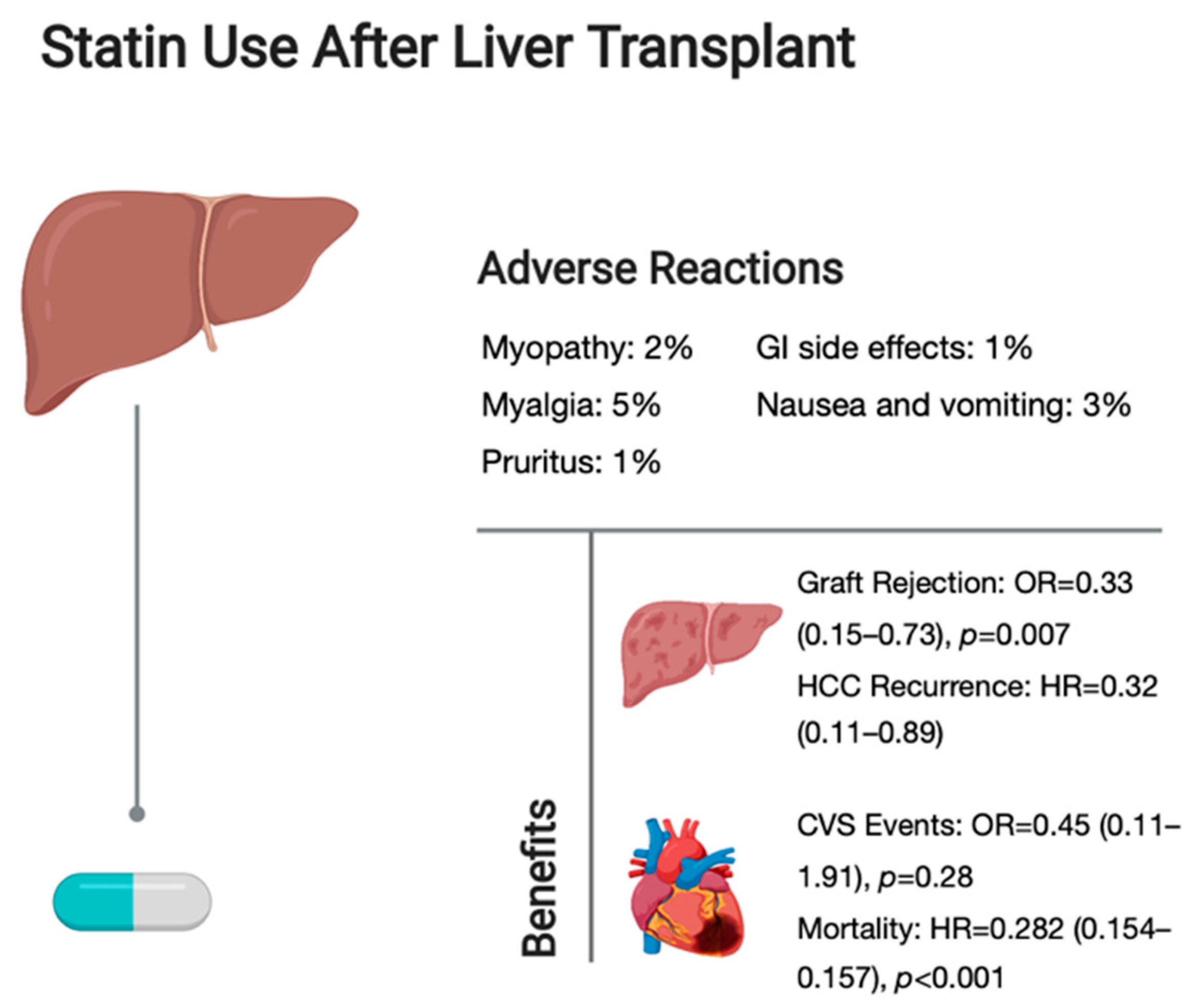
3.3. Adverse Events
3.4. Lipids, Cardiovascular Events and Overall Mortality
3.5. Graft Rejection and HCC Recurrence
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Laish, I.; Braun, M.; Mor, E.; Sulkes, J.; Harif, Y.; Ben Ari, Z. Metabolic syndrome in liver transplant recipients: Prevalence, risk factors, and association with cardiovascular events. Liver Transpl. 2011, 17, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Mells, G.; Neuberger, J. Reducing the risks of cardiovascular disease in liver allograft recipients. Transplantation 2007, 83, 1141–1150. [Google Scholar] [CrossRef] [PubMed]
- Hüsing, A.; Kabar, I.; Schmidt, H.H. Lipids in liver transplant recipients. World J. Gastroenterol. 2016, 22, 3315–3324. [Google Scholar] [CrossRef]
- Madhwal, S.; Atreja, A.; Albeldawdi, M.; Lopez, R.; Post, A.; Costa, M.A. Is liver transplantation a risk factor for cardiovascular disease? a meta-analysis of observational studies. Liver Transpl. 2012, 18, 1140–1146. [Google Scholar] [CrossRef] [PubMed]
- Kim, N.G.; Sharma, A.; Saab, S. Cardiovascular and metabolic disease in the liver transplant recipient. Best Pract. Res. Clin. Gastroenterol. 2020, 46–47, 101683. [Google Scholar] [CrossRef]
- Fatourou, E.M.; Tsochatzis, E.A. Management of metabolic syndrome and cardiovascular risk after liver transplantation. Lancet Gastroenterol. Hepatol. 2019, 4, 731–741. [Google Scholar] [CrossRef]
- Bagley, J.; Williams, L.; Hyde, M.; Birriel, C.R.; Iacomini, J. Hyperlipidemia and Allograft Rejection. Curr. Transplant Rep. 2019, 6, 90–98. [Google Scholar] [CrossRef]
- Bibbins-Domingo, K.; Grossman, D.C.; Curry, S.J.; Davidson, K.W.; Epling, J.W.; García, F.A.; Gillman, M.W.; Kemper, A.R.; Krist, A.H.; Kurth, A.E.; et al. Statin use for the primary prevention of cardiovascular disease in adults: US preventive services task force recommendation statement. JAMA J. Am. Med. Assoc. 2016, 316, 1997–2007. [Google Scholar]
- Martin, J.E.; Cavanaugh, T.M.; Trumbull, L.; Bass, M.; Weber, F.; Jr Aranda-Michel, J. Incidence of adverse events with HMG-CoA reductase inhibitors in liver transplant patients. Clin. Transpl. 2008, 22, 113–119. [Google Scholar] [CrossRef]
- Cho, Y.; Lee, M.J.; Choe, E.Y.; Jung, C.H.; Joo, D.J.; Kim, M.S. Statin therapy is associated with the development of new-onset diabetes after transplantation in liver recipients with high fasting plasma glucose levels. Liver Transpl. 2014, 20, 557–563. [Google Scholar] [CrossRef] [Green Version]
- Selim, R.; Abdulhamid, A.; Shyamraj, A.; Watson, A.; Tang, J.; Jafri, S.M. Statins in liver transplant recipients: Rates of use, mortality and rejection. Am. J. Transpl. 2017, 17, 585. [Google Scholar]
- Tan, P.S.; Muthiah, M.; Koh, T.; Teoh, Y.; Chan, A.; Kow, A. Asian Liver Transplant Network Clinical Guidelines on Immunosuppression in Liver Transplantation. Transplantation 2018, 103, 1. [Google Scholar] [CrossRef]
