Article Text

Abstract
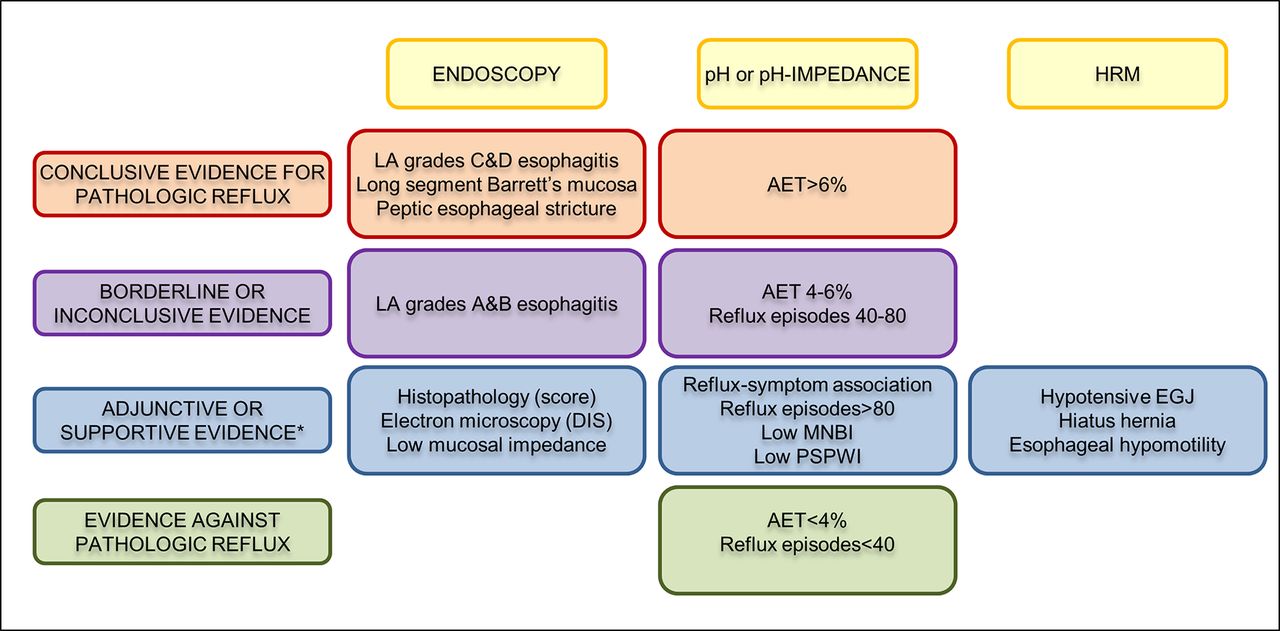
Clinical history, questionnaire data and response to antisecretory therapy are insufficient to make a conclusive diagnosis of GERD in isolation, but are of value in determining need for further investigation. Conclusive evidence for reflux on oesophageal testing include advanced grade erosive oesophagitis (LA grades C and D), long-segment Barrett’s mucosa or peptic strictures on endoscopy or distal oesophageal acid exposure time (AET) >6% on ambulatory pH or pH-impedance monitoring. A normal endoscopy does not exclude GERD, but provides supportive evidence refuting GERD in conjunction with distal AET <4% and <40 reflux episodes on pH-impedance monitoring off proton pump inhibitors. Reflux-symptom association on ambulatory reflux monitoring provides supportive evidence for reflux triggered symptoms, and may predict a better treatment outcome when present. When endoscopy and pH or pH-impedance monitoring are inconclusive, adjunctive evidence from biopsy findings (histopathology scores, dilated intercellular spaces), motor evaluation (hypotensive lower oesophageal sphincter, hiatus hernia and oesophageal body hypomotility on high-resolution manometry) and novel impedance metrics (baseline impedance, postreflux swallow-induced peristaltic wave index) can add confidence for a GERD diagnosis; however, diagnosis cannot be based on these findings alone. An assessment of anatomy, motor function, reflux burden and symptomatic phenotype will therefore help direct management. Future GERD management strategies should focus on defining individual patient phenotypes based on the level of refluxate exposure, mechanism of reflux, efficacy of clearance, underlying anatomy of the oesophagogastric junction and psychometrics defining symptomatic presentations.
- gastroesophageal reflux disease
- PH monitoring
- manometry
- endoscopy
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
GERD has an estimated worldwide prevalence of 8%–33%, involves all age groups and both genders1 and carries a price tag estimated at >US$9–US$10 billion/year in the USA alone, largely related to proton pump inhibitors (PPI) use and diagnostic testing.2 The current paradigm of GERD diagnosis hinges on the identification of oesophageal mucosal lesions or troublesome symptoms caused by gastro-oesophageal reflux.3 A putative GERD diagnosis is bolstered by a favourable response to PPI therapy.4 The primary determinant of mucosal injury is excessive oesophageal acid exposure attributable to anatomical or physiological defects of the oesophagogastric junction (EGJ) and oesophageal peristalsis.5 GERD symptoms, however, have multiple potential determinants including the number of reflux episodes, the proximal extent to which the refluxate migrates, the acidity of the refluxate, oesophageal hypersensitivity and cognitive hypervigilance. Consequently, depending on the clinical context, the defining features of GERD can be pathology, physiology or symptomatology. In this paradigm, oesophageal testing is often undertaken to define optimal management, be that PPI therapy, antireflux surgery (ARS) or cognitive behavioural therapy.
