Article Text

Abstract
Background: Although familial clusters of Barrett’s oesophagus and oesophageal adenocarcinoma have been reported, a familial predisposition to these diseases has not been systematically investigated.
Aims: To determine whether Barrett’s oesophagus and oesophageal (or oesophagogastric junctional) adenocarcinoma aggregate in families.
Patients and methods: A structured questionnaire eliciting details on reflux symptoms, exposure history, and family history was given to Caucasian case (n=58) subjects with Barrett’s oesophagus, oesophageal adenocarcinoma, or oesophagogastric junctional adenocarcinoma, and to Caucasian control (n=106) subjects with symptomatic gastro-oesophageal reflux disease without Barrett’s oesophagus. Reported diagnoses of family members were confirmed by review of medical records.
Results: The presence of a positive family history (that is, first or second degree relative with Barrett’s oesophagus, oesophageal adenocarcinoma, or oesophagogastric junctional adenocarcinoma) was significantly higher among case subjects compared with controls (24% v 5%; p<0.005). Case subjects were more likely to be older (p<0.001) and male (74% v 43% male; p<0.0005) compared with control subjects. In a multivariate logistic regression analysis, family history was independently associated with the presence of Barrett’s oesophagus, oesophageal adenocarcinoma, or oesophagogastric junctional adenocarcinoma (odds ratio 12.23, 95% confidence interval 3.34–44.76) after adjusting for age, sex, and the presence of obesity 10 or more years prior to study enrolment.
Conclusions: Individuals with Barrett’s oesophagus, oesophageal adenocarcinoma, or oesophagogastric junctional adenocarcinoma are more likely to have a positive family history of Barrett’s oesophagus, oesophageal adenocarcinoma, or oesophagogastric junctional adenocarcinoma than individuals without Barrett’s oesophagus, oesophageal adenocarcinoma, or oesophagogastric junctional adenocarcinoma. A positive family history should be considered when making decisions about screening endoscopy in patients with symptoms of gastro-oesophageal reflux.
- Barrett’s oesophagus
- oesophageal adenocarcinoma
- oesophagogastric junctional adenocarcinoma
- gastro-oesophageal reflux disease
- BO, Barrett’s oesophagus
- OAC, oesophageal adenocarcinoma
- OGJAC, oesophagogastric junctional adenocarcinoma
- FBQ, Familial Barrett’s Questionnaire
- GORD, gastro-oesophageal reflux disease
Statistics from Altmetric.com
- Barrett’s oesophagus
- oesophageal adenocarcinoma
- oesophagogastric junctional adenocarcinoma
- gastro-oesophageal reflux disease
- BO, Barrett’s oesophagus
- OAC, oesophageal adenocarcinoma
- OGJAC, oesophagogastric junctional adenocarcinoma
- FBQ, Familial Barrett’s Questionnaire
- GORD, gastro-oesophageal reflux disease
The incidence of oesophageal adenocarcinoma (OAC) and oesophagogastric junctional adenocarcinoma (OGJAC) in the USA has increased strikingly in the past two decades.1,2 In Caucasians, the incidence of OAC has more than tripled, surpassing the incidence of squamous cell cancer. The prognosis for patients with cancer of the oesophagus has remained poor, with 12 200 patients dying annually of cancer related causes.3
Most OAC/OGJACs are believed to originate in Barrett’s oesophagus (BO).4–8 Prospective studies have estimated the risk of developing oesophageal adenocarcinoma to be 30–125 times higher in patients with BO compared with the general population.9–13 BO is closely linked to gastro-oesophageal reflux disease (GORD).4,14–16 The prevalence of BO is less than 1% in patients without GORD symptoms but is approximately 10% in those with GORD.15–18 BO and OAC/OGJAC are also more common in Caucasians.18 Obesity and cigarette smoking are well established risk factors for the development of OAC/OGJAC.19–23 Alcohol use24,25 and use of medications that relax the lower oesophageal sphincter26 have also been associated with OAC/OGJAC in some studies.
