Article Text

Abstract
With few exceptions, the most commonly recommended triple Helicobacter pylori regimen (proton pump inhibitor (PPI), amoxicillin and clarithromycin) now provides unacceptably low treatment success. A review of worldwide results suggests that successful eradication using a triple regimen is not consistently observed in any population. Clinicians should use ‘only use what works locally’ and ignore consensus statements and society guidelines if they are not consistent with local results. Clinical trials should be result based, with the goal of identifying regimens with >90–95% success. New treatments should be only be compared with the currently locally effective treatment (>90%) or a historical untreated control (which has been shown to reliably yield 0% eradication); trials using placebos or treatments known to be inferior are with rare exceptions unethical. If a highly effective regimen is not available locally, we recommend trying a 14 day concomitant quadruple treatment regimen containing a PPI, amoxicillin, clarithromycin and a nitroimidazole; 10 day sequential treatment (PPI plus amoxicillin for 5 days followed by a PPI, clarithromycin and a nitroimidazole for 5 days); or 14 day bismuth-containing quadruple treatments. Treatments needing further evaluation include those containing furazolidone or nitazoxanide, hybrids of sequential–concomitant therapies and amoxicillin–PPI dual therapy with PPI doses such that they maintain intragastric pH >6.
- Antibiotics
- antibiotic treatment
- amoxicillin
- clarithromycin
- eradication treatment
- Helicobacter pylori
- metronidazole
- proton pump inhibitors
- tetracycline
Statistics from Altmetric.com
- Antibiotics
- antibiotic treatment
- amoxicillin
- clarithromycin
- eradication treatment
- Helicobacter pylori
- metronidazole
- proton pump inhibitors
- tetracycline
The problem
A decade ago it seemed that Helicobacter pylori treatments would soon reliably provide the same high level of treatment success demanded of other common infections.1 Unfortunately, that goal was not achieved and successful treatment of H pylori infections remains a challenge. The effectiveness of most commonly recommended treatments has declined to unacceptably low levels, largely related to development of resistance to clarithromycin.2 3 We, the H pylori opinion leaders, must assume the ‘blame’ for the current state as we have not provided physicians with appropriate recommendations in line with the most up to date evidence regarding the performance of treatments. For example, the latest Maastricht Consensus Report's global recommendations for treating H pylori infections focus on regimens containing either clarithromycin (500 mg twice daily), a proton pump inhibitor (PPI; given with standard dosing) and amoxicillin (1000 mg twice daily), or the same regimen substituting metronidazole (400 or 500 mg twice daily) for amoxicillin.4 The American College of Gastroenterology also included these two regimens in their guidelines published soon after the Maastricht III report, despite their own admission that these first-line treatments only eradicate 70–85% of infections.5 Likewise, although the Cervia II working group explicitly noted that the efficacy of standard treatments is ‘largely decreasing’, they too included these triple regimens in their recommendations for first-line treatments.6 Regardless of the evidence showing unacceptably low treatment success, these guidelines, and others like them, have given clinicians a consistent message to use triple regimens containing clarithromycin for first-line treatment. Here we discuss the current status of H pylori treatment, and provide our opinions regarding initial treatment as well as what to do following one or more treatment failures. Our guidelines for successful treatment are shown in box 1.