The aim of the GERD consensus process was to determine modern indications for oesophageal testing in GERD, and as an extension to that aim, to define criteria for a clinical diagnosis of GERD. The consensus process started in 2014, when the primary aims were formulated, followed by a literature search and grading of evidence. There was extensive discourse within a multinational group of GERD experts over 2 years, following which consensus statements were developed and published.6–8 These consensus statements were adapted for the practising gastroenterologist by a cohort of international experts at the Lyon GERD consensus meeting in November 2017, the conclusions from which are presented in this manuscript.
Diagnosis of GERD
GERD is empirically diagnosed and treated in clinical practice based on the clinician’s symptom assessment. Indications for testing include treatment failure, diagnostic uncertainty and treating (or preventing) complications of GERD. However, diagnostic testing may or may not support the initial diagnosis, as the criteria defining GERD are specific to each testing modality. Consequently, understanding the performance characteristics of each diagnostic modality and recognising evidence that supports or refutes the clinical impression of GERD is crucial. The Lyon Consensus evaluated GERD diagnostic tests from that perspective, and test results were categorised as being adequate to establish or refute a GERD diagnosis or inconclusive in the absence of additional supportive evidence.
The primary focus of oesophageal testing has hitherto been restricted to detection of excessive acid reflux as indicative of pathological GERD, supported by reflux-symptom association analysis. The threshold value discriminating abnormal from normal oesophageal acid exposure with 24 hour pH-metry was initially selected based on evidence that higher acid exposure is associated with the presence of reflux oesophagitis.9 However, the focus of current GERD management is on healing mucosal disease and on managing symptoms. The association of oesophageal acid exposure with patient symptoms is weak,10 11 making sole reliance of this metric problematic. Expansion of testing to include oesophageal mucosal impedance, manometry, histopathology and psychometrics may help in this regard, potentially identifying distinct GERD phenotypes with unique management implications. Each test adds a piece to the overall puzzle of symptom generation, disease pathophysiology and precision management.
Clinical history and questionnaires
Typical GERD symptoms (heartburn and acid regurgitation) are more likely than atypical symptoms to respond to treatment, emphasising the value of an accurate clinical history.5 However, when compared with objective evidence of GERD defined by pH-metry or endoscopy, even an expert history by a gastroenterologist has only 70% sensitivity and 67% specificity,12 reiterating the distinction between a physiology-based and a symptom-based GERD diagnosis. Likewise, questionnaires such as the reflux disease questionnaire (RDQ) and gastroesophageal reflux disease questionnaire (GERDQ) have similar limitations when compared with physiological testing.12–14 However, in clinical practice, diagnosing and treating GERD based on typical symptoms is pragmatic and endorsed by societal guidelines,4 even though these symptoms are neither sensitive nor specific for objectively defined GERD.12
Proton pump inhibitor trial
Although pragmatic, symptomatic response to PPI therapy does not equate to a GERD diagnosis, exhibiting an imperfect correspondence with objectively defined disease. On average, 69% of patients with oesophagitis, 49% of patients with non-erosive reflux disease (NERD) and 35% of patients with normal endoscopy and pH-metry gain symptom relief from a PPI trial.15 Hence, when evaluated as a diagnostic test for GERD among patients with heartburn, an empiric PPI trial has a sensitivity of 71% and specificity of only 44% compared with the combination of endoscopy and pH-metry.12 16 With atypical symptoms (chest pain, chronic cough, laryngitis, etc), PPI response rates are much lower than with heartburn, thereby diminishing the utility of that approach to diagnosis.17 A major limitation of the ‘PPI test’ is the strong modulation of symptoms by oesophageal hypersensitivity18 19; there is also variation in PPI dosing and duration of the test.20 Nonetheless, despite low specificity and high placebo response,21 the empiric PPI treatment approach is less costly than diagnostic testing22 and is endorsed by societal guidelines4 undoubtedly leading to the overdiagnosis of GERD and overuse of PPIs.
Endoscopy and biopsy
When putative GERD symptoms do not respond to empiric PPI therapy, upper endoscopy (EGD) is advised both to evaluate for GERD complications and to detect potential alternative diagnoses that might redirect therapy. High-grade oesophagitis (LA grades C or D), Barrett’s oesophagus or peptic stricturing are considered confirmatory evidence for GERD.6 However, erosive oesophagitis is found in only 30% of treatment-naïve patients with heartburn and in <10% when already taking a PPI.23 24 Furthermore, most of that is low-grade, and lower grades of oesophagitis, particularly LA grade A, are non-specific, found in 5%–7.5% of asymptomatic controls.25–27 When accurately defined, LA grade B oesophagitis provides adequate evidence for initiation of medical management of GERD, but problems with interobserver variability led an expert panel to conclude that additional pH-metry evidence is requisite prior to pursuing ARS.28 Barrett’s oesophagus is observed in 5%–15% of patients with chronic GERD,29–31 but histological confirmation is documented in only 50% of these. In summary, EGD findings can be clinically important and specific for GERD, but EGD has a low sensitivity in GERD diagnosis.
