Article Text

Abstract
Objective Reported malignant progression rates for low-grade dysplasia (LGD) in Barrett's oesophagus (BO) vary widely. Expert histological review of LGD is advised, but limited data are available on its clinical value. This retrospective cohort study aimed to determine the value of an expert pathology panel organised in the Dutch Barrett's Advisory Committee (BAC) by investigating the incidence rates of high-grade dysplasia (HGD) and oesophageal adenocarcinoma (OAC) after expert histological review of LGD.
Design We included all BO cases referred to the BAC for histological review of LGD diagnosed between 2000 and 2011. The diagnosis of the expert panel was related to the histological outcome during endoscopic follow-up. Primary endpoint was development of HGD or OAC.
Results 293 LGD patients (76% men; mean 63 years±11.9) were included. Following histological review, 73% was downstaged to non-dysplastic BO (NDBO) or indefinite for dysplasia (IND). In 27% the initial LGD diagnosis was confirmed. Endoscopic follow-up was performed in 264 patients (90%) with a median follow-up of 39 months (IQR 16–72). For confirmed LGD, the risk of HGD/OAC was 9.1% per patient-year. Patients downstaged to NDBO or IND had a malignant progression risk of 0.6% and 0.9% per patient-year, respectively.
Conclusions Confirmed LGD in BO has a markedly increased risk of malignant progression. However, the vast majority of patients with community LGD will be downstaged after expert review and have a low progression risk. Therefore, all BO patients with LGD should undergo expert histological review of the diagnosis for adequate risk stratification.
- Oesophageal Cancer
- Barrett's Carcinoma
- Barrett's Oesophagus
- Dysplasia
- Histopathology
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
-
Low-grade dysplasia (LGD) has previously been shown to be an independent risk factor for developing high-grade dysplasia (HGD) or oesophageal adenocarcinoma (OAC) in patients with Barrett's oesophagus (BO).
-
Previous studies have shown highly variable malignant progression rates for BO patients with LGD.
-
Expert pathology review of community LGD cases is recommended, but the quality of expert pathology in BO is highly variable.
What are the new findings?
-
A panel of expert pathologists will downstage 73% of community LGD diagnoses to non-dysplastic BO (NDBO) or indefinite for dysplasia (IND) with a low risk of malignant progression (0.6% and 0.9% per patient-year, respectively).
-
Patients in whom the community LGD diagnosis was confirmed by the expert pathology panel had a markedly increased risk of malignant progression (9.1% per patient-year; 5-year cumulative HGD/OAC incidence of 33.3%).
How might it impact on clinical practice in the foreseeable future?
-
In all BO patients with a community LGD diagnosis, the histopathological slides should be reviewed by a panel of expert pathologists.
-
Patients who are downstaged to NDBO or IND after expert pathology review should be managed as true non-dysplastic Barrett's patients, extending the surveillance interval to 3–5 years.
-
BO patients with a confirmed diagnosis of LGD should be referred to expert centres to undergo strict endoscopic follow-up or be considered for prophylactic ablation therapy.
