Article Text

Abstract
Objective: To characterise the circulating cytokine profile and the cellular source of circulating cytokines in polymyalgia rheumatica (PMR).
Methods: The study included 34 patients with active untreated PMR and 17 age-matched healthy controls (HC). Circulating cytokines were measured by cytometric bead array and ELISA. Intracellular cytokines were assessed in CD3+ and CD14+ cells by flow cytometry. Cytokines in cell culture supernatants were also determined after polyclonal stimulation of patients’ peripheral blood mononuclear cells.
Results: Circulating levels of interleukin-6 (IL6) were significantly higher in subjects with active PMR than in HC. Corticosteroid (CS) treatment was followed by a decrease in the level of IL6. Intracellular cytokine staining showed that circulating monocytes did not produce higher amounts of proinflammatory cytokines in patients with PMR than in HC. There was a discordance between serum levels and cytokine-producing monocyte and T cells, and it was not possible to demonstrate a Th1 bias in the peripheral compartment.
Conclusions: Active PMR is characterised by increased serum levels of IL6, but not of other proinflammatory cytokines, that are rapidly suppressed by CS treatment. As circulating monocytes do not show increased production of proinflammatory cytokines, IL6 may be mainly produced in the inflamed tissue. A study of the circulating cytokine profile and its cellular source may provide a clue to new therapeutic options.
Statistics from Altmetric.com
Polymyalgia rheumatica (PMR) is a chronic inflammatory disorder of unknown aetiology in elderly subjects.1 It presents with inflammation of joint and periarticular structures and is characterised by systemic manifestations such as fever, anorexia and weight loss.1 These manifestations are accompanied by laboratory abnormalities characteristic of a florid acute phase response such as anaemia, thrombocytosis and increased erythrocyte sedimentation rate (ESR) and C reactive protein (CRP) level.2 3 The mechanisms linking tissue inflammation and the systemic component of the disease remain undefined, but may involve proinflammatory cytokines that act as endocrine mediators at the site of inflammation.4 An alternative but not exclusive hypothesis suggests that this syndrome has a systemic component that is at least partially independent of the tissue component and mediated by the production of proinflammatory mediators, especially interleukin-6 (IL6), by circulating monocytes.4
Cytokines are involved in the pathogenesis of most inflammatory diseases and a number of studies have addressed their role in the pathogenesis of PMR.4 5 However, the cellular type and the site of production of circulating cytokines, the interaction between T cell-derived and macrophage-derived cytokines, and the influence of corticosteroid (CS) treatment in a wide range of circulating cytokines have rarely been assessed. The importance of clarifying the role of cytokines in PMR also has implications for its treatment, as we now have available an increasing number of effective biological agents directed against cytokines.
The purpose of the present study was to identify the cellular source of circulating cytokines and the state of activation of the different peripheral blood mononuclear cells (PBMC) in patients with PMR. We also analysed the influence of CS treatment on circulating cytokines.
Methods
Study subjects
The study included 34 prospectively recruited patients with active and untreated PMR and 17 healthy controls (HC). One sample from 14 of the 34 patients was also studied after disease remission with CS treatment. Patients with PMR were diagnosed according to the criteria proposed by Chuang et al.3 Patients with PMR and ESR <40 mm/1 h but who satisfied other clinical criteria were also included in the study.2 In patients with PMR, giant cell arteritis (GCA) was excluded by a negative temporal artery biopsy and/or a complete resolution of symptoms with low-dose CS (10 mg/day prednisone) and the absence of characteristic GCA manifestations. Patients with polymyalgic symptoms who satisfied the ACR 1987 revised criteria for rheumatoid arthritis6 were excluded. Seventeen age-matched healthy controls (HC) without a previous history of infectious, neoplastic or autoimmune disease were included in the study.
The clinical findings at diagnosis and during follow-up, the ESR and CRP values at diagnosis and the initial prednisone dosage were ascertained by reviewing the patients’ medical records (table 1). At the time of diagnosis, all patients with isolated PMR received an initial dose of prednisone of 10 mg/day immediately after obtaining the blood sample for the pretreatment study. Reductions in CS therapy were individualised according to physician judgement.