The Rome IV consensus recommended oesophageal biopsies during EGD to rule out eosinophilic oesophagitis.32 Biopsies may also have value in differentiating NERD (with positive pH-metry) from reflux hypersensitivity, functional heartburn and controls when scored using a structured histopathological protocol evaluating papillary elongation, basal cell hyperplasia, dilated intercellular spaces, intraepithelial inflammatory cells, necrosis and erosions33 34; changes that resolve following adequate GERD therapy.35 However, histopathological findings can overlap between the groups studied, and are not conclusive of GERD. Identification of dilated intercellular spaces on electron microscopy suggests mucosal injury from reflux,36 37 but clinical application is limited. The widespread adoption of histopathological examination for GERD injury is hindered by the cumbersome protocol and need for a dedicated oesophageal pathologist.33 38 39
Ambulatory reflux monitoring
Ambulatory reflux monitoring can provide confirmatory evidence of GERD, in patients with normal endoscopy, atypical symptoms and/or when contemplating ARS.6 Reflux monitoring demonstrates the consequence of GERD pathophysiology, evident as either excessive oesophageal acid exposure time (AET) or reflux episodes, rather than the mechanism by which that occurs. Reflux-symptom association uses simple ratios and statistical tests to determine whether reflux episodes co-occur with symptoms, and adds value to ambulatory reflux monitoring. Hence, reflux monitoring can confirm or exclude pathological GERD, although not always conclusively.
The primary outcome of a 24-hour pH-metry study is the AET. Extending recording time to 48 or 96 hours with the wireless pH monitoring system increases the diagnostic yield40–42 and test reproducibility,43 and is particularly useful when a transnasal catheter was not tolerated or yielded a negative result despite high suspicion of GERD.40 44 However, wireless pH monitoring is expensive, limiting its availability. Another variation on reflux monitoring is pH-impedance monitoring, which characterises reflux events with both a pH electrode and a series of impedance electrodes. Since pH-impedance detects all reflux (liquid, gas or mixed) regardless of acidity, and defines the direction of flow, it is considered the gold standard.6 45 However, the added yield is limited,46 47 the test is not widely available and the interpretation is laborious.
Reflux monitoring can be done ‘on’ or ‘off’ PPI therapy in patients with persistent and/or atypical symptoms despite PPI therapy. The Lyon Consensus proposes that testing always be performed off therapy to demonstrate baseline AET in ‘unproven GERD’, meaning no (or low-grade) oesophagitis at endoscopy, and no prior positive pH testing.8 Testing off therapy is also recommended when done to evaluate for ARS.6 32 In contrast, the Lyon Consensus proposes that patients with ‘proven GERD’ (prior LA grade C or D oesophagitis, long segment Barrett’s oesophagus or prior abnormal pH-metry) be evaluated on double-dose PPI therapy to establish correlation between refractory symptoms and reflux episodes and/or to exclude inadequate acid suppression or poor compliance as the mechanism of persisting symptoms. This assessment requires pH-impedance (vs pH) monitoring since most reflux episodes on PPI therapy are weakly acidic (pH 4–7).48 49
Assessment of proximal oesophageal or pharyngeal reflux has also been proposed, but methodology and interpretation have not been standardised, and outcome studies are currently lacking.50–53 An additional problem with the pharyngeal pH probe designed to evaluate both aerosolised and liquid acid reflux54 is that it detects pharyngeal pH drops in the absence of concomitant oesophageal pH-impedance events,55 56 even in patients post-gastrectomy, raising questions about its accuracy.57
Interpretation of pH and pH-impedance monitoring
Among the pH monitoring metrics, AET is the most reproducible,58 is reliably extracted from automated analysis and is predictive of response from medical and surgical reflux therapy.59 60 However, the significance of an abnormal AET is proportionate to the degree of abnormality, and the Lyon Consensus proposes that AET <4% be considered definitively normal (physiological) and >6% be considered definitively abnormal6 with intermediate values between these limits being inconclusive. Another outcome metric of pH-impedance monitoring is the number of reflux episodes (acidic, weakly acidic or weakly alkaline) with the caveat that this is overestimated by the automated analysis and requires manual review of the tracing.61 The Lyon GERD Consensus proposes that >80 reflux episodes per 24 hours are definitively abnormal, while a number <40 is physiological6 and intermediate values inconclusive. The clinical relevance of an abnormal number of reflux episodes remains incompletely defined, although recent preliminary data demonstrate improvement of regurgitation verified by increased reflux episodes following magnetic sphincter augmentation.62 Consequently, this is considered an adjunctive measure to be used when AET is inconclusive (ie, between 4% and 6%). pH-Impedance monitoring assists diagnosis of belching disorders and rumination, which can mimic reflux disease. Additional impedance parameters such as bolus exposure, baseline impedance and postreflux swallow-induced peristaltic wave (PSPW) also have potential as reflux metrics, but outcome data are currently limited.