Although environmental factors associated with BO and OAC/OGJAC have been identified, the possibility of familial or genetic influences has not been systematically investigated. Numerous case reports have documented familial clusters of BO or OAC/OGJAC.27–33 In these reports, the frequency of BO has been more than 20% and the frequency of GORD has been approximately 40% among relatives.30–33 Indirect evidence for a possible genetic effect also comes from studies that have documented an increased prevalence of GORD among family members of patients with BO and OAC/OGJAC.34,35 The aim of this study was to determine whether patients with BO, OAC, or OGJAC have an increased likelihood of having a positive family history of BO and/or OAC/OGJAC compared with control patients with GORD alone.
MATERIALS AND METHODS
Basic study design
The study population was recruited from patients undergoing endoscopy at a tertiary care university hospital. All eligible patients with BO, OAC, or OGJAC seen between November 1999 and October 2000 and control patients with GORD seen between May 2000 and October 2000 were invited to participate (limitations in the availability of research personnel limited the recruitment of consecutive control subjects to the second half of the study period). Enrolled subjects were given a Familial Barrett’s Questionnaire (see following section on FBQ). As individuals may not be fully cognisant of their relatives’ medical histories, study subjects were encouraged to take the questionnaire home, discuss family history with relatives, and then return the questionnaire by mail. Permission was obtained from all subjects to contact their relatives. Attempts were made to confirm the histological diagnosis for all family members reported to have a history of BO or oesophageal cancer. The institutional review board for human investigation approved this protocol.
Study definitions
BO was defined as a 3 cm or longer segment of salmon coloured mucosa in the oesophagus at endoscopy and the presence of intestinal metaplasia on biopsies. OAC was defined as adenocarcinoma arising in the oesophagus and OGJAC was defined as adenocarcinoma arising at the gastro-oesophageal junction with involvement of the oesophagus. The study pathologist (JW) reviewed biopsies for all case and control patients to confirm the diagnosis. Obesity was defined as a body mass index (weight (kg)/height2 (m2)) ≥27.8 kg/m2 for males and ≥27.3 kg/m2 for females.36
BO, OAC, or OGJAC case group
Case subjects were recruited from patients with a known diagnosis of BO undergoing surveillance endoscopy, patients with a new diagnosis of BO, patients with a known diagnosis of OAC/OGJAC undergoing a palliative or staging endoscopic procedure, and patients with a new diagnosis of OAC/OGJAC seen in the endoscopy suite during the one year recruitment period. Eligible patients were men or women, aged 18 years or older, confirmed histological diagnosis of BO, OAC, or OGJAC, able to give informed consent, with no history of radiation therapy to the chest, or history of chemotherapy in the year preceding the initial diagnosis of BO, OAC, or OGJAC. All eligible case subjects who did not return their questionnaires were contacted once by telephone or mail and encouraged to participate in the study.
GORD control group
Control patients were identified from an open access outpatient endoscopy system that has been in place since 1993 and from outpatients seen in the gastroenterology clinic. In this open access system, a detailed form is provided to primary physicians requesting demographic data, details on coexisting illnesses, and indications for endoscopic referral. During the six month recruitment period, all patients undergoing endoscopy for evaluation of GORD symptoms (one of the approved indications for endoscopy referral listed on the open access form) who had no evidence of BO, OAC, or OGJAC were contacted for study participation. Eligible control subjects were men or women, aged 18 years or older, able to give informed consent, with no history of radiation therapy to the chest, or history of chemotherapy in the year preceding endoscopy. All eligible control subjects who did not return their questionnaires were contacted once by telephone or mail and encouraged to participate in the study.