Box 1 Authors' guidelines for anti-H pylori treatment
The golden rule for choice of treatment is only to use what works locally (ie, ≥90 or 95% success)
Monitor its effectiveness over time
Treatment success of ≥95% per protocol is obtainable and should be expected
The factors that influence treatment success are: drugs, doses, dosing intervals and treatment duration
Treatment failures are explainable based on one or more of the factors listed above
Proportion cured should only be assessed against expected outcome (eg, ≥95%)
Comparisons with known low treatment success regimens are unethical unless full informed consent regarding treatment outcome expected with the low success regimen and provisions are made to deal with the expected treatment failures122
The current status of clarithromycin-containing triple regimens
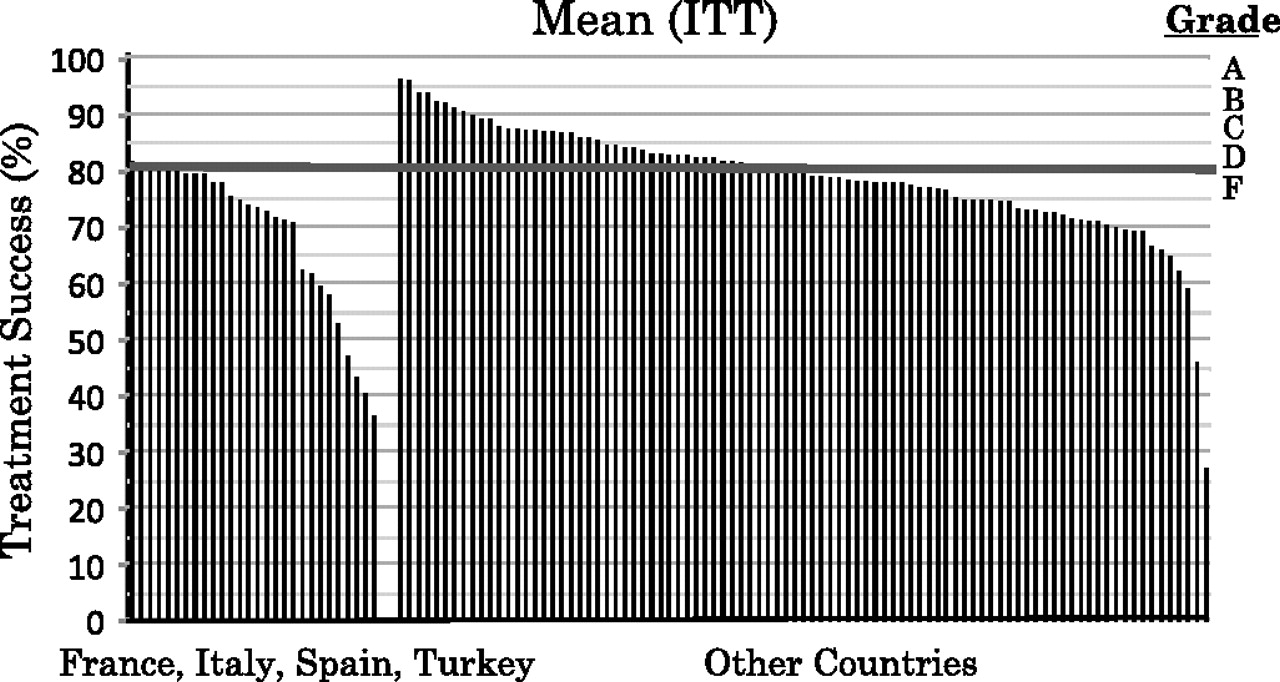
For several years now, meta-analyses have reported that the effectiveness of the triple regimens containing clarithromycin has decreased over time, corresponding with the increase in clarithromycin resistance.7 However, when we searched the recent literature regarding H pylori eradication treatments, the recommended ‘legacy triple therapy’ consisting of a PPI, clarithromycin and amoxicillin was clearly the dominant treatment used. For example, ∼60% of first-line treatment arms published in trials since the Maastricht III Consensus Report used ‘legacy triple therapy’ consisting of a PPI, clarithromycin and amoxicillin,8–45 and even in Italy where clarithromycin resistance is high, ‘legacy therapy’ has been reported to be the preferred regimen for eradication of H pylori for most (88%) general practitioners.46 Figure 1 shows treatment success (and the corresponding 95% CI) for treatment arms using the Maastricht III recommended ‘legacy triple therapy’ found in the recent literature and in existing databases from published meta-analyses and systematic reviews of first-line treatments used in adult patient populations.8–45 47–88

Percentage of intention-to-treat (ITT) treatment success for ‘legacy triple therapy’. ‘Legacy triple therapy’ contains a proton pump inhibitor (PPI), clarithromycin and amoxicillin. The studies were identified from published articles and reviews in PubMed; see text for details.
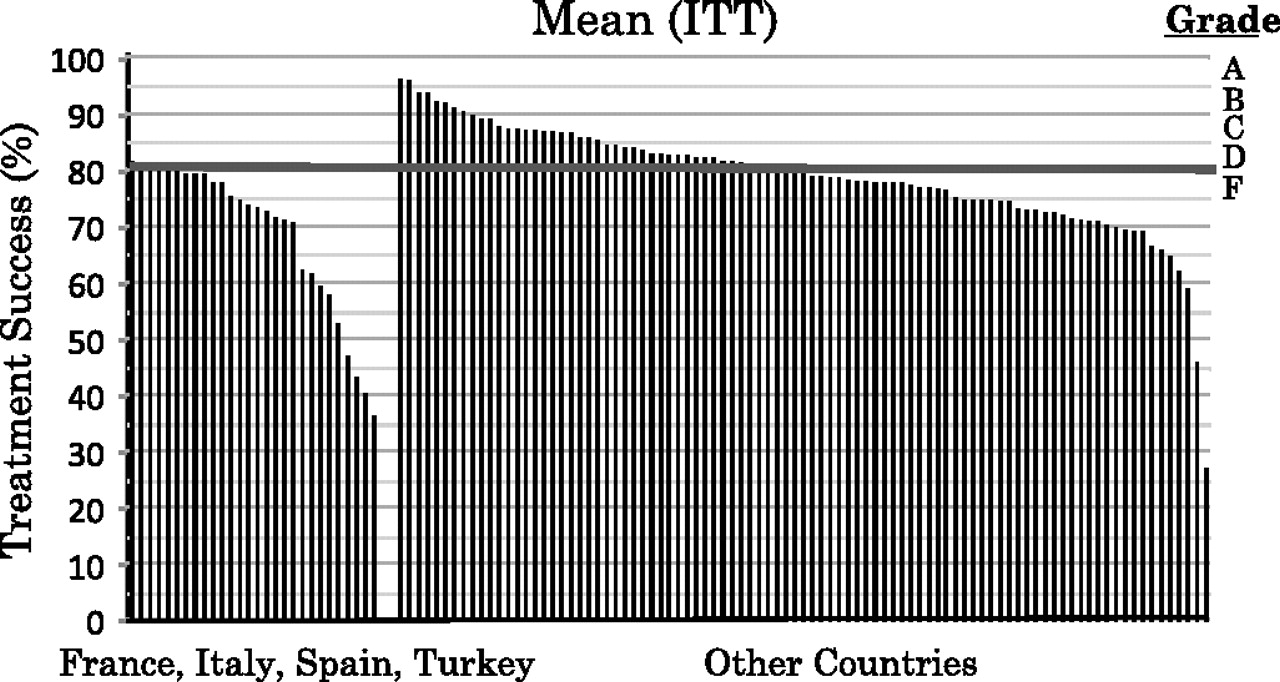
Clearly, the vast majority show unacceptably low treatment success for ‘legacy therapy’, with only 18% exceeding 85% and ∼60% failing to reach 80% eradication intention-to-treat. Highly successful treatment was not consistently observed across studies in any population. As shown in figure 2, treatment success fails to reach even 80% in most studies in the southern and central European countries of France, Italy, Spain and Turkey, populations which, as the Maastricht III report noted, tend to have a high prevalence (∼18.5%) of clarithromycin resistance (figure 2). Similar poor results were obtained in the more recent large US trials of triple regimens.68 77 89–91 Using meta-regression methods described previously,7 92 we observed treatment success for the more commonly used ‘legacy triple therapy’ to be ∼8.1% lower than treatment success for the combination using metronidazole in place of amoxicillin in recent years (95% CI 2.2% to 14.0%).
Percentage of intention-to-treat treatment success for ‘legacy triple therapy’ in populations in southern Europe and other geographic areas. Treatment success is also graded using the Report Card scoring system.91 Legacy triple therapy' contains a proton pump inhibitor (PPI), clarithromycin and amoxicillin. Southern European countries studied include France, Italy, Spain and Turkey. Studies were identified from published articles and reviews in PubMed; see text for details.