Demographic and clinical characteristics of patients with polymyalgia rheumatica (PMR)
Detection of soluble cytokines in serum
The serum was isolated from 2.5 ml blood obtained in tubes without additives from each individual and stored at −80°C until analysis.
Cytometric bead array (CBA)
The quantitative determination of proinflammatory cytokines in serum was performed using the Cytometric Bead Array (CBA) Human Inflammation kit (BD Biosciences, San Diego, California, USA). The CBA assay contained five bead populations with distinct fluorescence intensities which had been coated with capture antibodies specific for IL12p70, tumour necrosis factor (TNF)-α, IL10, IL6 and IL1β. Previously, these beads were mixed to form mixed capture beads which were then incubated together with phycoerythrin-conjugated detection antibodies and recombinant standards or test samples to form sandwich complexes. The fluorescence produced by CBA beads was measured on a FACScalibur Flow Cytometer (BD Biosciences) and analysed using Software CBA Folder Excel 98 (BD Biosciences). Detection limits were 1.9 pg/ml for IL12p70, 3.7 pg/ml for TNFα, 3.3 pg/ml for IL10, 2.5 pg/ml for IL6 and 7.2 pg/ml for IL1β.
ELISA
The quantitative determination of serum interferon γ (IFNγ) was performed by ELISA (Diaclone, Besançon, France) following the manufacturer’s instructions. The minimum detectable level of IFNγ was 0.69 pg/ml.
Detection of intracellular cytokines in circulating lymphocytes and monocytes by flow cytometry analysis
Intracellular cytokine staining is able to detect the production and accumulation of cytokines in the endoplasmic reticulum following stimulation. Cells collected in sodium heparin tubes were either polyclonally stimulated for 4 h with phorbol 12-myristate 13-acetate (PMA, 1 μg/ml; Sigma Aldrich, St Louis, Missouri, USA) and ionomycin (50 μg/ml; Calbiochem, Gibbstown, New Jersey, USA) in polystyrene tubes (lymphocytes) or activated with lipopolysaccharide (LPS) (100 μg/ml; Sigma Aldrich) in polypropylene tubes (monocytes) in the presence of brefeldin A (500 μg/ml; Sigma Aldrich) (induced or stimulated cytokine expression). Cells incubated in identical medium without stimulation (spontaneous or unstimulated cytokine expression) were used as controls.
After culture, cells were stained with peridinin chlorophyll protein-conjugated anti-CD3 antibody and fluorescein isothiocyanate (FITC)-conjugated anti-CD14 antibody to identify lymphocyte and monocyte subpopulations, respectively. Thereafter, the red blood cells were lysed with FACS lysing solution and the mononuclear cells were permeabilised using FACS Permeabilizing Solution and intracellularly stained with FITC- or phycoerythrin-conjugated cytokine-specific monoclonal antibodies (anti-IL2, anti-IFNγ and anti-IL4 for lymphocytes; anti-IL1β, anti-TNFα and anti-IL6 for monocytes). Levels of intracellular cytokine-producing cells were determined using a FACScalibur Flow Cytometer and analysed using Paint-A-Gate or Cell Quest Pro Software (all from BD Biosciences).
Detection of cytokines in cell culture supernatants
PBMCs from heparinised blood were obtained by Ficoll Histopaque 1077 (Sigma Aldrich) gradient centrifugation. PBMCs from 10 patients of each disease group and HC were cultured in RPMI 1640 and 10% FCS with PMA (100 ng/ml) and ionomycin (4 μg/ml) for 24 h. Supernatants were obtained and stored at −80°C until analysis. Release of proinflammatory cytokines (IL1β, TNFα and IL6) into the culture supernatants was determined using the CBA kit as described above. Release of IL12p70 and IFNγ into the culture supernatants was determined by ELISA (Diaclone) in accordance with the manufacturer’s instructions. The sensitivity of the ELISA kit for IL12p70 was 0.75 pg/ml.
Statistical analysis
All the statistical analysis of data was carried out using the SPSS 12.0 software (Chicago, Illinois, USA). The statistical comparisons of data between patients and controls were performed using the Mann-Whitney U test. Differences between pre- and post-treatment data were analysed by Wilcoxon signed-rank test. Differences were considered significant when p<0.05.