Familial Barrett’s Questionnaire (FBQ)
The FBQ is a structured 11 page instrument consisting of three sections—reflux symptoms, exposure, and family history. Reflux symptom information is obtained using a modified version of the standardised Mayo reflux symptom questionnaire developed by Locke et al (used with permission).37 The questions are limited to symptoms of heartburn, acid regurgitation, and trouble swallowing. Patients who are receiving GORD therapy are asked to rate the frequency and severity of their symptoms as if they are not on medications. The exposure section elicits details on smoking history, alcohol use, education, ethnicity, current weight and height, as well as weight and height at 1, 5, 10, and 20 years prior to study enrolment. The family history section is a modification of an instrument used by the Family Studies Core at Case Western Reserve University in an ongoing genetic study. Although the instrument has not been formally validated, it has been used by genetic counsellors for more than five years to obtain a detailed family history of colon polyps, colon cancers, and other cancers from patients. The instrument was specifically modified for this study to ask structured questions regarding family history of BO, oesophageal cancer, and other cancers. A detailed history is elicited for all first degree relatives and any affected second degree relatives. Contact information for affected relatives and permission to contact them are also obtained.
On receipt of FBQs from study participants, questionnaires were reviewed for incomplete or missing information. Follow up phone calls were made as needed to obtain complete information on each study subject.
Confirmation of family history
Efforts were made to confirm diagnoses for all first and second degree relatives reported with BO, oesophageal cancer, or oesophagogastric junctional cancer. After permission was obtained, the reported affected relatives (next of kin, if affected relative was deceased) were contacted and a signed release of medical information was requested. Endoscopy and pathology reports were then requested from the institution where the affected relatives received medical care. Medical records departments were contacted by telephone at least twice before reports were classified as unavailable. For relatives reported as having oesophageal cancer, death certificates were examined when medical reports could not be obtained. Positive family history was defined as a first or second degree relative with BO, OAC, or OGJAC whose diagnosis was confirmed or whose endoscopy and histology reports could not be obtained from hospital archives. If the relative reported as having oesophageal cancer had squamous cell cancer or a cancer that did not involve the oesophagus or cardia, the family history was classified as negative.
Statistical analysis
Each risk factor was initially investigated by estimating a crude odds ratio and evaluating simple proportions for contingency tables. Statistical significance was assessed using Pearson’s χ2 test, where differences with p values <0.05 were considered statistically significant. Continuous variables (for example, age) were converted to categorical variables for this preliminary analysis. GORD symptoms and family size distributions were compared for the two groups, in addition to exposure factors such as age and sex.
Multivariate logistic regression analysis was used to assess the relationship between family history of BO or OAC and case/control status, adjusting for potentially confounding or effect modifying variables. Risk factors that were considered as potential confounders or effect modifiers included alcohol consumption score (defined as: 1, <1 drink; 2, 1–5 drinks; 3, 6–10 drinks; and 4, >10 drinks per week), smoking status, coffee consumption, obesity at 0, 1, 5, 10, and 20 years prior to study evaluation, age, and sex. Risk factors with a p value <0.05 were considered statistically significant, and retained in the model. Two way interactions and higher order terms were considered to evaluate effect modification. Risk factors that changed the coefficient for the family history indicator by more than 10% were considered confounders and also retained in the model, regardless of statistical significance of the confounder. All analyses were performed using the Splus2000 software package (Mathsoft Inc., Seattle, Washington, USA).
RESULTS
Demographics
FBQs were returned by 70/92 (76%) cases (BO/OAC/OGJAC) and 156/238 (66%) control GORD patients. The ethnicity distribution was significantly different (p<0.001) between the groups, as 58 (83%) of the case patients and 106 (68%) of the control GORD patients were Caucasian. Because of the small number of non-Caucasian case subjects (n=12), and the large difference in the proportion of African-American subjects between the two groups (28% of control patients v 0% of case patients), we restricted our analysis to Caucasians. However, there was no significant difference in the findings when all subjects were considered (data not shown). Of the 58 Caucasian cases, 35 had BO and 23 had OAC/OGJAC (16 OAC and seven OGJAC). Patients with BO or OAC/OGJAC were significantly older and more likely to be male compared with control patients with GORD symptoms (table 1).