Response to falling treatment success
The increasingly low treatment success should have been a call to action resulting in widespread discussion of the problem, and rigorous studies in a variety of populations using different antimicrobial agents, doses, formulations and durations, to identify new effective treatments. Instead, the fact that the most commonly recommended treatments no longer cured even 80% of infections in many populations was not appreciated by general clinicians. The message that declining treatment success had reached the point where triple regimens containing clarithromycin should be abandoned as an empiric first-line treatment in these populations was communicated in an unintelligible ‘code’ or was completely ignored in the summary guideline statements. For example, the Maastricht III report recommended that ‘the threshold of clarithromycin resistance at which this antibiotic should not be used, or a clarithromycin susceptibility test should be performed, is 15–20%’. In retrospect, while this recommendation may have been satisfying to both the participants (disclosure, DYG was one) and the conference sponsors (most of whom were major stakeholders in triple regimens), it was meaningless to most general clinicians because of the absence of widespread information on the prevalence of drug resistance in local populations.4
In general, the message that ‘legacy triple therapy’ provides unacceptable results in many populations and alternative treatments with superior effectiveness should be evaluated for use in these populations is still not widely understood by general clinicians nor reflected in the recently published Food and Drug Administation (FDA) ‘Draft Guidance: Guidance for Industry. Helicobacter pylori-associated duodenal ulcer disease in adults: developing drugs for treatment’ (http://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/UCM184500.pdf). Some of the reasons for this misunderstanding may include: (1) ‘legacy triple therapy’ is the only approved combination in some populations; (2) most information comes directly or indirectly from pharmaceutical companies who are stakeholders in ‘legacy therapy’; (3) these same companies provide support for meetings, speakers, societies, consensus conferences and consultants (ie, why upset one's benefactors); (4) confirmation of eradication is not routinely done and thus clinicians are unaware of their own treatment failures; and (5) community surveillance of antimicrobial resistance typically does not include H pylori. The time is long overdue for us, the H pylori investigators, to speak up and communicate to clinicians that the treatments they are using are often no longer effective, recommend superior alternative treatments and seek out new highly efficacious treatments.
Why is H pylori difficult to cure?
There are many reasons that successful treatment (ie, consistent treatment success ≥90%) of H pylori infections remains a challenge. These reasons include those due to the nature of the organism itself, those pertaining to the intragastric environment where the organism resides, those relating to the regimens used to eradicate the organism, and the behaviour and reactions of the host. The roles that the organism, gastric environment, hosts and drug regimens play in treatment failures are often inter-related. Drug regimens should be designed to overcome drug-resistant and dormant forms of the organism, a high bacterial load, the typically low gastric pH, impaired mucosal immunity and the busy lifestyle of the human host.