Reflux-symptom association
Both pH monitoring and combined pH-impedance monitoring provide analysis of the temporal association between symptoms with a crisp onset (eg, heartburn, regurgitation, chest pain, cough or belching) and reflux episodes.63 The time window applied for reflux-symptom association analysis is 2 min.64 65 The Symptom Index (SI) is the percentage of symptom events preceded by reflux episodes,66 and the optimal SI threshold for heartburn is 50%.67 The disadvantage of the SI is that the number of reflux episodes is not considered leaving open the possibility of chance association. The Symptom Association Probability (SAP) and the Ghillebert Probability Estimate (GPE), also known as Binomial Symptom Index (BSI), use more complex statistical calculations to express the probability that symptom events and reflux episodes are associated68 69 and are considered positive if the probability (P value) of the observed association occurring by chance is <5%. Both SAP and GPE/BSI take all relevant components, that is, total numbers of symptom events, reflux episodes and reflux-related symptom events, into account. In summary, SI is a measure of ‘effect size’, whereas SAP is a measure of probability. As such the two metrics are complementary, measure different things and cannot be compared with each other. The combination of a positive SI and positive SAP provides the best evidence of a clinically relevant association between reflux episodes and symptoms.6 70 71 Both the SI and SAP are predictive of the effect of medical and surgical antireflux therapy, independent of AET.72–75
The reliability of reflux-symptom association analysis is critically dependent on proper execution of the reflux monitoring procedure and meticulous analysis protocols including careful selection of symptoms of interest. Patients must be instructed to use the symptom event button on the portable data logger accurately and to fill in the symptom diary accurately. The outcome of symptom association analysis is more reliable when at least three symptom events occur during the test.6 When cough is the symptom of interest, an automated acoustic or manometric cough monitor is necessary to accurately capture cough events.76 77 Prolonged wireless pH monitoring increases the yield of symptom association analysis,40 41 as does combined pH-impedance monitoring with the detection of weakly acidic reflux episodes.78 This requires manual analysis, as automated analysis significantly overdetects weakly acidic reflux episodes and inaccurately reports association with non-acid reflux events in nearly 20% of cases.61 However, ‘rapid’ visual analysis limited to the 2 min window preceding each symptom event yields SI and SAP values concordant with a full visual analysis, with excellent intraobserver and interobserver agreement.79 Although pH-impedance monitoring provides analysis of symptom-reflux association on PPI therapy, testing off PPI therapy increases the number of symptoms reported, which increases the chance of a positive symptom-reflux association.80
Reflux-symptom association analysis has a high degree of reproducibility, the SI being somewhat less reproducible than the SAP.81 Monte Carlo simulations have identified limitations of reflux-symptom association analysis, especially when acid exposure is low and symptom events are few.82 83 If new methods for reflux-symptom association are developed in the future, rigorous outcome testing will be needed to define superiority to the existing metrics.
Novel metrics
Two novel impedance-detected parameters, the PSPW index and baseline impedance have been investigated within GERD phenotypes.84 85 These metrics may augment the diagnostic value of impedance-pH testing, especially in discriminating patients with GERD from those with functional heartburn.86–88 In health, reflux episodes trigger primary peristalsis to neutralise acidified oesophageal mucosa with saliva. This is evident as the antegrade progression of impedance decline within 30 s of a reflux episode (PSPW) on a pH-impedance study.87 The PSPW index, which currently requires cumbersome manual calculation as it is not programmed into the analysis software, consists of the proportion of reflux episodes on pH-impedance monitoring followed by a PSPW. The PSPW index reflects the integrity of primary peristalsis stimulated by reflux episodes, correlates with contraction reserve assessed using multiple rapid swallows (MRS)89 and has excellent performance characteristics in differentiating erosive oesophagitis and pathological acid exposure from functional heartburn and controls (sensitivity 99%–100%, specificity 92%).87 90
Baseline impedance values reflect the permeability of the oesophageal mucosa, both in animal models and healthy volunteers, with lower values found in erosive and non-erosive GERD.91 92 Low baseline oesophageal mucosal impedance has been linked to alteration in intercellular space and tight junctions93 94 and to reflux symptoms.95 Since frequent swallows and reflux events impact measurement, baseline impedance is best measured from pH-impedance tracings during sleep, termed mean nocturnal baseline impedance (MNBI) when averaged from three 10 min periods spaced an hour apart.84 MNBI is lower in persisting erosive oesophagitis compared with healed oesophagitis,96 in PPI-responsive NERD and chronic cough compared with PPI-refractory states,84 97 and in erosive oesophagitis, NERD and reflux hypersensitivity compared with functional heartburn and healthy controls.86 87 93 Low MNBI (<2292 ohms) independently predicts response to antireflux therapy,98 links PPI responsive heartburn to reflux better than AET90 and improves with healing oesophagitis.99 100
Baseline impedance can also be directly measured from the oesophageal mucosa. Initially, this was done using probes with impedance sensors that were passed through the endoscope. Subsequently, the design has improved using two radial sensors mounted on a 10 cm balloon that is inflated to insure optimal contact with a long segment of oesophageal mucosa. Baseline mucosal impedance values correlate with oesophageal mucosal inflammation, differentiating erosive and non-erosive GERD from eosinophilic oesophagitis and normal patients with better specificity (95% vs 64%) and positive predictive value (96% vs 40%) compared with pH monitoring.101–103 Similar to baseline impedance from pH-impedance monitoring, values normalise following PPI therapy. Although normative values are not yet available, ongoing studies should clarify the role of mucosal impedance measurements in GERD management.