Results
IL6 is the more detectable proinflammatory circulating cytokine in active PMR
Previous studies suggest that PMR is characterised by a hyperproduction of IL6,4 5 7 8 9 10 11 and the results of the present study confirm this (fig 1). Circulating levels of IL6 were significantly higher in patients with active untreated PMR compared with HC. Treatment with CS was followed by a prompt and complete clinical response in all patients. As shown in fig 1, after treatment for a mean (SD) of 9.7 (4.1) weeks, the circulating IL6 levels in patients with PMR decreased significantly with most patients having IL6 levels under the detection limit. Treatment with CS was also followed by a significant decrease in circulating TNFα levels in patients with PMR (fig 1).

Serum cytokine levels in patients with active untreated polymyalgia rheumatica (PMR) and effect of corticosteroid treatment. Serum cytokine levels were assessed by cytometric beads array in 34 patients with active PMR and compared with 17 age-matched healthy controls. The effect of corticosteroid treatment was assessed in one serum sample from 14 patients with PMR in clinical remission after a mean (SD) treatment duration of 9.7 (4.1) weeks. p Values are only shown when significant. IFN, interferon; IL, interleukin; pre, active untreated disease; post, post-treatment samples; TNF, tumour necrosis factor.
IL1β, IL6 and TNFα are the major cytokines secreted by monocytes, and it would be expected that, in the case of a non-specific activation of circulating monocytes, IL1β and TNFα would also be increased. However, in agreement with previous studies,7 serum levels of IL1β and TNFα were not raised in patients with PMR compared with controls (fig 1). Interestingly, the anti-inflammatory cytokine IL10 showed higher levels in patients with PMR than in HC (p = 0.018). Finally, the circulating cytokine profile did not enable us to distinguish between patients with PMR with high or low ESR.
Cytokine production by circulating T lymphocytes in patients with PMR
As soluble cytokine levels may not reflect the real state of specific cell production, we analysed cell-specific cytokine production without ex vivo stimulation. We also examined the capacity of the cell response by measuring cell-specific cytokine production after in vitro stimulation of PBMC from patients with PMR. As shown in fig 2, circulating CD3+ lymphocytes from patients with PMR expressed similar amounts of intracellular cytokines to controls. Polyclonal in vitro stimulation showed a several fold increase in the main Th1 cytokine IFNγ and a lower response of the Th2 cytokine IL4 (fig 2). Treatment with CS did not induce significant changes in Th1 cytokines ex vivo or after in vitro stimulation (fig 2).

Intracellular T cell-derived cytokines in healthy controls and patients with polymyalgia rheumatica (PMR). Peripheral blood mononuclear cells were polyclonally stimulated for 4 h with phorbol 12-myristate 13-acetate and ionomycin in polystyrene tubes (induced or stimulated cytokine expression, right panel). Cells incubated in identical medium without stimulation acted as controls (spontaneous or unstimulated cytokine expression, left panel). After culture, cells were stained with anti-CD3 antibody and intracellularly stained with cytokine-specific monoclonal antibodies (anti-IL2, anti-IFNγ and anti-IL4). The levels of intracellular cytokine-producing cells were determined by flow cytometry. IFN, interferon; IL, interleukin.
Peripheral blood monocytes do not produce higher amounts of proinflammatory cytokines in PMR
It has been suggested that the systemic component of PMR is secondary to the production of proinflammatory cytokines by circulating monocytes.7 These observations were based on a semiquantitative PCR study and have not been confirmed. Using flow cytometry technology, we examined whether circulating monocytes are a major source of proinflammatory cytokines in patients with PMR. As shown in fig 3, the percentage of proinflammatory cytokine-producing cells ex vivo in patients with PMR was similar to the percentage in HC. In vitro stimulation with LPS showed a clear response of circulating CD14+ cells, especially in HC (fig 3). The percentage of TNFα-producing cells after in vitro stimulation was significantly lower in patients with active PMR. We did not find a significant correlation between serum and cell-specific cytokines (not shown). Treatment with CS induced a decrease in the percentage of circulating proinflammatory cytokine-producing CD14+ cells that becomes clearly significant after in vitro stimulation (fig 3).