Since their introduction >50 years ago, antibiotics have been viewed as miracle drugs. Antibiotics have also been overused (eg, to treat viral infections or to promote weight gain in animals). This overuse has resulted in steadily increasing antimicrobial resistance such that the useful lifespan of any one antimicrobial agent has generally been limited. The strongest predictor of H pylori treatment failure appears to be antimicrobial resistance.7 92
For some antimicrobial drugs, resistance can be prevented, and at least partially overcome, by increasing the dose, duration or number of antimicrobials in the regimen. Treatment failure following use of antibiotics to which the organism is not susceptible is easily understood. In H pylori infections, resistance usually develops because of the outgrowth of a small existing population of resistant organisms.93 The total number of H pylori in the stomach is very high, resulting in an inoculum effect.93 For example, if the spontaneous mutation rate for a particular resistance was 1 in 10 million and there were 50 million organisms present, it would be statistically likely that a small population of resistant organisms would always be present. However, rare events would be unlikely in the same organism such that dual resistance would be unlikely. If a single drug were used, the minor resistant population could survive and would repopulate the stomach. Approaches to overcoming this problem include increasing the dose and duration of some drugs, using multiple drugs (one of which will probably kill the resistant organisms) or pretreatment with agents to markedly reduce the bacterial load (eg, PPIs or bismuth) which would make survival of the minor populations less likely. We have observed that using a combination of both metronidazole and clarithromycinin quadruple regimens is very effective at eradicating strains of H pylori resistant to either clarithromycin or metronidazole.94 In fact, only a negligible reduction in efficacy was observed when concomitant quadruple regimens containing a PPI, amoxicillin, clarithromycin and metronidazole (a nitroimidazole), were given to patients with either nitromidazole- or clarithromycin-resistant H pylori.
Metronidazole is a prodrug that is activated by H pylori enzymes to become active within the cell. There are a number of different enzyme pathways that can accomplish this task, and clinically one finds that by increasing the dose and duration it is possible to, at least partially, overcome metronidazole resistance.95–100
Resistance to bismuth does not occur, and it is probably the most underutilised agent.101 Amoxicillin and tetracycline resistance are usually rare in most regions.3 102 Treatment success for triple drug regimens containing amoxicillin does not always appear to be significantly lowered in the presence of amoxicillin resistance, suggesting that resistance may often be overestimated,48 especially in areas where a relatively high prevalence (ie, >20%) is reported and where appropriate tests for resistance are not utilised.103 Resistance to clarithromycin, on the other hand, has increased over time2 3 104 and is a major factor in the reduced effectiveness of triple regimens containing clarithromycin.7 Clarithromycin must bind to ribosomes in order to kill H pylori. Resistance is associated with failure to bind to ribosomes, such that resistance cannot be overcome by increasing the dose or duration.102 105 The highest frequency of clarithromycin resistance in adults is observed in southern European countries such as Italy, Spain, Portugal and France, as well as Mexico, Japan and Iran.2 3 104 Clarithromycin resistance is also fairly common in the USA, while it appears to be infrequent in Northern Europe and Hong Kong. In accordance with this (using multilevel meta-regression modelling), we observed an effect of geographic location, but not clarithromycin dose or duration, on treatment success for the commonly used ‘legacy therapy’7–45 47–88 (figure 2). Likewise, resistance to fluoroquinolones (eg, levofloxacin, moxifloxacin) is not responsive to changes in dose or duration, and has been rapidly increasing worldwide such that in most regions fluoroquinolones would be a poor choice for an empiric treatment.106
H pylori treatment failures may also occur independently of resistance—that is, treatment may fail but the organism remains susceptible to the antibiotic. This is most commonly seen with amoxicillin where failure is rarely caused by acquired resistance. This form of reversible resistance is termed phenotypical antibiotic resistance and it often due to the presence of a persistor or non-replicating population of organisms.107–109 Bacteria in the persistor population oscillate between a non-replicating and replicating state or from intracellular to extracellular environments. Thus they oscillate between a phenotypically resistant and a phenotypically susceptible state during which they can be eradicated. One solution is to extend the duration of treatment such that the antibiotic will be present during at least one period of susceptibility.110 An alternative approach is to entice the organism to enter the replicative state and become susceptible to the antibiotic.111 112 The fact that treatment success reliably increases as the duration of treatment increases from 3 to 14 days with amoxicillin and a PPI is probably an example of phenotypic resistance.113
The gastric environment also influences H pylori treatment success. H pylori typically resides within the human stomach, and populations of organisms occupy different environments, each with its own challenges. The majority of organisms are found within the mucus layer, which is technically outside of the body. Many are found attached to surface cells and a few are found even within epithelial cells.114–116 Most importantly, at any one time, a proportion of the organisms is either not replicating or is replicating very slowly, which represents a challenge for antibiotics that require microbial replication to kill the organisms (eg, clarithromycin and amoxicillin).