Introduction
Barrett's oesophagus (BO) is the only known precursor to oesophageal adenocarcinoma (OAC) and is defined by replacement of the squamous epithelial lining of the distal oesophagus by columnar epithelium.1 ,2 Although some guidelines do not require the presence of intestinal metaplasia for the diagnosis of BO, most guidelines (eg, from the USA and the UK) require the presence of intestinal metaplasia as a necessary prerequisite for surveillance since previous studies have shown that the risk of malignant progression is considerably lower in BO without intestinal metaplasia.1 ,3–5 Malignant progression in BO is thought to be a multi-step process, which develops through subsequent grades of dysplasia classified as non-dysplastic BO (NDBO), low-grade dysplasia (LGD) and high-grade dysplasia (HGD) resulting in cancer.1 ,2 Patients with HGD or OAC are offered a therapeutic intervention with either endoscopic therapy or surgery depending on local expertise, patient fitness and depth of invasion.1 ,5 ,6 Patients with LGD are considered to have an increased risk of malignant progression over patients with no dysplasia and are offered intensified endoscopic surveillance every 6–12 months or may sometimes undergo endoscopic therapy.1 ,5 For patients with NDBO, current guidelines recommend a 3–5 year surveillance interval. In patients with a diagnosis of indefinite for dysplasia (IND), it is recommended that antireflux therapy is optimised and endoscopy is repeated in 6 months. If subsequent biopsies demonstrate no definite dysplasia, patients should be managed as NDBO.5
Currently, surveillance and treatment decisions are solely based on conventional histopathological assessment of surveillance biopsies. Although recent research into objective biological markers for progression is promising, clinical implementation of a biomarker panel is far away and histology is the only risk stratification tool available.7–9
Risk stratification according to dysplasia grade is nevertheless fraught with uncertainty as data on malignant progression rates for LGD are highly diverging, ranging from 0.6% to 13.4% per patient-year.10–20 The cause of these variable progression rates is twofold. First, most studies that have investigated progression risk for LGD patients suffer methodological shortcomings. Sample sizes are relatively small, quality of endoscopic follow-up data is limited and several studies were performed in tertiary care settings, resulting in referral bias. However, the most important issue seems to be reliability of the baseline LGD diagnosis. Community pathologists frequently overdiagnose LGD, as previously demonstrated by our group.11 In that study, a consensus diagnosis by an expert pathology panel could reliably downstage 85% of community LGD diagnoses. In many studies that reported progression rates for LGD patients, expert histological review was not included in the work-up or was only performed in a subset of patients. The lack of a reliable LGD diagnosis in these studies is likely the most important factor associated with the high variability in reported malignant progression rates for LGD patients.
The second important cause for the wide range in reported progression risks is the high interobserver variation between pathologists for diagnosing LGD in BO, even among expert GI pathologists. Most previously reported κ values range from 0.14 to 0.32, which can be classified as poor to fair agreement.10 ,12 ,21–24 Only a minority of studies reported moderate to good agreements between GI pathologists with a special interest in BO, with κ scores ranging from 0.48 to 0.69.11 ,13 ,25 ,26 Such a wide range in κ values suggests that a reliable LGD diagnosis might be questionable, even for studies that included expert histological review of LGD. The quality and homogeneity of the expert panel seem to be essential in establishing a reliable baseline LGD diagnosis and is important in the interpretation of reported progression risks for patients with LGD.
The Dutch Barrett's Advisory Committee (BAC), founded by the Comprehensive Cancer Centre Amsterdam, is a national consultative working group that offers central pathology review for all Dutch centres.
This retrospective cohort study aimed to establish the prognostic value of the aforementioned expert pathology panel for BO related dysplasia. This was achieved by reviewing histological slides from a large cohort of BO patients with LGD and comparing this review diagnosis to the histological outcome during endoscopic follow-up.
Methods
Setting and source population
The data analysed in this study were obtained from BO patients who were referred to the BAC. The BAC is a national multidisciplinary consultative working group that harbours pathologists, gastroenterologists and surgeons with extensive experience in management of BO related dysplasia and carcinoma. Upon referral of a patient, the histology slides and endoscopic images are reviewed by expert pathologists and endoscopists, respectively. Subsequently, a multidisciplinary consensus advice on clinical management of the patient is provided.27
The histopathological specimens obtained during the initial endoscopic procedure with a diagnosis of LGD by the community hospital pathologist were retrieved and reviewed by the BAC expert pathology panel. This pathology panel consists of six pathologists (FJWtK, GAM, CAS, GJO, MV and SLM) with extensive experience in BO related dysplasia. They have assessed histological inclusion criteria for research studies into various treatments for BO patients performed at the Academic Medical Centre, Amsterdam.28–30 At least two panel pathologists were required to review all retrieved H&E stained slides of paraffin embedded biopsy specimens. The presence of intestinal metaplasia was recorded and the presence and degree of dysplasia were classified according to the Vienna classification into NDBO, IND, LGD, HGD or invasive OAC.31 Histological reviews were performed according to four different methodologies: cases where two pathologists reviewed the specimens together and reached a conclusion (method A); cases that were independently reviewed by two pathologists and where disagreement between pathologists was resolved in a dedicated consensus meeting (method B); cases with two independent expert reviews and where disagreement between both pathologists was resolved after consulting a third panel pathologist (method C); and cases with an initial independent review by three expert pathologists (method D).