- Patel, S.S.; Guzman, L.A.; Lin, F.-P.; Pence, T.; Reichman, T.; John, B. Utilization of aspirin and statin in management of coronary artery disease in patients with cirrhosis undergoing liver transplant evaluation. Liver Transpl. 2018, 24, 872–880. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campbell, P.T.; VanWagner, L.B. Mind the Gap: Statin Underutilization and Impact on Mortality in Liver Transplant Recipients. Liver Transpl. Soc. 2019, 25, 1477–1479. [Google Scholar] [CrossRef] [PubMed]
- Rostami, Z.; Arani, M.; Salesi, M.; Safiabadi, M.; Einollahi, B. Effect of Statins on Patients and Graft Survival in Kidney Transplant Recipients: A Survival Meta-analysis. Iran. J. Kidney Dis. 2017, 11, 329–338. [Google Scholar]
- Huang, X.; Jia, Y.; Zhu, X.; Zhang, Y.; Jiang, L.; Wei, X. Effects of Statins on Lipid Profile of Kidney Transplant Recipients: A Meta-Analysis of Randomized Controlled Trials. BioMed. Res. Int. 2020, 9094543. [Google Scholar]
- Mehra, M.R.; Raval, N.Y. Metaanalysis of statins and survival in de novo cardiac transplantation. Transplant Proc. 2004, 36, 1539–1541. [Google Scholar] [CrossRef]
- Vallakati, A.; Reddy, S.; Dunlap, M.E.; Taylor, D.O. Impact of Statin Use After Heart Transplantation: A Meta-Analysis. Circ. Heart Fail. 2016, 9, 10. [Google Scholar] [CrossRef] [PubMed]
- Blais, P.; Lin, M.; Kramer, J.R.; El-Serag, H.B.; Kanwal, F. Statins Are Underutilized in Patients with Nonalcoholic Fatty Liver Disease and Dyslipidemia. Dig. Dis. Sci. 2016, 61, 1714–1720. [Google Scholar] [CrossRef] [PubMed]
- Almutairi, F.; Peterson, T.C.; Molinari, M.; Walsh, M.J.; Alwayn, I.; Peltekian, K.M. Safety and effectiveness of ezetimibe in liver transplant recipients with hypercholesterolemia. Liver Transpl. 2009, 15, 504–508. [Google Scholar] [CrossRef]
- Loffredo, L.; Pastori, D.; Farcomeni, A.; Violi, F. Effects of Anticoagulants in Patients with Cirrhosis and Portal Vein Thrombosis: A Systematic Review and Meta-analysis. Gastroenterology 2017, 153, 480–487.e1. [Google Scholar] [CrossRef] [Green Version]
- Sedgwick, P. What is publication bias in a meta-analysis? BMJ Br. Med. J. 2015, 351, h4419. [Google Scholar] [CrossRef] [PubMed]
- Hopewell, S.; McDonald, S.; Clarke, M.J.; Egger, M. Grey literature in meta-analyses of randomized trials of health care interventions. Cochrane Database Syst. Rev. 2007. [Google Scholar] [CrossRef]
- McKenzie, J.E.; Brennan, S.E.; Ryan, R.E.; Thomson, H.J.; Johnston, R.V.; Thomas, J. Defining the criteria for including studies and how they will be grouped for the synthesis. Cochrane Handb. Syst. Rev. Int. 2019, 3, 33–65. [Google Scholar]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Furukawa, T.A.; Barbui, C.; Cipriani, A.; Brambilla, P.; Watanabe, N. Imputing missing standard deviations in meta-analyses can provide accurate results. J. Clin. Epidemiol. 2006, 59, 7–10. [Google Scholar] [CrossRef] [PubMed]