Age and sex distributions of the case group with Barrett’s oesophagus, oesophageal adenocarcinoma, and oesophagogastric junctional adenocarcinoma, and of the control group with gastro-oesophageal reflux disease symptoms
GORD symptoms
The presence and duration of GORD symptoms (heartburn, acid regurgitation, or dysphagia) was not statistically significantly different between the case and control groups for most of the variables considered (table 2). The exception was that heartburn was less frequent and less severe in the case group compared with the control group.
Duration, severity, and frequency of gastro-oesophageal reflux disease symptoms* in 58 case subjects and 106 control subjects
Other exposure history
The distribution of exposure risk factors is shown in table 3. Case subjects were more than twice as likely to be current or former smokers than GORD control subjects. There was also a tendency for greater alcohol consumption among case subjects.
Distribution of risk factors in case subjects with Barrett’s oesophagus, oesophageal adenocarcinoma, and oesophagogastric junctional adenocarcinoma, and in the control group with gastro-oesophageal reflux disease symptoms
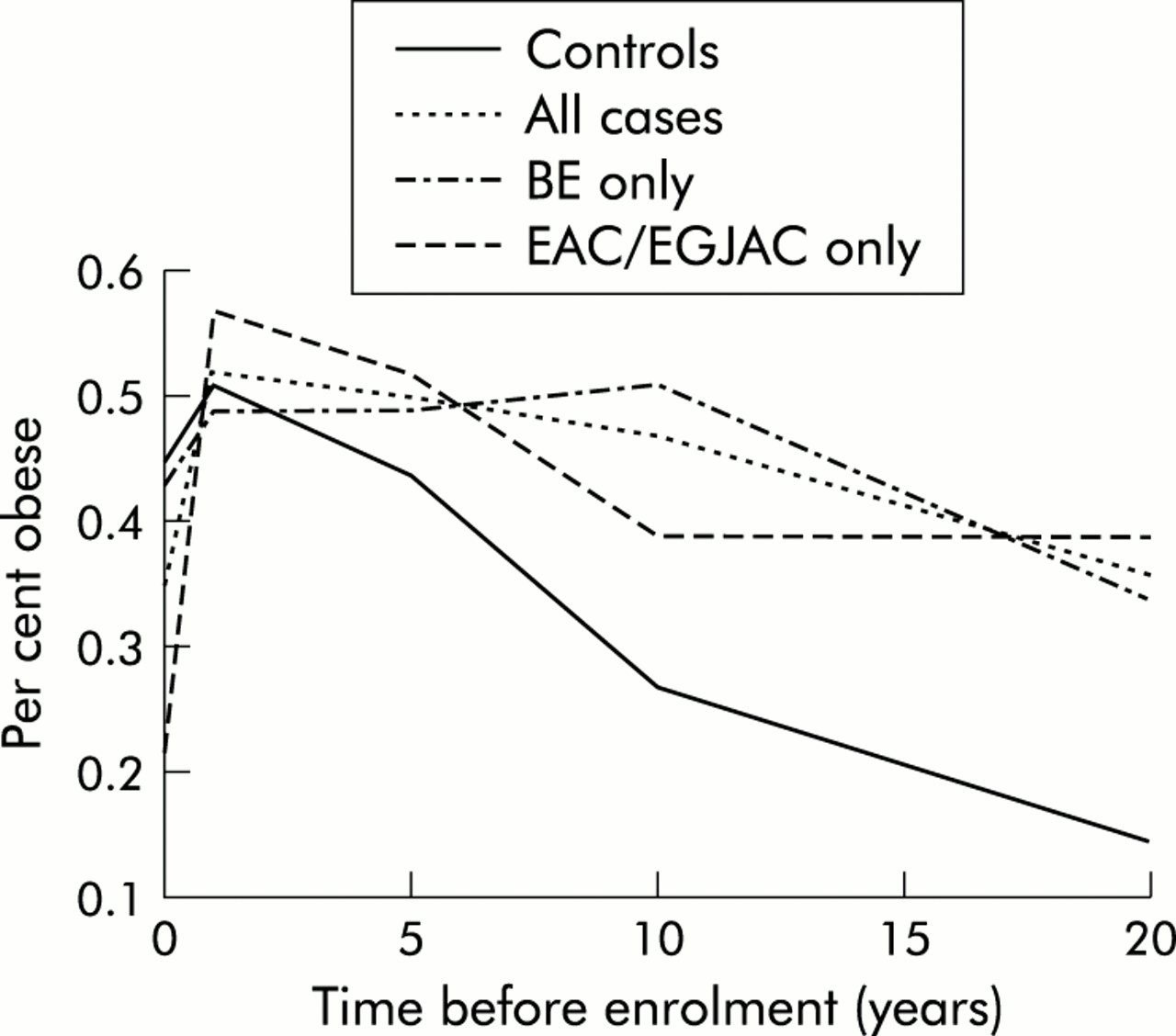
The difference in the obesity indicator between case and control subjects depended on the time since enrolment. There was no significant difference in obesity at the time of study enrolment, one year ago, and five years ago. However, case subjects were significantly more likely than control subjects to be obese 10 years and 20 years prior to study enrolment. There was a concern that the obesity measures might be influenced by disease status as individuals with OAC/OGJAC are likely to lose weight due to their disease and treatment. Therefore, we evaluated obesity for BO and OAC/OGJAC cases separately (fig 1). As shown in this figure, the percentage of patients who were obese was similar for BO and OAC/OGJAC cases with the exception of the current year where the percentage of OAC/OGJAC patients who were obese decreased dramatically. Therefore, obesity indicators at times prior to the present better reflect the risk for the case group. In the multivariate analysis, obesity indicators at 10 years and 20 years prior to enrolment were considered.

{kind=link}
Relationship between the proportion of obese subjects and time prior to study enrolment in all control subjects, all case patients, in patients with Barrett’s oesophagus (BO) alone, and in those with oesophageal adenocarcinoma (OAC) and oesophagogastric junctional adenocarcinoma (OGJAC).
Family size distribution