The institutional ethics committee of the Academic Medical Centre, Amsterdam has exempted this study from formal ethical review. The follow-up analysis was restricted to all patients who gave written informed consent to the gathering of clinical data.
Study population
BO was defined as visible columnar epithelium on initial endoscopy, extending at least 1 cm above the gastro-oesophageal junction, with biopsy specimens showing intestinal metaplasia. All BO patients with LGD who were referred to the BAC between January 2000 and December 2011 were eligible for inclusion. We excluded patients who participated in a previous study by our group on natural history of LGD.11 Patients who were included in a randomised trial comparing radiofrequency ablation (RFA) with regular endoscopic surveillance in patients with confirmed LGD were also excluded.32
Endoscopic follow-up
Endoscopic follow-up data were analysed in order to relate the review diagnosis to the histological outcome during endoscopic follow-up. For all patients with a referral diagnosis of LGD, follow-up endoscopic procedures with biopsies were identified in the nationwide network and registry of histo- and cytopathology in the Netherlands (PALGA database). The PALGA database has nationwide coverage since 1991, archiving the reports of all pathology laboratories in the Netherlands.33 Subsequently, one investigator visited the regional referring hospitals to collect all follow-up endoscopy and pathology reports. Data on endoscopic follow-up were entered in a dedicated database and included patient demographics (age, gender, hospital of origin), endoscopic results (procedure date, oesophageal landmarks, number of biopsies taken) and histological diagnosis.
Duration of follow-up was calculated for each patient from the date of referral LGD endoscopy to the most recent endoscopic procedure with biopsies.
Study endpoints
Primary endpoint of the study was development of any malignant progression (HGD/OAC) during endoscopic follow-up. If a patient reached the endpoint of the study, the histological slides from the HGD/OAC diagnosis had to be confirmed by the BAC expert pathology panel according to the aforementioned criteria. Pathologists were blinded for their previous review results.
Secondary endpoint of the study was the interobserver agreement between the members of the expert pathology panel.
Statistical analysis
Mean and SD were used for normally distributed continuous variables. Median and IQR were used for continuous variables with a skewed distribution. Kaplan–Meier survival analysis was performed to estimate the cumulative risk of progression to HGD/OAC. Time to progression was calculated as the interval between date of referral LGD endoscopy and date of first endoscopy with biopsies demonstrating HGD/OAC. Follow-up data were censored at the time of first event or latest known follow-up. Differences in cumulative risk between different review diagnosis subgroups were compared using the log-rank statistic. All reported p values were two-tailed and p values <0.05 were considered to indicate statistical significance.
All cases with expert histological review according to method B, and the two initial readings for cases that were reviewed according to method C were included in the analysis of interobserver agreement. Interobserver agreement between the first and second ratings was assessed using Cohen's (weighted) κ.34 ,35 Strength of agreement was categorised as follows: 0.00–0.20, poor; 0.21–0.40, fair; 0.41–0.60, moderate; 0.61–0.80, good; and 0.81–1.00, very good.36
Statistical calculations were performed using the Statistical Package for the Social Sciences (SPSS 20.0, IBM Corp., Armonk, New York, USA).
Results
Patients
Between January 2000 and December 2011, a total of 492 BO patients were referred to the BAC for histological review of a diagnosis of LGD. We excluded 199 patients due to various reasons, as depicted in figure 1. Therefore, the study population consisted of 293 patients referred for a community diagnosis of LGD. Mean age at time of LGD diagnosis was 62.8 years (SD 11.9) and 76% were men. Further patient characteristics of the study population are summarised in table 1.
Patient demographics and follow-up characteristics of the study population (n=293)

Flowchart of patients in this study. LGD, low-grade dysplasia; RFA, radiofrequency ablation; HGD, high-grade dysplasia.