- Nyaga, V.N.; Arbyn, M.; Aerts, M. Metaprop: A Stata command to perform meta-analysis of binomial data. Arch. Public Health 2014, 72, 39. [Google Scholar] [CrossRef] [Green Version]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control Clin. Trials. 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Harris, R.; Bradburn, M.; Deeks, J.; Harbord, R.; Altman, D.; Sterne, J. Metan: Fixed and random-effects meta-analysis. Stata J. 2008, 8, 3–28. [Google Scholar] [CrossRef] [Green Version]
- Fletcher, J. What is heterogeneity and is it important? BMJ 2007, 334, 94–96. [Google Scholar] [CrossRef]
- Aromataris, E.; Fernandez, R.; Godfrey, C.M.; Holly, C.; Khalil, H.; Tungpunkom, P. Summarizing systematic reviews: Methodological development, conduct and reporting of an umbrella review approach. Int. J. Evid. Based Healthc. 2015, 13, 132–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borges Migliavaca, C.; Stein, C.; Colpani, V.; Barker, T.H.; Munn, Z.; Falavigna, M. How are systematic reviews of prevalence conducted? A methodological study. BMC Med. Res. Methodol. 2020, 20, 96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imagawa, D.K.; Dawson Iii, S.; Holt, C.D.; Kirk, P.S.; Kaldas, F.M.; Shackleton, C.R. Hyperlipidemia after liver transplantation: Natural history and treatment with the hydroxy-methylglutaryl-coenzyme A reductase inhibitor pravastatin. Transplantation 1996, 62, 934–942. [Google Scholar] [CrossRef] [PubMed]
- Zachoval, R.; Gerbes, A.L.; Schwandt, P.; Parhofer, K.G. Short-term effects of statin therapy in patients with hyperlipoproteinemia after liver transplantation: Results of a randomized cross-over trial. J. Hepatol. 2001, 35, 86–91. [Google Scholar] [CrossRef]
- Taylor, P.J.; Kubler, P.A.; Lynch, S.V.; Allen, J.; Butler, M.; Pillans, P.I. Effect of Atorvastatin on Cyclosporine Pharmacokinetics in Liver Transplant Recipients. Ann. Pharmacother. 2004, 38, 205–208. [Google Scholar] [CrossRef] [PubMed]
- Mela, M.; Gelson, W.; Unitt, E.; Alexander, G. Statins before and after liver transplantation—A randomised control trial with 5-year follow-up. J. Hepatol. 2011, 54, S227–S228. [Google Scholar] [CrossRef]
- Glynn, M.; Jantz, A.; Summers, B.; Salgia, R.; Sulejmani, N. Safety of statin therapy after liver transplantation. Am. J. Transpl. 2017, 17, 585. [Google Scholar]
- Campbell, P.T.; Kosirog, M.; Montag, S.; Connolly, S.; Daud, A.; Das, A. Guideline adherence for secondary prevention of stroke and atherosclerotic cardiovascular disease among liver transplant recipients. Am. J. Transpl. 2019, 19, 864. [Google Scholar]
- Cho, Y.; Kim, M.S.; Nam, C.M.; Kang, E.S. Statin Use is Associated with Decreased Hepatocellular Carcinoma Recurrence in Liver Transplant Patients. Sci. Rep. 2019, 9, 1467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, S.S.; Rodriguez, V.A.; Siddiqui, M.B.; Faridnia, M.; Lin, F.-P.; Chandrakumaran, A. The Impact of Coronary Artery Disease and Statins on Survival after Liver Transplantation. Liver Transpl. Soc. 2019, 25, 1514–1523. [Google Scholar] [CrossRef]