Having a family history of disease, in some regard, depends on the number of relatives for each individual. In addition, as age and sex may also be related to the presence of disease, it is important to consider age and sex distributions for relatives also. To ensure that the family history variable was comparable between the two groups, we compared family size and relative age and sex distributions for the case and control groups for siblings and offspring (table 4). Age distribution was not measured for the offspring. Finally, 25% of the control subjects had second degree relatives that were considered in this study compared with 29% of case subjects. Age and sex distributions for second degree relatives are also not known. Overall, family size, sex, and age distributions were similar for cases and controls in this study, suggesting that a family history indicator was comparable for the two groups.
Distribution of siblings and offspring in the Caucasian case group with Barrett’s oesophagus, oesophageal adenocarcinoma, and oesophagogastric junctional adenocarcinoma, and in the control group with gastro-oesophageal reflux disease symptoms
Family history
A positive family history (that is, a first or second degree relative with BO, OAC, or OGJAC) was reported by 16 case subjects and 11 control subjects. However, review of the medical records revealed that two of these reportedly affected case relatives and six control relatives did not have BO, OAC, or OGJAC (four had squamous cell cancer of the oesophagus, two had erosive oesophagitis, and two had non-oesophageal cancers). A positive family history of BO, OAC, or OGJAC was confirmed for 10 case patients and one control patient. Archived hospital records were no longer available for relatives of another four cases and four controls who had reported a positive family history. After excluding those relatives who were definitively found not to have BO, OAC, or OGJAC, a positive family history was reported by 14 (24%) of the case group compared with five (5%) of the control group (p=0.0005) (table 3). Specifically, 10/35 (29%) patients with BO and 4/23 (17%) patients with OAC/OGJAC reported a positive family history (p values of 0.0003 and 0.087 for respective comparisons with the control group). Of the 10 BO patients with a positive family history, five had a first degree relative with BO, one had a second degree relative with BO, one had a first degree relative with OAC, one had a second degree relative with OGJAC, one had two first degree relatives with OGJAC, and one had a first degree relative with OAC and two second degree relatives with OAC/OGJAC. Of the four OAC/OGJAC patients with a positive family history, one had a first degree relative with BO, two had a second degree relative with BO, and one had a first degree relative and a second degree relative with OAC/OGJAC. No control subject reported more than one relative with BO or OAC/OGJAC.