H pylori infections are thought to enter a non-replicative but viable state (ie, become phenotypically resistant) when the pH in their microenvironment is lower than 6 and higher than 3117 (figure 3). The site at which this occurs is most probably in the mucus layer. This localisation is based on both the direct measurement of H pylori gene expression118 and indirectly by the marked increase in effectiveness of antimicrobial treatment that occurs when pronase is used to remove this layer.119 Increasing the pH in this layer to 6 or 7 allows the bacteria to enter the replicative state where they become susceptible to amoxicillin and clarithromycin. This approach has also been the theoretical basis for the revival of PPI plus amoxicillin dual treatment.120 Using meta-regression modelling of 127 arms of dual treatment with a PPI plus amoxicillin, we observed treatment success to be ∼27% higher when the PPI was given four times per day rather than just twice a day. The theoretical reasons to explain this increase are discussed above in ‘Why is H pylori difficult to cure’, and elsewhere.112 We also observed that treatment success was ∼5% higher when the PPI was given at twice the standard dose (the standard doses for omeprazole and lansoprazole are 20 and 30 mg, respectively).

Helcobacter pylori survives over the pH range 4–8 but is incapable of growing. In contrast, active replication primarily takes place at pH 6 and 7 and, as the organism is only susceptible to killing by antibiotics such as clarithromycin or amoxicillin during growth, it can remain phenotypically resistant and thus survive antibiotic therapy. (Adapted from Scott et al.117)
Finding regimens to treat H pylori successfully
Successful treatment of an infectious disease depends on the use of the optimum regimen(s) in terms of drugs, drug formulation, dose, dosing interval and duration. Few of these parameters have been evaluated prospectively for H pylori infections, and such studies are needed to allow truly informed recommendations. The fact that the organism occupies different microenvironments makes the search for the optimal drug formulations, doses, dosing intervals or adjuvants (ie, antisecretory drugs, mucolytics) at least in part an empiric one.
The goal of testing new treatment regimens is to efficiently, safely and ethically identify those worthy of large clinical trials.121 To prevent retesting a regimen because the treatment duration or drug doses were possibly insufficient, initial choices should not be arbitrary (ie, within the usual ranges, higher doses and longer durations often provide higher efficacy such that we believe that initial evaluations of new regimens should employ the highest practical doses for the longest reasonable duration such as 14 days). Clearly, the dosing scheme and duration chosen are limited by concerns regarding safety and the patients' tolerance, as well as maintaining a high level of compliance. Initial trials evaluating a new treatment for H pylori should enrol the minimum number of subjects required to observe efficacy and use clear stopping rules that include both efficacy and safety. Subsequent larger studies designed to confirm the original observations and to evaluate different parameters such as dose, dosing interval, formulation and duration while still maintaining acceptable efficacy and tolerance should be done in geographically, ethnically and socio-economically diverse populations. The primary outcome should be treatment success, and comparison trials with currently used treatments are generally not indicated. Trials with known inferior treatments or placebos are generally unethical and not needed since we can use a historical untreated control which is known to estimate 0% eradication.7 121–123 Ideally, clinical trials should perform pretest susceptibility testing. If culture and susceptibility testing is not available, a tissue specimen can be frozen (eg, at –80°C) in H pylori transport medium for later or off-site testing. At a minimum, a specimen such as the tissue used for rapid urease testing should be frozen so that molecular testing can be done at least for the antibiotics where molecular tests are available.102 124 In general, sites without the ability to perform susceptibility testing should not be involved in studies of new treatments but can certainly test regimens already known to be efficacious elsewhere for use as a local empiric regimen.
Recommendations for judging the results of a treatment
The standard, in terms of treatment success for common infectious diseases, such as pneumococcal pneumonia, Escherichia coli urinary tract infections and gonorrhoea, is to demand treatment success (from per-protocol analyses) of >95%. When resistance increases and undermines a treatment, an alternative and superior treatment should be identified in order to maintain high treatment success. H pylori treatment should be no different and we should no longer recommend and treat patients using a regimen that has repeatedly been shown to be ineffective.
We recommend that H pylori treatment evaluation should also be ‘results based’ and we previously proposed a ‘report card’ format to judge effectiveness using the scale of A=95–100%, B=90–94%, C=86–89% and F=≤85% from per-protocol analyses.91 We recommend that only grade A, or at most grade A and B treatments, be used. When neither a grade A nor a grade B treatment is available in a population, we recommend using the most effective treatments available locally which have been shown to be safe, and that new regimens, or those which have been shown to be highly effective in other populations, be tested until at least a grade A or B treatment is identified.