In 65 patients (22%), the histological review was performed according to method A. Methods B and C included 155 (53%) and 29 patients (10%), respectively. In 44 patients (15%), the histological review was performed according to method D.
Histological review of the original LGD diagnosis yielded the following revised diagnoses: LGD in 79 patients (27%), IND in 40 patients (14%) and NDBO in 174 patients (59%) (see figure 2).

Flowchart of patients with community LGD after expert histological review by the Barrett's Advisory Committee, with review diagnosis and outcome of subsequent endoscopic follow-up. NDBO, non-dysplastic Barrett's oesophagus; IND, indefinite for dysplasia; LGD, low-grade dysplasia; HGD, high-grade dysplasia; OAC, oesophageal adenocarcinoma.
No follow-up information was available in 29/293 patients (10%) for reasons shown in figure 1. In the remaining 264 patients, data on endoscopic follow-up were available and this cohort was then stratified according to the expert histological review diagnosis, resulting in three subgroups (NDBO, IND and LGD). The histological outcome of these three subgroups is depicted in figure 2.
Progression to HGD/OAC
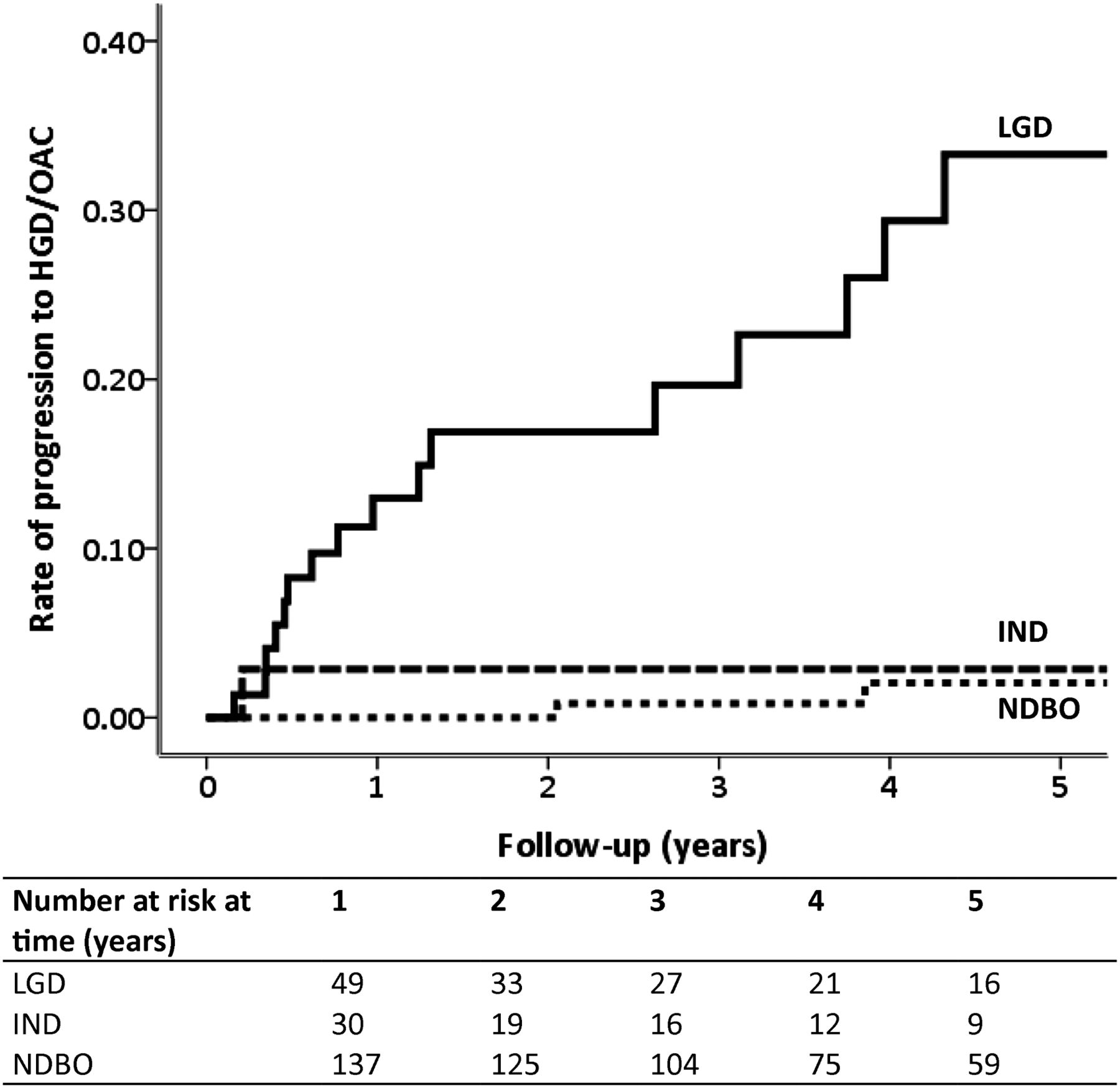
Among patients with an expert review diagnosis of LGD, 21 of 79 patients (27%) had neoplastic progression during endoscopic follow-up. Median time to progression was 16 months (IQR 5.6–68.1) and these patients underwent a median of 2 surveillance endoscopies (IQR 1–4) before progression. For patients with an expert review diagnosis of LGD, the combined incidence rate for HGD/OAC was 9.1% (95% CI 5.8 to 13.6) per patient-year. The cumulative incidence of progression for these patients was 33.3% (95% CI 18.2 to 48.4) in 5 years (figure 3).
{kind=link}
{kind=link}
{kind=link}
Kaplan–Meier plot showing the estimated cumulative risk of developing high-grade dysplasia (HGD) or oesophageal adenocarcinoma (OAC) for patients with an expert review diagnosis of low-grade dysplasia (LGD), indefinite for dysplasia (IND) and non-dysplastic Barrett's oesophagus (NDBO).