Oesophageal high-resolution manometry
A common indication for high-resolution manometry (HRM) is to accurately place pH or pH-impedance catheters. HRM is also used to assess peristalsis and to detect alternative major motor disorders prior to ARS or when symptoms do not improve with GERD therapy. Consequently, HRM studies are often performed in the setting of GERD. Nonetheless, although fundamental to GERD pathophysiology, a pathophysiological classification of motor findings in GERD was only recently described.7
EGJ barrier function
The most fundamental abnormality in GERD is incompetence of the EGJ as an antireflux barrier, making quantifying EGJ competence an attractive biomarker. However, the EGJ is a complex sphincter composed of both the crural diaphragm (CD) and lower oesophageal sphincter (LES), the relative dominance of which varies with circumstance. The EGJ pressure varies with time, respiration and swallowing;, similarly the EGJ morphology can also vary over time, transitioning between superimposed and separated CD and LES elements.104 Furthermore, some degree of EGJ incompetence is physiological, evident by the phenomenon of transient LES relaxation (TLESR), reflex relaxation of both the LES and CD that facilitates gas venting from the stomach.105 Clearly, there are challenges to quantifying EGJ barrier function.
No single HRM metric adequately summarises EGJ competence. Hence, the Lyon Consensus proposes adopting two metrics, one expressing the anatomical morphology of the EGJ and the second summarising its contractile vigour. EGJ morphology, defined by the relationship between the LES and CD, has been characterised into three subtypes on HRM106 107: type 1 with superimposed LES and CD, type 2 with axially separated LES and CD pressure signals separated by <3 cm and type 3 with a ≥3 cm separation between the LES and CD pressure signatures (figure 1). Type 3 EGJ morphology is associated with reduced LES pressure and lower inspiratory augmentation, which correlates with reflux severity.106 108 109 However, this relationship is not linear and there are clear exceptions.
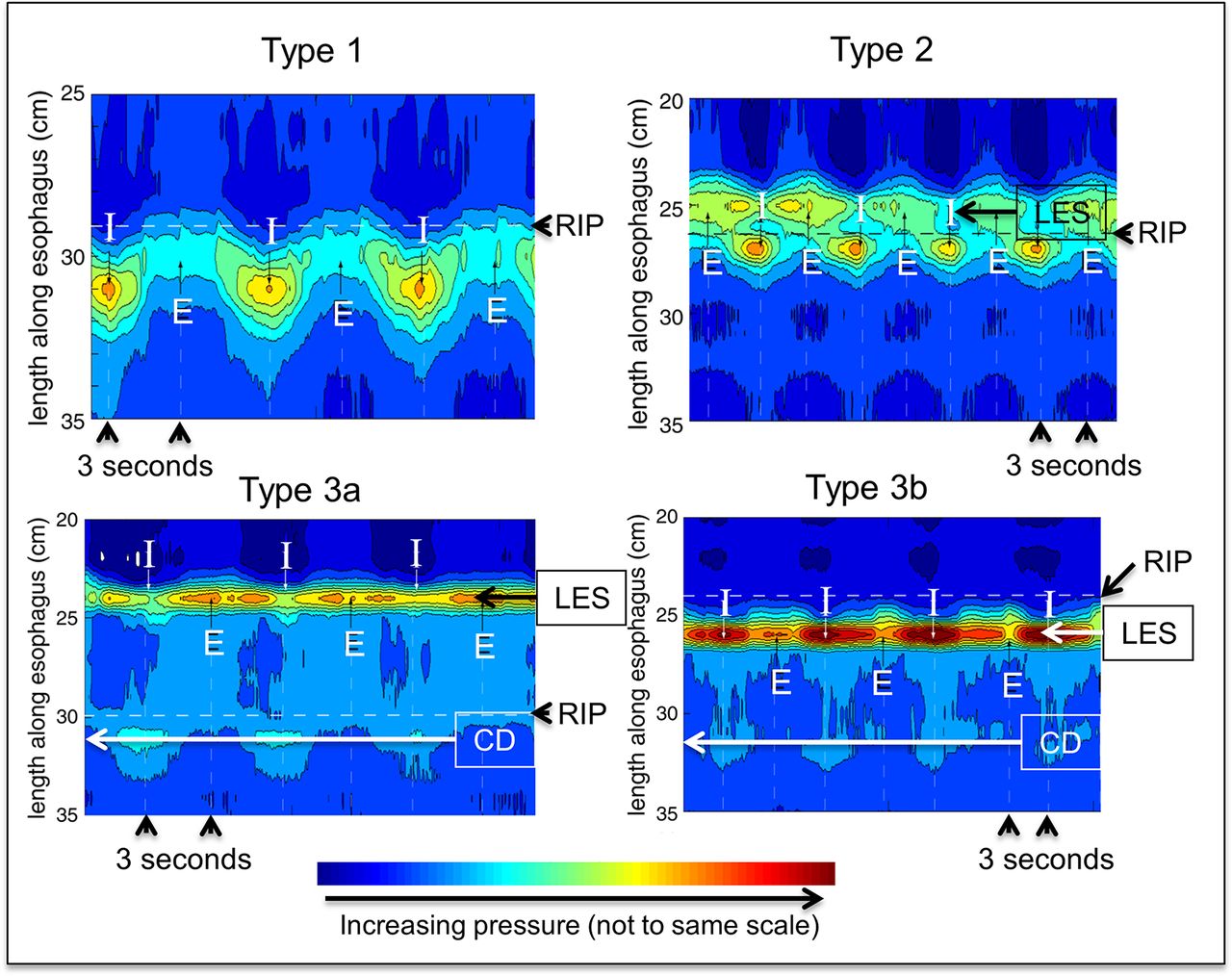
Oesophagogastric junction morphology as depicted in HRM. With type 1 morphology the crural diaphragm (CD) component, evident during inspiration (I), is completely superimposed of the lower oesophageal sphincter (LES) component such that the magnitude of the actual LES pressure is not discernible. With type 2 morphology, there is partial separation of the LES and CD constituents, but the respiratory inversion point (RIP) remains at the level of the CD, evident by the decrease observed in the LES pressure band during inspiration. Other characteristics of type 2 morphology are that the LES-CD separation is <3 cm and that the pressure trough between the LES and CD is greater than intragastric pressure. With type 3 morphology, there is ≥3 cm separation between the LES and CD and the pressure trough between the two is equal to intragastric pressure during expiration (E). However, the RIP remains at the level of the CD in type 3a and elevated to the level of the LES pressure band with type 3b. This is evident by the decreases in LES pressure during inspiration in type 3a and increases in LES pressure during inspiration in type 3b.