- Hwang, S.D.; Lee, J.H.; Jhee, J.H.; Kim, Y.J.; Park, K.M.; Kim, J.K. Effect of Fluvastatin on Cardiovascular Complications in Kidney Transplant Patients: A Systemic Review and Meta-analysis. Transpl. Proc. 2019, 51, 2710–2713. [Google Scholar] [CrossRef]
- Palmer, S.C.; Navaneethan, S.D.; Craig, J.C.; Perkovic, V.; Johnson, D.W.; Nigwekar, S.U. HMG CoA reductase inhibitors (statins) for kidney transplant recipients. Cochrane Database Syst. Rev. 2014, 1, 5019. [Google Scholar] [CrossRef]
- Som, R.; Morris, P.J.; Knight, S.R. Graft vessel disease following heart transplantation: A systematic review of the role of statin therapy. World J. Surg. 2014, 38, 2324–2334. [Google Scholar] [CrossRef]
- Chou, R.; Dana, T.; Blazina, I.; Daeges, M.; Jeanne, T.L. Statins for Prevention of Cardiovascular Disease in Adults: Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA 2016, 316, 2008–2024. [Google Scholar] [CrossRef] [PubMed]
- Saliba, F.; Lakehal, M.; Pageaux, G.P.; Roche, B.; Vanlemmens, C.; Duvoux, C. Risk factors for new-onset diabetes mellitus following liver transplantation and impact of hepatitis C infection: An observational multicenter study. Liver Transpl. 2007, 13, 136–144. [Google Scholar] [CrossRef] [PubMed]
- Sattar, N.; Preiss, D.; Murray, H.M.; Welsh, P.; Buckley, B.M.; de Craen, A.J. Statins and risk of incident diabetes: A collaborative meta-analysis of randomised statin trials. Lancet 2010, 375, 735–742. [Google Scholar] [CrossRef]
- Chin, Y.H.; Tan, H.Q.M.; Ng, C.H.; Tan, D.J.H.; Lin, S.Y.; Huang, D.Q.; Khoo, C.M.; Muthiah, M.D. A Time-Based Meta-Analysis on the Incidence of New Onset Diabetes after Liver Transplantation. J. Clin. Med. 2021, 10, 1045. [Google Scholar] [CrossRef]
- Migliozzi, D.R.; Asal, N.J. Clinical Controversy in Transplantation: Tacrolimus Versus Cyclosporine in Statin Drug Interactions. Ann. Pharmacother. 2020, 54, 171–177. [Google Scholar] [CrossRef]
- Lemahieu, W.P.; Hermann, M.; Asberg, A. Combined therapy with atorvastatin and calcineurin inhibitors: No interactions with tacrolimus. Am. J. Transplant. 2005, 5, 2236–2243. [Google Scholar] [CrossRef]
- Tan, D.J.H.; Wong, C.; Ng, C.H. A Meta-Analysis on the Rate of Hepatocellular Carcinoma Recurrence after Liver Transplant and Associations to Etiology, Alpha-Fetoprotein, Income and Ethnicity. J. Clin. Med. 2021, 10, 238. [Google Scholar] [CrossRef]
- Pradelli, D.; Soranna, D.; Scotti, L.; Zambon, A.; Catapano, A.; Mancia, G. Statins and primary liver cancer: A meta-analysis of observational studies. Eur. J. Cancer Prev. 2013, 22, 229–234. [Google Scholar] [CrossRef] [PubMed]
- Dogan, N.; Hüsing-Kabar, A.; Schmidt, H.H.; Cicinnati, V.R.; Beckebaum, S.; Kabar, I. Acute allograft rejection in liver transplant recipients: Incidence, risk factors, treatment success, and impact on graft failure. J. Int. Med. Res. 2018, 46, 3979–3990. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year | Country | Study Design | Sample Size/N (Statin) | Mean Age/Years | Medication | Indication | Quality |
|---|---|---|---|---|---|---|---|