Among patients who were downstaged to NDBO or IND after expert histological review, five of 214 patients (2%) subsequently progressed to HGD/OAC. These patients had a median time to progression of 46 months (IQR 13.6–90.6). In two of five patients (40%), LGD was diagnosed and confirmed by the expert pathology panel during the interval between the downstaged referral LGD diagnosis and progression to HGD/OAC. Patients who were downstaged to NDBO or IND after expert histological review had a combined incidence rate of 0.6% (95% CI 0.2 to 1.3) and 0.9% (95% CI 0.4 to 4.3) per patient-year, respectively. The 5-year cumulative incidence of progression was significantly lower for patients with an expert review diagnosis of IND (2.9%; 95% CI 0.0 to 8.4; p=0.002) and NDBO (2.1%; 95% CI 0.0 to 5.0; p<0.001), compared with patients with confirmed LGD. Further details on the three subgroups of review diagnosis categories are shown in table 2.
Progression to HGD/OAC for the three review diagnosis categories in patients with available endoscopic follow-up
Treatment
Among patients who progressed to HGD/OAC after a confirmed diagnosis of LGD (n=21), three patients progressed to advanced stage OAC not amenable to endoscopic or surgical treatment and received palliative care. The remaining 18 patients were managed endoscopically with endoscopic resection and/or RFA. Two of these patients were still under treatment upon submission of the manuscript, all the 16 remaining patients achieved complete remission of neoplasia and 15 of 16 patients (94%) achieved complete remission of intestinal metaplasia during a median follow-up of 27 months (IQR 20–39).
Among patients who were downstaged to NDBO/IND and subsequently progressed to HGD/OAC (n=5), one patient received palliative treatment for an advanced OAC that was not amenable to surgical therapy due to severe comorbidity. One patient was referred for oesophagectomy when the endoscopic resection specimen revealed submucosal invasion (Sm1) with lymphovascular invasion. The subsequent oesophagectomy specimen demonstrated no residual cancer and no positive lymph nodes and the patient remained disease free during 12 months follow-up. The remaining three patients were managed endoscopically by endoscopic resection and/or RFA. Two of these patients were still under treatment upon submission of the manuscript; the other patient remained in complete remission for neoplasia and intestinal metaplasia during 26 months follow-up.