Multivariate analysis
A multivariate logistic regression analysis demonstrated that older age, male sex, positive family history, obesity 10 years prior to enrolment, and alcohol consumption were independently associated with the presence of BO, OAC, or OGJAC in Caucasians (table 5).
Multivariate analysis of factors independently associated with Barrett’s oesophagus, oesophageal adenocarcinoma, and oesophagogastric junctional adenocarcinoma in Caucasian patients
DISCUSSION
This study demonstrated that Caucasian patients with BO, OAC, or OGJAC were 12 times more likely to have a first or second degree relative with BO, OAC, or OGJAC than Caucasian patients with GORD symptoms. Although the number of patients was limited, this familial effect appeared to be present approximately equally in those who had BO and those who had OAC/OGJAC. Prior case reports have documented large familial clusters of these diseases.27–33 The findings of the present investigation are the first systematic demonstration of a significant familial component to BO and OAC/OGJAC.
BO, OAC, and OGJAC were examined in combination because of existing evidence that the three diseases are closely related. Firstly, considerable evidence indicates that OAC and OGJAC originate in Barrett’s epithelium.4–8 Secondly, risk factors for these diseases are similar.14–26 Finally, several common molecular changes that characterise metaplastic Barrett’s epithelium and OAC as well as OGJAC have been identified.38 Two prior population based studies that investigated a familial predisposition for oesophageal adenocarcinoma in much larger cohorts reported that heredity does not contribute to the risk of oesophageal adenocarcinoma.39,40 These studies39,40 may have failed to identify an association because they confined themselves to determining the presence of cancer in first degree relatives and did not investigate the presence of BO in family members. These two prior studies39,40 also did not confirm the histology or location of reported cancers in family members.
Prior reports have suggested that an autosomal dominant gene is responsible for familial BO.30–33 Numerous genes that determine susceptibility to the development of cancers as well as a gene that determines susceptibility to GORD in the paediatric population41 have been identified. At this point, one can only speculate whether genes that may be responsible for familial BO fall into one of these categories. Definitive establishment of a genetic effect and characterisation of the gene(s) that confers susceptibility to BO requires a full scale genetic segregation analysis of a much larger patient population.
Thorough investigation requires the use of an appropriate instrument as well as encouraging patients to discuss family medical histories with their relatives. Conceivably, the 22 BO, OAC, or OGJAC patients who did not return their questionnaires were less likely to have a family history than the study participants, and the prevalence of a positive family history in the study population may have been overestimated. However, even if the 22 non-participating cases who did not return their questionnaires were included in the analysis and considered to have a negative family history, a significant association between positive family history and presence of BO, OAC, or OGJAC would still exist (p=0.0092). The prevalence of family history may also be subject to the unavoidable bias of a study population at a referral institution. The proportion of subjects with OAC in the case group was probably high because of referral patterns.
Confirmation of the diagnosis was an important component of this study. When histology reports on reported oesophageal cancers in family members were obtained, four relatives of control GORD subjects were found to have squamous cell cancer of the oesophagus whereas relatives of the case group almost invariably had OAC or OGJAC, further supporting the familiality of OAC/OGJAC. However, the findings are potentially subject to recall bias. It is possible that control subjects were more likely than case subjects to underreport their family history. However, patients with GORD symptoms undergoing endoscopy are probably more likely to understand the complications of GORD than healthy control subjects. Therefore, the use of patients with GORD symptoms as the control group as opposed to an asymptomatic healthy control group helps to minimise recall bias. Subjects whose familial diagnosis could not be validated because of the unavailability of medical records were included in the analysis because a substantial proportion (80%) of control subjects with a reported positive family history were in this group. The association of a positive family history and presence of BO, OAC, or OGJAC was stronger if only validated family histories were analysed. In fact, the association was still significant, even if it was assumed that all four relatives of the control subjects whose history could not be confirmed had BO, OAC, or OGJAC and all four relatives of the case subjects whose history could not be confirmed did not have BO, OAC, or OGJAC (p=0.018).