The second HRM metric to quantify EGJ barrier function is the EGJ contractile integral (EGJ-CI) (figure 2). The EGJ-CI is calculated using methodology analogous to that for calculating the distal contractile integral (DCI) with the DCI box set to encompass the LES and CD over a period of three respiratory cycles above a threshold of gastric pressure. The calculated ‘DCI’ is then divided by the duration of the three respiratory cycles to make it independent of time and expressed in units of mm Hg·cm.110 Several groups of investigators have subsequently tested the performance of the EGJ-CI in segregating GERD populations (table 1),110–114 with general agreement that this metric identifies a subset of patients with severe barrier dysfunction prone to either endoscopic oesophagitis or unequivocally abnormal reflux testing. However, it is also evident from the spread of normal ranges reported among these studies that there are likely methodological discrepancies in exactly how the EGJ-CI is calculated. In view of this, the Lyon Consensus concluded that the EGJ-CI is a promising metric, but needs further research before widespread adoption. In an attempt to standardise methodology among groups, they recommended exclusion of CD component of the EGJ in instances of type 3 EGJ morphology and calculation of EGJ-CI above the gastric baseline pressure.

High-resolution manometry metrics used in the motor classification of GERD. The oesophagogastric junction contractile integral (EGJ-CI) measures vigour of the EGJ barrier using a software tool that encompasses length and vigour of the EGJ above the gastric baseline. The measurement is made over three respiratory cycles during quiet rest, and corrected for duration of respiration. The distal contractile integral (DCI) measures vigour of smooth muscle contraction taking length, duration and amplitude of contraction into consideration. Following a series of repetitive swallows (multiple rapid swallows (MRS)), DCI augments higher than mean DCI from single swallows when there is contraction reserve.
Studies that have compared the EGJ-CI among patient and control populations. Values reported at median (IQR)
Further insight into the genesis of the EGJ-CI has been gleaned through studies using three-dimensional (3D)-HRM.115 Isolation of the CD component of the composite EGJ signal on 3D-HRM concluded that approximately 85% of overall EGJ contractility was attributable to the CD.116 Furthermore, analysis of 3D-HRM recordings differentiating the CD and LES constituents of the EGJ pressure complex demonstrated that the CD component correlated strongly with the EGJ-CI, suggesting that both are largely determined by CD contractility.117 Together, these studies provide physiological support for adopting the EGJ-CI as a good summary metric of EGJ barrier function, although with the caveat that the metric is largely an indicator of CD contractility.