General guidelines for treating patients diagnosed with H pylori infections
Clinicians should use the rule ‘only use what works locally’ and should ignore consensus statements and society guidelines if the results are not consistent with local treatment results. Ideally, clinicians should be kept aware of the prevalence of antimicrobial resistance locally or regionally, as well as the efficacy of treatments in their practice. Currently pretreatment antimicrobial testing is not readily available, is expensive and often requires endoscopy to obtain the specimen for culture. The ability to obtain local susceptibility patterns is likely to improve based on the increasing availability of molecular methods (ie, PCR or fluorescent in situ hybridisation (FISH)) which can be used to evaluate clarithromycin and fluoroquinolone susceptibility directly from biopsies.102 124 125 More importantly, antimicrobial susceptibility testing using stools and biopsy specimens has proven practical for evaluation of clarithromycin resistance. The use of stools obviates the need and expense of endoscopy and theoretically makes obtaining local-, regional- or patient-specific susceptibility testing for some antibiotics practical. This approach has been used clinically, allowing ‘tailored treatment’ with marked improvements in treatment success.17 124 126 Lacking susceptibility data, clinicians can use prescribing practices and prior treatment history to estimate the likelihood of antimicrobial resistance. A high level of local use or individual patient's previous use of clarithromycin for any reason are useful proxy indicators of local antimicrobial resistance prevalence.127
Because H pylori is typically acquired in childhood, most patients have been infected for many decades and clinicians should feel no sense of urgency regarding initiating treatment. Physicians should take whatever time is needed to gather the information needed for a successful result. Lacking current local susceptibility data, we recommend that when either the patient has used clarithromycin previously or treatment success for clarithromycin-based treatments is low, clinicians treat every patient as if clarithromycin resistance were present.
General recommendations for treatment
Besides of considerations regarding allergies and the local availability of the drugs, we recommend that clinicians use the following general rules when treating patients with a H pylori infection: (1) do not use ‘legacy triple therapy’ consisting of a PPI, clarithromycin and amoxicillin unless it has been proven to be highly effective locally (eg, eradication ≥90% in per-protocol analyses); (2) use higher doses of drugs (eg, 500 mg of clarithromycin, metronidazole and tetracycline) unless it has been shown that lower doses are equally effective; (3) use 14 day duration unless a shorter duration has been shown locally to be equally effective (eg, for clarithromycin and fluoroquinolones); (4) do not use a triple regimen containing clarithromycin, if clarithromycin is commonly prescribed locally or the patient has taken clarithromycin in the past, for any indication; (5) avoid fluoroquinolones if a quinolone (eg, ciprofloxacin, levofloxacin or moxifloxacin) has been given previously, even for any indication; and (6) following treatment failure, do not reuse drugs for which resistance is likely to have developed (ie, clarithromycin and fluoroquinolones).
The current most effective first-line empiric treatments for adult patients
One would hope that one could turn to meta-analyses to determine the optimum treatment(s) for H pylori in different populations. However, this has rarely been the case. With adequate data from previous studies, meta-analyses can provide information that clinicians need to know such as what works, where does it work, when (under which conditions) does it work and why, or why it does not work (ie, to be clinically useful one should be able to answer where, what, when and why). Whenever possible, treatment should be based on knowledge of the antimicrobial susceptibility for that patient (ie, tailored treatment). When that is not possible or practical, one must use an empiric regimen. Using appropriate methods from meta-analyses, we recommend using a four-drug treatment (ie, either sequential, concomitant or bismuth-containing). Concomitant treatment as currently used is a quadruple regimen containing a PPI, amoxicillin, clarithromycin and a nitroimidazole (metronidazole or tinidazole); sequential treatment consists of a 10 day treatment in which a PPI plus amoxicillin is given for 5 days followed by a PPI plus clarithromycin and a nitroimidazole (metronidazole or tinidazole) for 5 days. Concomitant treatment consistently achieves grade A or B levels of effectiveness and has been evaluated in a variety of populations including Japan, Taiwan, Colombia and several countries throughout Europe (figure 4).9 73–76 128–132 Likewise, the recommended sequential treatment provides a high level of effectiveness in Italy, Korea, Taiwan and the USA14 42 44 52 63 65 70 132–138 (figure 5) (Ping-I Hsu, Kaohsiung Hp Treatment Group, unpublished data) and recently in Japan as a second-line treatment for those who had failed ‘legacy triple therapy’.139 However, in Korea, sequential treatment achieved success of only 86% (95% CI 75% to 93%), which may have been related to higher rates of dual resistance locally.13 Both concomitant and sequential treatment are designed to overcome increasing clarithromycin resistance. Neither is ideal, as treatment success is generally <95% and both can be improved.140 The success rate for both is dependent on the rates of resistance to clarithromycin and to metronidazole and thus neither is exempt from the rule to know what works locally. The recommended doses and drug combinations are shown in table 1.

Per-protocol (PP) treatment success and 95% CIs for concomitant quadruple treatment. The data are shown left to right in order of year of publication.9 73–76 128–132 The grey bars represent studies published in 2009 and 2010. Treatment success is also graded using the Report Card scoring system.91 Studies were identified from published articles and reviews in PubMed; see text for details.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Per-protocol (PP) treatment success and 95% CIs for sequential quadruple treatment.The data are shown left to right in order of the year of publication.14 42 44 52 63 65 70 132–138 Treatment success is also graded using the Report Card scoring system.91 Studies were identified from published articles and reviews in PubMed; see text for details.