Familial aggregation was assessed in prevalent as well as incident cases in this study. Clearly, family members of patients with cancers might be more likely to be evaluated for GORD symptoms and might undergo endoscopic evaluation more frequently than family members of patients with GORD. It is difficult, if not impossible, to eliminate this bias when investigating familial aggregation of uncommon human diseases. A study confined to incident cases of BO, OAC, or OGJAC would avoid this bias but the resources and time required to identify a sufficiently large cohort would be prohibitive. The difference in familial aggregation only became apparent when the diagnoses in family members were validated.
Other studies have reported an association of obesity and smoking with BO and OAC/OGJAC.19–23 Alcohol use has been associated with OAC/OGJAC in some studies24,25 but not in others.22,23 Use of medications that decrease lower oesophageal sphincter pressure has also been recently associated with OAC/OGJAC.26 Use of these medications was not specifically investigated in the present study because this association had not been recognised prior to study initiation. In the present study, smoking was a weak risk factor that did not confound the association between case status and positive family history. Alcohol use, on the other hand, was weakly associated with BO and OAC/OGJAC and negatively confounded the association between case status and positive family history in the multivariate analysis. Obesity differences between the groups were only detected when the history of obesity 10 and 20 years prior to study enrolment was examined, suggesting that the timing of exposure and the duration of obesity play a role in the development of BO and OAC/OGJAC.
The association of GORD with BO and OAC/OGJAC is well established.14–18 Outpatients with GORD undergoing diagnostic endoscopy were felt to be the best control group for this study because their endoscopic findings were available, they likely represented the more severe spectrum of GORD, and they could be recruited at the time of endoscopy. The two groups were fairly well matched in terms of GORD symptoms. The only significant difference between the two groups was that although heartburn tended to be of longer duration it was significantly more frequent and severe in the control GORD group. This difference may be related to a decrease in acid sensitivity known to occur in patients who are older and have BO42,43 or it may reflect the fact that BO and OAC/OGJAC are increasingly being recognised in patients who have no symptoms of GORD.
Increasing age, male sex, and ethnicity are known risk factors for the development of BO and OAC/OGJAC.18 For the purposes of this study, the analysis was restricted to subjects who defined their ethnicity as Caucasian in their response on the FBQ to avoid biases related to major ethnicity differences between the case and control groups. The vast majority (83%) of the case subjects were included in this group. When looking for familial effects in diseases it is also extremely important that the compared groups are matched in terms of family size, as in this study. As expected, the multivariate analysis demonstrated that age and male sex were independently associated with BO, OAC, and OGJAC. Much larger studies would be required to determine whether familial aggregation for BO and OAC/OGJAC also exists in non-Caucasian populations.
In conclusion, this study demonstrates that BO, OAC, and OGJAC aggregate in Caucasian families. Current recommendations for endoscopic screening are based on age, sex, ethnicity, and duration and severity of GORD symptoms. The results support the use of a positive family history of BO, OAC, or OGJAC as an additional factor when deciding whether to perform a diagnostic endoscopy in patients with GORD symptoms. Furthermore, it is important to elicit a careful family history to recognise the presence of familial BO. Large full scale segregation studies are required to determine the exact nature of this familial aggregation, which is postulated to have a genetic basis.
Acknowledgments
This project was funded by the ASGE Endoscopic Research Award. Dr Chak is also supported by a Midcareer Investigator Award in Patient Oriented Research from the National Institute of Health.