Oesophageal peristaltic function
Oesophageal peristalsis can be characterised by the DCI which summarises the vigour of post-transition zone contraction (figure 2).107 A DCI threshold of 450 mm Hg·cm·s correlates with an averaged distal peristaltic amplitude of 30 mm Hg118, the original manometric threshold defining ineffective swallows. When abnormal, oesophageal peristalsis is often weak in GERD,119–121 with poor and/or delayed formation of post-transition zone contraction segment.122 This can result in major breaks (>5 cm) in the peristaltic contour even when contraction vigour is preserved, a condition termed fragmented peristalsis when ≥50% of test swallows demonstrate this finding.107
Peristaltic dysfunction becomes progressively more common going from NERD to erosive oesophagitis, to Barrett’s oesophagus.123 124 High proportions of ineffective contractions increase the likelihood of abnormal AET, particularly while supine,125 and increase the likelihood of reflux symptoms.126 The Chicago Classification defines ineffective oesophageal motility (IEM) as ≥50% of test swallows with DCI <450 mm Hg·cm·s, inclusive of any combination of weak (DCI 100–450 mm Hg·cm·s) or failed (DCI <100 mm Hg·cm·s) sequences.107 Failed sequences are more predictive of an abnormal AET than a similar proportion of weak sequences.127 The greatest reflux burden is seen with absent contractility (100% of test swallows with DCI <100 mm Hg·cm·s).128
Provocative tests
The physiological phenomenon of deglutitive inhibition is more pronounced with multiple swallows in rapid succession such that the oesophagus remains in inhibition until after the final swallow, which is then followed by a peristaltic contraction.129 MRS and rapid drink challenge (RDC) are two provocative tests of the integrity of deglutitive inhibition during HRM.130 With MRS, five 2 mL swallows are taken <4 s apart and with RDC 200 mL of water is swallowed within 30 s. The Lyon Consensus proposes that every HRM study should be accompanied by at least one of these provocative tests.
Post-MRS contractions are an indicator of ‘contraction reserve’ in the oesophagus, the phenomenon wherein the post-MRS contraction has greater DCI than the preceding test swallows (figure 2).131 Recent data suggest three MRS sequences for reliable assessment of contraction reserve.132 The absence of contraction reserve in IEM is predictive of the poor efficacy of promotility drugs,133 higher AET in NERD,89 outlet obstruction and subsequent benefit from dilation following ARS134 135 and persistence or development of IEM after ARS.136 Absent contraction reserve is also the most common manometric finding in systemic sclerosis.137 The Lyon Consensus accepted the value of adopting MRS into HRM protocols for determining contraction reserve in IEM or absent contractility,107 acknowledging that MRS is the most widely studied provocative test,131 135 138 provides a computationally simple endpoint (peristaltic augmentation ratio: post-MRS vs pre-MRS)137 and is quick and easy to perform.
In contrast to MRS, the most important clinical application of RDC is in distinguishing EGJ obstruction from achalasia, by identifying LES relaxation in the former, and an exaggerated pressure gradient across a non-relaxed EGJ in the latter.139–141 Therefore, RDC is most helpful in detecting panoesophageal pressurisation in achalasia, identifying increased resistance to EGJ outflow and uncovering latent hypercontractility.139 Additionally, RDC may offer supportive evidence for erosive GERD; effective post-RDC peristalsis was seen in 83% of healthy controls compared with 70% of patients with NERD and only 30% of patients with erosive oesophagitis.142 Solid test meals have also been used as provocative tests during HRM, mainly in evaluating transit symptoms.142–145 Normal values of oesophageal pressure responses to RDC and solid meals have been recently reported in normal healthy volunteers.145 146
HRM studies performed during the postprandial period could be of interest for identification of pathophysiological mechanisms in GERD,147 148 particularly reflux episodes that tend to be postprandial. A reflux episode may occur during a TLESR, from low LES pressure, or in conjunction with rumination (increased gastric pressure with or without decreased thoracic pressure) or supragastric belching (air swallowing to initiate belching).147 Postprandial HRM has also been used to evaluate the efficacy of drugs targeted to TLESRs, rumination and supragastric belching.149 150 However, several limitations exist, including lack of normative postprandial HRM data, difficulties with standardisation of the test meal and unclear optimal duration of the recording period.
Classification of motility findings in GERD
The most common motility pattern in GERD is a normal study. However, either the EGJ or the oesophageal body, or both can be abnormal. The EGJ can be hypotensive, with or without a hiatus hernia. Peristalsis can be fragmented, ineffective or absent, with or without contraction reserve. The Lyon Consensus endorses the hierarchical classification of motility findings in GERD first evaluating EGJ morphology and function with LES-CD separation and the EGJ-CI, second characterising the integrity of peristalsis as normal, weak, fragmented or absent and third, evaluating for contraction reserve7 (table 2). This classification is intended to be used in conjunction with the Chicago Classification.
Classification of motor function in GERD using oesophageal high-resolution manometry
Advances since the Porto Consensus
The Lyon Consensus builds on the Porto Consensus of 2002,45 providing recommendations for the use and interpretation of reflux testing techniques in 2018 including oesophageal HRM and baseline impedance measurement that were not widely available in 2002 (table 3). The primary indication for reflux testing is in distinguishing among patients with pathological reflux burden, reflux-mediated hypersensitivity and functional syndromes (table 4).151 The Lyon Consensus attempts to augment this approach by stratifying the significance of findings into those that are conclusive of pathological GERD, as opposed to suggestive of the diagnosis (figure 3). The Lyon Consensus also proposes the concept of ‘borderline’ or inconclusive evidence when additional evidence can sway the final judgement towards or away from GERD. This is an area where novel metrics and diagnostic techniques may prove helpful. Conditions that can mimic GERD, such as achalasia, supragastric belching and rumination syndrome need to be excluded with appropriate testing.