Recommended treatments with the currently highest success
One must remember that even in area where clarithromycin resistance is high, most patients will have clarithromycin-susceptible strains, such that clarithromycin can effectively be used as one component of an empiric quadruple regimen containing two other antibiotics (ie, as either sequential or concomitant treatment). In a recent study comparing sequential and concomitant treatments, dual resistance to clarithromycin and metronidazole significantly reduced efficacy for the sequential, but not the concomitant treatment.132 Concomitant treatment is also less complicated than sequential treatment (ie, one simply adds two 500 mg metronidazole tablets to ‘legacy twice-a-day triple therapy’). In an attempt to improve treatment success further to grade A, we recommend prescribing concomitant treatment for 14 days instead of for shorter durations. Theoretically, sequential treatment could be improved by increasing the doses, duration or the number of drugs in each phase (eg, by continuing amoxicillin into the second part of the sequential threatment).140 We have recently examined a sequential–concomitant hybrid treatment with 7 days of dual PPI plus amoxicillin, followed by amoxicillin, clarithromycin, metronidazole and PPI for an additional 7 days. Treatment success with this new sequential treatment was >95%, making it a clear grade A regimen, whereas increasing the duration of sequential treatment to 14 days (7+7) did not increase success (Ping-I Hsu, Kaohsiung Hp Treatment Group, unpublished data). We are currently comparing different durations of the dual component of the new hybrid treatment to identify the shortest duration that will maintain >95% treatment success.
A bismuth triple regimen consisting of a bismuth salt, metronidazole/tinidazole and tetracycline was the first successful H pylori treatment; initially it provided treatment success >95% even without the use of an antisecretory drug.141 Subsequent experience showed that eradication was reduced in the presence of metronidazole-resistant H pylori and that this could be largely overcome by increasing the dose of metronidazole and duration and/or adding a PPI.95 142 143 As such, the dose of metronidazole (eg, ∼1500 mg per day) and duration (14 days) are considered optimum especially in areas where metronidazole resistance is more than trivial.95 112 143 In many populations, quadruple regimens containing a bismuth compound, metronidazole (500 mg three times a day), tetracycline (500 mg four times a day) and a PPI (standard dosing twice daily) can achieve grade A and B level effectiveness.92 144 Importantly, the commercially available convenience pack containing bismuth, metronidazole and tetracycline in the USA (Helidac) contains what may be a suboptimal doses of metronidazole (250 mg four times a day). The other available convenience pack, Pylera, contains what may be a suboptimal dose of tetracycline (375 mg three times a day instead of the recommended 500 mg four times a day) and comes in a package for 10 day treatment, making it difficult to provide it for 14 days. Therefore, it is a less attractive choice unless the prevalence of metronidazole resistance is low, pretreatment antimicrobial testing is available or it has proven to provide grade A treatment success locally. If one chooses to use these convenience packs, it may be prudent to add an additional prescription to bring the dose up to 500 mg three times a day for both. Head-to-head comparisons of the commercial products with what is considered optimal are lacking. Bismuth is not available worldwide and thus its use is restricted to those countries where it is available.
Options after treatment failure
When confronted with a patient who has failed treatment, an appropriate second-line treatment should be chosen. With multiple treatment failures this becomes difficult as one is choosing a ‘rescue’ treatment. The issues include: (1) What antibiotics is the infection likely to be resistant to? (2) Which drugs can the patient not take either because of an allergy or side effects? and (3) Which drugs are available locally? The best method to determine which drugs the infection is resistant to is to test for antimicrobial susceptibility (tailored treatment). As noted above, this can be done using stool specimens for clarithromycin and fluoroquinolone susceptibility which can be assessed using molecular techniques, but this is not available for the other commonly used drugs. As a general rule, as noted above, when antimicrobial susceptibility testing is not feasible, one can presume that the infection is resistant to antibiotics that the patient has taken previously in which resistance is common or develops rapidly (eg, metronidazole, clarithromycin or fluoroquinolones). Thus, we recommend including at least one antibiotic the patient has not previously taken. Sequential and concomitant treatments expose the patient to both clarithromycin and metronidazole/tinidazole, and therefore we do not recommend that both drugs be used in the rescue treatment as well (see table 2). One recent approach has been to use a fluoroquinolone-containing triple or quadruple regimen. However, the worldwide rapid increase in fluoroquinolone resistance has undermined this approach in many areas and one must fall back on the ‘only use what works locally’ rule.145–147 In addition, one should generally expect the same treatment success rate for first, second and even third treatment regimens if the organisms are susceptible.