| Imagawa et al., 1996 | USA | Prospective Cohort | 98 | NA | Pravastatin | 2 or more coronary artery disease risk factors | 7 |
| Zachoval et al., 2001 | Germany | Randomized Controlled Trial | 16 | 54.75 | Cerivastatin | LDL > 100 mg/dL (coronary artery disease patients), LDL > 130 mg/dL (>2 risk factors), LDL > 160 mg/dL (≤1 risk factor) | 8 |
| Pravastatin | |||||||
| Taylor et al., 2004 | Australia | Prospective Cohort | 6 | 54.3 ± 8.34 | Atorvastatin | Persistent elevation of TC > 213 mg/dL or LDL > 128 mg/dL | |
| Martin et al., 2008 | USA | Retrospective Cohort | 54 | NA | Atorvastatin, Fluvastatin, Lovastatin, Pravastatin, Simvastatin | LDL > 130 mg/dL or LDL > 100 mg/dL for high-risk patients or LDL > 70 mg/dL for very high-risk patients | 7 |
| Mela et al., 2011 * | UK | Randomized Control Trial | 53 | NA | Unspecified Statins | Risk of hypercholesteremia, cardiovascular disease and cerebrovascular disease (at the discretion of the responsible clinician) | 4 |
| Cho et al., 2014 | South Korea | Retrospective Cohort | 41 | 51.4 ± 8.1 | Atorvastatin, Fluvastatin, Pravastatin, Pitivastatin Rosuvastatin | Hypercholesterolemia (mean TC = 251 ± 52.5 mg/dL) | 11 |
| Glynn et al., 2017 * | USA | Retrospective Cohort | 37 | NA | Unspecified Statins | Hyperlipidemia | 3 |
| Selim et al., 2017 * | USA | Retrospective Cohort Study | 14 | NA | Unspecified Statin | Diabetes mellitus and coronary artery disease | 2 |
| Campbell et al., 2019 * | USA | Retrospective Cohort | 91 | NA | Unspecified Statin | Secondary prevention of atherosclerotic cardiovascular disease and stroke | 4 |
| Cho et al., 2019 | South Korea | Retrospective Cohort | 112 | 56.7 ± 6.0 | Unspecified Statin | NA | 11 |
| Patel et al., 2019 | USA | Retrospective Cohort | 175 | 55.3 ± 9.3 | Unspecified Statin | LDL > 100 mg/dL in diabetics, LDL > 130 mg/dL in nondiabetics or TC > 200 mg/dL or known history of cardiovascular disease | 8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ho, Y.J.; Koh, A.S.-M.; Ong, Z.H.; Ng, C.H.; Kong, G.; Chew, N.W.S.; Lim, H.N.; Siddiqui, M.S.; Muthiah, M.D. The Underutilization, Adverse Reactions and Efficacy of Statins after Liver Transplant: A Meta-Analysis and Systematic Review. Transplantology 2021, 2, 264-273. https://doi.org/10.3390/transplantology2030025
Ho YJ, Koh AS-M, Ong ZH, Ng CH, Kong G, Chew NWS, Lim HN, Siddiqui MS, Muthiah MD. The Underutilization, Adverse Reactions and Efficacy of Statins after Liver Transplant: A Meta-Analysis and Systematic Review. Transplantology. 2021; 2(3):264-273. https://doi.org/10.3390/transplantology2030025
Chicago/Turabian StyleHo, Yeung Jek, Audrey Su-Min Koh, Zhi Hao Ong, Cheng Han Ng, Gwyneth Kong, Nicholas W.S. Chew, Hui Ning Lim, M. Shadab Siddiqui, and Mark Dhinesh Muthiah. 2021. "The Underutilization, Adverse Reactions and Efficacy of Statins after Liver Transplant: A Meta-Analysis and Systematic Review" Transplantology 2, no. 3: 264-273. https://doi.org/10.3390/transplantology2030025