Agreement between pathologists
In total, 184 patients (methods B and C) were included in the analysis of interobserver agreement. In 133 patients (72%; 95% CI 65% to 79%), there was complete agreement between the two reviewing panel pathologists after the first reading. In 21 patients there was disagreement between NDBO and IND, in 13 cases there was disagreement between IND and LGD and in 16 cases the two expert pathologists disagreed between NDBO and LGD. Finally, in one case there was disagreement between LGD and HGD after the first reading. This resulted in a weighted κ of 0.49 (95% CI 0.37 to 0.61) between the first and second expert pathology review.
When the expert pathology reviews were dichotomised, counting confirmed LGD as ‘high risk’ and NDBO/IND as ‘low risk’, the proportion of complete agreement was 84% (95% CI 78% to 89%). The resulting unweighted κ value in this analysis was 0.45 (95% CI 0.27 to 0.62).
Discussion
In this community based cohort of 293 BO patients with LGD, with a median follow-up of 39 months, an expert pathology panel organised in the Dutch BAC accurately stratified patients according to their risk of malignant progression. The majority (73%) of patients were downstaged to NDBO/IND after histological review by the expert pathologists. During endoscopic follow-up, these patients demonstrated a low risk of malignant progression, with an annual progression rate of 0.6% and 0.9% for NDBO and IND, respectively. However, when the expert pathology panel confirmed the diagnosis of LGD, the risk of progression to HGD/OAC was much higher. The annual progression rate was 9.1% and the 5-year cumulative progression risk was 33.3%.
These data are in accordance with previous findings by our group in a separate cohort of community based LGD patients.11 That study included 147 patients who were diagnosed with LGD between 2000 and 2006 in six centres where we started a prospective BO registry at that time. Following expert histological review, 85% of patients were downstaged to NDBO/IND. During endoscopic follow-up, risk of progression for confirmed LGD was 13.4% per patient-year, compared with 0.5% per patient-year for patients downstaged to NDBO.11 These studies suggest that the majority of patients diagnosed with LGD in community hospitals do not have dysplasia, but reactive inflammatory changes that are misinterpreted as such. If these patients are downstaged to NDBO/IND, their risk of progression to HGD/OAC appears comparable with the combined incidence rate for patients with a primary diagnosis of NDBO/IND. In our study, five patients who were downstaged to NDBO/IND progressed to HGD/OAC, but two of these had an interval diagnosis of confirmed LGD prior to progression. When these patients were included in the LGD consensus diagnosis category, the risk of progression to HGD or OAC for patients with NDBO dropped even further to 0.3% per patient-year.
According to most international BO guidelines, all patients included in the current study would have received surveillance endoscopy every 6–12 months given their diagnosis of LGD. Data from the current study imply that the surveillance interval for 73% of these community LGD patients can be safely extended to 3–5 years (recommended for NDBO patients), which will significantly reduce surveillance cost.
A logical consequence of overdiagnosing LGD is an underestimation of the risk of malignant progression for patients with ‘true’ LGD. A recent systematic review and meta-analysis has investigated studies that reported the incidence of HGD/OAC among patients with LGD. This meta-analysis showed that BO surveillance cohorts with a high rate of LGD diagnosis report a low rate of progression to HGD/OAC, whereas a much higher rate of malignant progression is reported in cohorts where LGD is diagnosed less frequently.37 The current study also indicates that ‘purifying’ the LGD population by expert histological review identifies a subgroup with a high risk of malignant progression. Other studies that included high quality histological review by a panel of expert pathologists have reported similarly high progression rates for patients with confirmed LGD.13 ,38 On the contrary, considerably lower malignant progression rates for BO patients with LGD have been reported in a number of other, mainly US cohorts.10 ,39 ,40 However, these studies did not include expert histological review, only performed this on a subset of patients or did not include a consensus diagnosis. Furthermore, the quality and homogeneity of the expert pathology panel in these studies might be questionable since the only reported interobserver agreement between the expert pathologists was strikingly low (κ=0.14).10
The high progression rate for patients with confirmed LGD, which was established in the current study, warrants strict endoscopic follow-up to detect HGD/OAC at a curable stage. Recent international guidelines suggest that prophylactic ablation therapy with RFA may be an acceptable alternative in selected LGD cases.1 ,5 A recent cost effectiveness analysis indicated that RFA treatment for patients with LGD might be cost effective when the diagnosis is confirmed and stable.41 This analysis used a 0.19%–0.75% annual progression rate for LGD, which is, however, significantly less than the rate found in our current series.