Regimens that have been used in the past but are generally not recommended as empiric treatment and treatments used as rescue treatment after failure of drug combinations in table 1
It is important to remember that metronidazole resistance can often be partially overcome by increasing the dose and duration; the option of a 14 day bismuth-containing quadruple regimen (bismuth, metronidazole, tetracycline and a PPI) remains, and this is often the preferred approach, albeit ensuring that the regimen uses the appropriate doses and duration of treatment (eg, 1500 or 1600 mg of metronidazole and 2 g of tetracycline for 14 days). Thus, if one initially used a clarithromycin-containing concomitant or sequential regimen, one of the reasonable second choices would be 14 day bismuth quadruple regimen. If this bismuth quadruple rescue treatment is ineffective in the local population, or when metronidazole is not a viable drug option, metronidazole can be replaced by furazolidone (100 mg). Quadruple rescue treatment, containing bismuth and furazolidone, is our pièce de résistance and we have had essentially no failures in the USA even after multiple prior treatment failures (unpublished observation).
An alternate rescue treatment approach is to use a PPI plus amoxicillin-based triple regimen. Twice-a-day PPI plus amoxicillin for 14 days will typically achieve ∼50% treatment success (lower treatment success is achieved with shorter durations). As previously mentioned, PPI plus amoxicillin dual treatement can be improved by increasing the frequency and dose of the PPI and extending treatment duration. Until this dual treatment is shown consistently to provide grade A or B effectiveness with higher doses and longer durations, we recommend adding a third drug (not previously used by the patient) to a 14 day PPI plus amoxicillin regimen. A fluoroquinolone (once a day) is a good choice for the third drug, provided that resistance is not present. The other option that is commonly used is rifabutin (150 mg twice a day).
Some cautions associated with anti-H pylori antimicrobials
Metronidazole, tinidatzole and furazolidone have received cautions regarding carcinogenicity. Nitroimidazoles may cause an antibuse-like reaction when taken with alcohol. Furazolidone is a monamine oxidase inhibitor and thus patients prescribed this medication should be advised to avoid the intake of all cheeses (except cottage and cream cheeses), bologna, salami and pepperoni, lima beans, lentils, snow peas and soybeans, canned figs and raisins, beer, ale and wines (especially Chianti wine), liquorice, soy sauce and any food product that is made with soy sauce. Fluoroquinolones are associated with an increased risk of tendinitis and tendon rupture. This risk is further increased in those over age 60, in kidney, heart and lung transplant recipients, and with use of concomitant steroid treatment. Rifabutin induces CYP3A enzymes and has a very long list of drugs with which it interacts listed in three categories: avoid/use alternative; monitor/modify treatment; and caution advised. It is also an important antimycobacterial agent and there is some fear that overuse will be associated with increasing resistance in mycobacteria. It should probably be considered a drug of last resort. Finally, some drugs are not widely available (eg, bismuth and furazolidone).
Conclusions
Increases in antimicrobial resistance have led to decreases in H pylori treatment success, such that the most commonly prescribed regimens used to treat H pylori infection (clarithromycin-containing triple regimens) are no longer adequately effective in most populations. Alternative treatments with superior effectiveness should be sought and appropriately tested in a variety of populations. Instead of following consensus guidelines which recommend using clarithromycin triple regimens such as ‘legacy therapy’ (clarithromycin–amoxicillin–PPI), clinicians should prescribe treatments which achieve ≥90% eradication in their local population. If a highly effective regimen has not yet been found in the local population, we recommend using treatments which are currently consistently effective in a variety of adult populations such as: (1) a 14 day concomitant quadruple regimen containing a PPI, amoxicillin, clarithromycin and a nitroimidazole; or (2) a 10 day sequential treatment in which a PPI plus amoxicillin are given for 5 days followed by a PPI, clarithromycin and a nitroimidazole given for 5 days. Bismuth-based quadruple regimens, although commonly used as rescue treatments, can also be used as a first-line option to eradicate H pylori. Treatments that need further evaluation include relatively untested drugs such as furazolidone- or nitazoxanide-containing regimens, amoxicillin–PPI dual treatment with the PPI given at doses that can reliably maintain the intragastric pH above 6, and hybrids of sequential–concomitant treatments. Finally, the time is long overdue to let clinicians know that the currently used treatments for H pylori are not adequately effective, and alternative therapies with ≥95% treatment success need to be identified.
Acknowledgments
This material is based upon work supported in part by the Office of Research and Development Medical Research Service Department of Veterans Affairs. DYG is supported in part by Public Health Service grants DK56338 which funds the Texas Medical Center Digestive Diseases Center and R01 CA116845. The contents are solely the responsibility of the authors and do not necessarily represent the official views of the VA or NIH.
References
Footnotes
Funding Public Health Service grant DK56338.
Competing interests In the last 2 years, Dr Graham has received 20 free urea breath tests from Meretek. Dr Graham is a consultant for Novartis in relation to vaccine development for treatment or prevention of H. pylori infection. Dr Graham is also a paid consultant for Otsuka Pharmaceuticals and until July 2007 was a member of the Board of Directors of Meretek, Diagnostics, the manufacturer of the 13C-urea breath test. Until November 2009, Dr Graham received royalties on the Baylor College of Medicine patent covering materials related to 13C-urea breath test. Dr Fischbach declares no competing interests.
Provenance and peer review Commissioned; externally peer reviewed.