Intracellular monocyte-derived cytokines in healthy controls and patients with polymyalgia rheumatica (PMR). Peripheral blood mononuclear cells were stimulated for 4 h with lipopolysaccharide in polypropylene tubes (induced or stimulated cytokine expression, right panel). Cells incubated in identical medium without stimulation acted as controls (spontaneous or unstimulated cytokine expression, left panel). After culture, cells were stained with anti-CD14 antibody and intracellularly stained with cytokine-specific monoclonal antibodies (anti-IL1β, anti-TNFα and anti-IL6) for monocytes. Levels of intracellular cytokine-producing cells were determined by flow cytometry. IL, interleukin; TNF, tumour necrosis factor.
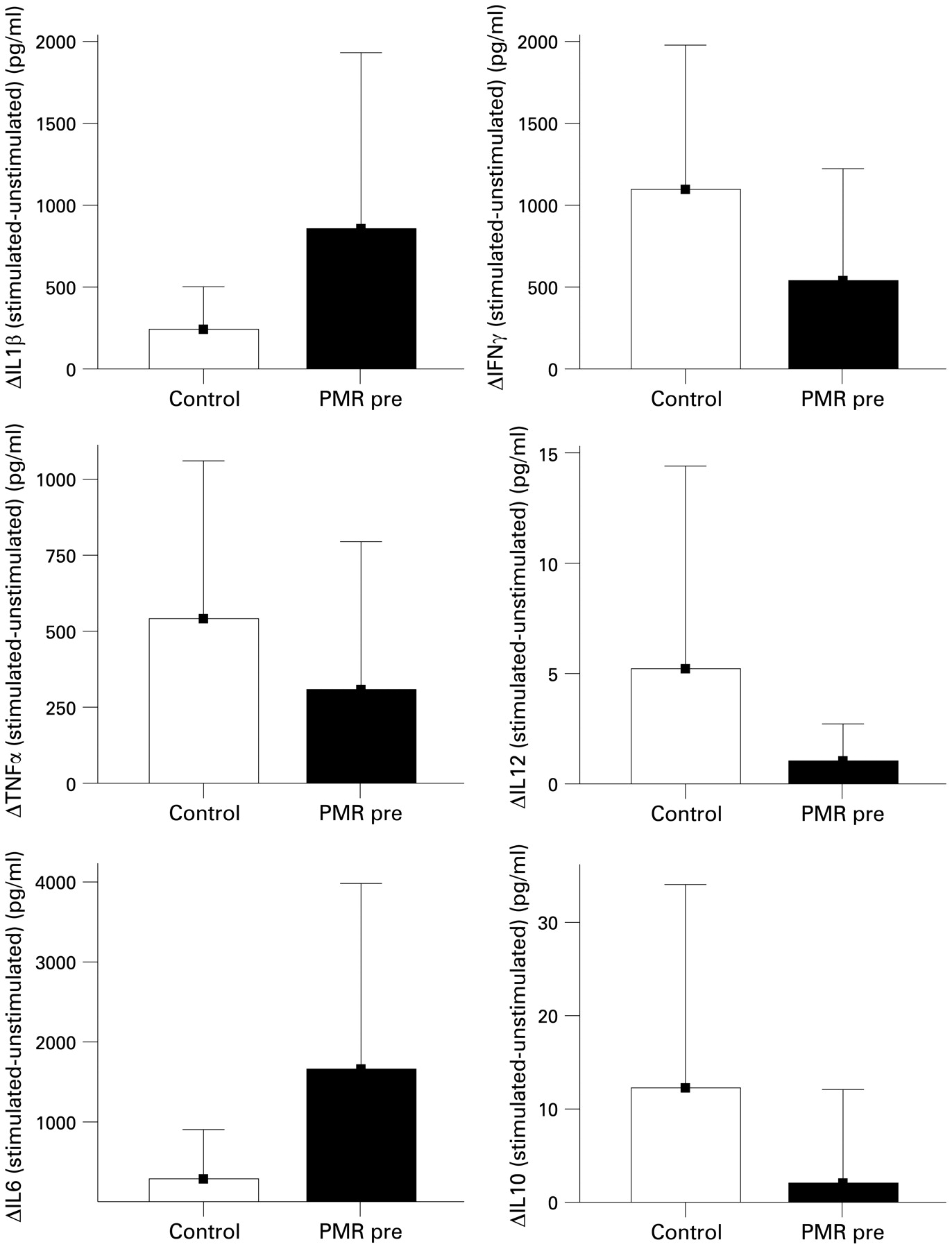
We also tested the capacity of the PBMCs of patients to secrete proinflammatory cytokines to culture supernatant upon in vitro activation. After 24 h of stimulation, no significant differences were found between patients and controls, although there was a tendency for patients with PMR to produce higher levels of IL1β and IL6 (fig 4, left panel). Interestingly, polyclonal T cell stimulation in vitro was not followed by an increase in the amount of IFNγ released. Patients with PMR secreted less IFNγ into the supernatant than age-matched HC (p = 0.07, fig 4, right panel). The same results were also found for IL12. Polyclonal T cell stimulation in vitro was followed by a significant decrease in IL12 secretion in patients with PMR.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Production of cytokines by activated peripheral blood mononuclear cells from patients with polymyalgia rheumatica (PMR). Peripheral blood mononuclear cells from 10 patients of each disease group and controls were cultured with phorbol 12-myristate 13-acetate and ionomycin for 24 h. Release of proinflammatory cytokines (left panel) and Th1 cytokines (IFNγ, IL12 and IL10, right panel) into the culture supernatant was determined using the cytometric beads array kit and ELISA, respectively. IFN, interferon; IL, interleukin; TNF, tumour necrosis factor.
Discussion
Cytokines function at a microenvironment level. However, their study is limited by the availability of inflamed tissue and the complex techniques that are needed to address this issue. Only one study has assessed the tissue levels of cytokines in PMR,12 but most studies have addressed only the levels in serum or plasma.5 7 8 9 10 11 13 14 15 16 17 In this study we have combined different strategies to study circulating cytokines in patients with PMR in order to examine whether there is an underlying dysregulation of cytokine secretion independent of tissue inflammatory effects. To this end, we have measured a wide panel of circulating cytokines at the serum level, intracellular cytokines by flow cytometry, and we have also measured the levels of cytokines in supernatants of in vitro stimulated PBMCs. Furthermore, we have been able to identify the main cellular source of cytokines at the peripheral blood compartment, the state of activation of PBMCs during the active phase of the disease, and also the capacity of the response of PBMCs to in vitro stimuli. Finally, the study of patients after clinical remission with CS treatment also allowed us to examine the main effects of treatment on circulating cytokines.