One may argue that patients with confirmed LGD who developed HGD/OAC within 6 months might have had prevalent disease at baseline. This is reflected by the steep incline of the Kaplan–Meier curve for confirmed LGD patients during the first 6 months of follow-up. This indicates that LGD can be a marker of prevalent neoplasia elsewhere in the BO segment. After the first year of follow-up, the Kaplan–Meier curve still demonstrates a constant increase in cumulative HGD/OAC incidence, indicating the value of confirmed LGD to predict future progression. In our opinion, therefore, a confirmed histological diagnosis of LGD is both a marker for synchronous lesions as well as a marker for future neoplastic progression. In patients with confirmed LGD, adequate endoscopic inspection is imperative at baseline, with a low threshold for endoscopic resection. In the absence of visible abnormalities, patients with confirmed LGD should be considered for endoscopic ablation therapy to prevent future malignant progression.
The moderate interobserver agreement (κ=0.49) between the expert pathologists from the BAC is among the highest agreement levels reported for diagnosing LGD in BO.10–13 ,21 ,23–26 A more clinically relevant measure, however, might be the reliability of the pathology panel for stratifying community LGD patients into low and high risk groups of progression. The proportion of complete agreement between the expert pathologists for diagnosing LGD versus NDBO/IND was high (85%); however, the unweighted κ was paradoxically lower (κ=0.45). Since κ is affected by prevalence of the investigated disease, this low value of κ can be explained by the asymmetrical distribution of cases in this study (low rate of true LGD).34 ,35 Therefore, the interpretation of the κ value in this situation is ambiguous. However, our data showed a high rate of agreement between participating pathologists in discerning patients at high risk from those at low risk of progression.
A limitation of this study is the retrospective collection of endoscopic follow-up data in the majority of patients. This might have impacted on the completeness of endoscopic follow-up information. Follow-up information was not available in 10 patients, six patients did not consent to the study and four were lost to follow-up. This amounts to less than 3% of the study population. It is also improbable that the retrospective data collection has impacted on the diagnostic quality of endoscopic follow-up, since community pathologists rarely fail to recognise HGD/OAC.
In conclusion, results from this large multicentre study confirm that the Dutch BAC expert pathology panel can accurately risk stratify BO patients with a community diagnosis of LGD. The majority of patients will be downstaged after expert review and these patients should be managed as true NDBO patients, extending the surveillance interval to 3–5 years. However, when LGD is confirmed, the annual risk of developing HGD/OAC is 9.1%. In our opinion, these patients should be referred to expert centres for endoscopic work-up to exclude prevalent HGD/OAC followed by either strict endoscopic follow-up or prophylactic ablation therapy.
References
Footnotes
-
Contributors Study concept and design: LCD, KNP, WLC, RCM-H, JJGHMB. Acquisition of data: LCD, KNP, FJWtK, GAM, CAS, GJO, MV, SLM, KKK. Analysis and interpretation of data: LCD, KNP, WLC, JGPT, RCM-H, JJGHMB. Drafting of the manuscript: LCD, KNP, WLC, JGPT, RCM-H, JJGHMB. Critical revision for important intellectual content and final approval of the manuscript: All authors. Study supervision: RCM-H, JJGHMB.
-
Competing interests JJGHMB receives research support from Olympus Endoscopy, Cook Medical, Boston Scientific, GI Solutions Covidien, Erbe and Ninepoint Medical; receives financial support for training programs from GI Solutions Covidien; and receives honorarium-consultancy-speakers fee from Cook Medical, Boston Scientific and GI Solutions Covidien.
-
Ethics approval This study was exempted from formal ethical review by the ethics committee of the Academic Medical Centre, Amsterdam.
-
Provenance and peer review Not commissioned; externally peer reviewed.