We confirmed that patients with PMR are characterised by an increase in serum levels of IL6.5 7 8 9 10 11 The central role of IL6 in PMR was illustrated by the rapid clinical response to CS treatment which was followed by a parallel decrease in serum levels of this cytokine. Alternatively, it may be that the main source of IL6 is not the activated circulating monocyte but other cell types that selectively or predominantly produce IL6. The levels of other proinflammatory cytokines such as IL1β and TNFα were within a very low range, and differences may reflect different pathogenic pathways or differences in the polymorphisms of genes within the IL1 pathway that influence circulating cytokine levels.18 19 In fact, IL1RN*2 homozygosity is significantly higher in patients with PMR than in HC.20 21
Despite the advantages of measuring circulating levels of cytokines, there are also a number of drawbacks.22 23 The levels of circulating cytokines may be affected by receptor binding, cytokine metabolism, processing technique and the type of test used for measurement.23 Furthermore, although cytokines also act as endocrine mediators, their major function is to act locally at the cellular level. Serum cytokine levels therefore provide, at best, an indirect measure of cytokine function and may not reflect the role of a cytokine in disease pathogenesis.23 24 25 26
This is the first study in which cytokines have been detected at the single cell level in patients with PMR. Although we did not assess intracellular cytokines at the site of inflammation, PMR is a systemic process characterised by a significant acute phase response so serum cytokines and blood cytokine-producing cells might be expected to reflect the systemic component of the disease. It is still unclear whether the increase in cytokine production is caused by an increase in the numbers of cytokine-producing cells or by the enhanced ability to produce cytokines. We also compared serum cytokines with cell-specific cytokine production without ex vivo stimulation. The reasoning behind this comparison is that patients with an increased acute phase response such as those with PMR might be expected to have in vivo stimulated cells.23
It has been suggested that PMR has a systemic component that is at least partially independent of the tissue component and is mediated by the production of IL6 by circulating monocytes.4 Our findings showed ex vivo activation in both patients and HC. Spontaneous ex vivo cytokine production by PBMC has been reported in healthy individuals, especially for IL6.22 23 It has been shown that the correlation of serum and cytokine-specific cells is weak.23 In fact, this correlation may be negative, indicating that serum and cytokine-specific cells measure different factors.22 27 Furthermore, some cytokines such as IL6 might be produced by circulating immune cells and also by other non-blood cell types. Thus, serum levels might not necessarily reflect the production of circulating immune cells.28 In this study we found no correlation between serum and intracellular cytokine production. We therefore hypothesise that the increased levels of IL6 found in patients with PMR are not the result of IL6 production by circulating monocytes, and it is reasonable to assume that the major production of proinflammatory cytokines is located at the site of the inflammatory process7 or in blood cells different from circulating CD14+ cells.
We also examined intracellular cytokine production and extracellular cytokine secretion in vivo and after in vitro stimulation. The presence of spontaneous cytokine production ex vivo implies prior in vivo stimulation. In theory, if cells have been stimulated in vivo, secondary ex vivo induction could lead to in vitro apoptosis and obscure the role of the studied cell-specific cytokine.22 Cytokine expression is strongly dependent on the specific activation stimulus29 and also on the duration of in vitro stimulation,30 and the results must therefore be interpreted accordingly.
Despite these considerations, our in vitro results yielded the following conclusions. In vitro stimulation showed no significant difference in the induction of proinflammatory cytokines in HC, which may suggest that the proinflammatory cytokines studied here are not crucial in the pathogenesis of PMR.24 Alternatively, the lack of significant differences in the response of circulating monocytes may also reflect the hyporesponsiveness of previously activated T lymphocytes. The latter hypothesis might be supported by the marked reduction in IFNγ secretion following polyclonal activation of T cells in PBMC from patients with PMR. Although we cannot exclude a gene transcription defect, the reduction in IFNγ secretion does not appear to be attributable to reduced intracellular protein production. In fact, although intracellular cytokine production was assessed at different time intervals from protein secretion (fig 2), there were no differences between patients and controls. Furthermore, a selective peripheral impairment of the Th1 response might also be confirmed by the similar results found for IL12, another Th1 cytokine produced by a different cell type. These findings could have important pathogenic implications. It has been shown in animal models that IFNγ can reduce the inflammatory response,31 and the reduced peripheral Th1 response may represent an increased risk for infections.32 On the other hand, reductions in the peripheral Th1 response may prime inflamed tissues to a prolonged and exacerbated inflammation.29
A detailed knowledge of the cellular source and the role of cytokines in the pathogenesis of PMR might have therapeutic implications. Although CS will continue to be the main therapeutic agents, their toxicity and the existence of a subgroup of patients with a refractory course make it necessary to search for alternatives. In this regard, the rapid development of more selective therapeutic agents—especially those directed at blocking proinflammatory cytokines—has opened up new treatment options. Thus, blocking IL633 may represent a major step towards avoiding the use of prolonged CS treatment in this aged population.
In summary, active PMR is characterised by increased serum levels of IL6—but not of other proinflammatory cytokines—that are rapidly suppressed by CS treatment. As circulating monocytes do not show increased production of proinflammatory cytokines, IL6 is probably mainly produced in the inflamed tissue. The discordance found between serum levels and cytokine-producing cells may have important consequences for the understanding of the pathogenesis of PMR.
Acknowledgments
The authors thank Iñaki Beares (supported by a grant for Research Aid from Schering-Plough, Spain), Marta González, Maria San Martín and Ainhoa Bolívar (supported by Fundación Marqués de Valdecilla-IFIMAV) for their helpful technical assistance, and all the patients and controls included in the present study and the consultants of the Rheumatology Divisions who monitored them.
REFERENCES
Footnotes
Funding This work was supported by grants from Fondo de Investigación Sanitaria (05/0475), Fundación Marqués de Valdecilla and Fundación Mutua Madrileña. LA-R was supported by a grant for Research Aid from Wyeth Pharma (Spain).
Competing interests None.
Ethics approval All the patients and controls gave signed informed consent and the study was approved by the regional ethics committee.
Provenance and Peer review Not commissioned; externally peer reviewed.