{kind=link}
{kind=link}
{kind=link}
Interpretation of oesophageal test results in the context of GERD. Any one conclusive finding provides strong evidence for the presence of GERD. While a normal EGD does not exclude GERD on its own, this provides strong evidence against GERD when combined with AET <4% and <40 reflux episodes on pH-impedance monitoring off proton pump inhibitor therapy. When evidence is inconclusive or borderline, adjunctive or supportive findings can add confidence to the presence or absence of GERD. Histopathology as an adjunctive measure requires a dedicated scoring system (incorporating papillary elongation, basal cell hyperplasia, DIS, intraepithelial inflammatory cells, necrosis and erosions) or evidence of DIS on electron microscopy. However, adjunctive findings, particularly histopathology and motor findings in isolation, are not enough to diagnose GERD. AET, acid exposure time; DIS, dilated intercellular spaces; MNBI, mean nocturnal baseline impedance; HRM, high-resolution manometry; PSPWI index, postreflux swallow-induced peristaltic wave index; EGJ, oesophagogastric junction. *Factors that increase confidence for presence of pathological reflux when evidence is otherwise borderline or inconclusive.
Comparison of the Porto and the Lyon Consensus conclusions
GERD phenotypes predicting abnormal reflux burden from clinical evaluation and oesophageal testing
Optimisation of GERD testing
GERD symptoms are diverse, response to treatment is variable, pathogenesis is heterogeneous and mechanistic phenotypes are heavily influenced by hypersensitivity and hypervigilance. Because simple algorithms starting with a PPI trial do not consider these complex phenotypes of GERD, they often lead to inappropriate PPI utilisation, delayed diagnosis and inaccurate diagnoses.152 The Lyon Consensus opines that the optimal initial testing for PPI non-responders with no prior endoscopic or pH-metry demonstration of GERD is pH or pH-impedance monitoring done withholding antisecretory therapy. A key potential outcome of that testing is to rule out GERD and to redirect management towards weaning off PPIs, using neuromodulators and/or cognitive behavioural therapy as appropriate. In contrast, optimal testing in poorly responsive patients with a prior demonstration of GERD is the combination of EGD, HRM and pH-impedance monitoring done on twice-daily PPI therapy. This combination of tests serves both to redirect therapy towards alternative diagnoses and to mechanistically subtype patients in terms of poor clearance, excessive reflux episodes and hypersensitivity (table 4), each of which can trigger specific management options. The precise roles of baseline impedance, PSPW index and provocative manoeuvres on HRM remain to be clarified with future research.
Outcome measures in GERD
The optimal use of diagnostic testing may translate into better therapeutic outcomes, but appropriate outcome measures are necessary to properly evaluate that improvement. Oesophagitis healing is a common measure for therapeutic trials, but visible oesophagitis is rare in patients with refractory GERD symptoms,24 and the objective of the evaluation is to determine if refractory symptoms are attributable to GERD or not. Hence, potentially relevant outcome measures are symptom description,153 symptom questionnaires,154 pictograms with visual depictions of symptoms155 156 and ambulatory reflux monitoring with analysis of reflux-symptom association.74 157 Outcome measures typically used in GERD therapeutic trials have included individual symptom assessment with Likert or visual analogue scales,158 global outcome evaluations on Likert scales,159 adequate versus inadequate relief, disease-specific questionnaires160 and quality of life questionnaires. Looking to the future, regulatory agencies have stipulated that validated patient-reported outcome questionnaires (PROs) and quality of life questionnaires will be requisite in future therapeutic trials. Such PROs require a fastidious approach that includes item generation, testing for reliability, responsiveness, validity and interpretability and finally, cross-cultural adaptation when applicable, for each diagnostic category.161
Conclusions and future direction
GERD is a complex disease with a heterogeneous symptom profile and a multifaceted pathogenic basis that defies a simple diagnostic algorithm or categorical classification. The Lyon Consensus defines parameters on oesophageal testing that conclusively establish the presence of GERD and characteristics that rule out GERD. Additional evidence from reflux-symptom association, motor findings on HRM, novel metrics from pH-impedance monitoring, baseline mucosal impedance and PPI response complement oesophageal testing when pH-metry is borderline or inconclusive. While acknowledging the limitations of currently available oesophageal testing in GERD, the Lyon Consensus proposes this model as a guide to direct management.
The future approach to phenotyping patients with GERD should focus on assessing important physiological biomarkers and PROs to categorise patients based on the severity of refluxate exposure, mechanism of reflux, effectors of clearance and underlying EGJ pathophysiology (table 4), while recognising that no single approach is perfect. Novel metrics assessing tissue resistance, oesophageal clearance, peripheral and central neural integration and psychometrics will allow for a tailored therapeutic approach including pharmacological treatments, surgical/endoscopic interventions and behavioural strategies targeting the underlying defect(s) in the antireflux barrier, oesophageal clearance, visceral sensitivity and cognitive response to reflux. As newer metrics emerge, the Lyon Consensus plans future meetings to update and adapt the consensus conclusions. Collaboration between high volume medical centres involved in GERD testing has opened possibilities for more robust normative data and for validation of conclusions and recommendations from the Lyon Consensus. As the GERD diagnostic paradigm evolves, using diagnostic testing to define a precision approach tailored to the individual patient becomes possible. The goals of evaluation should therefore transition towards defining GERD phenotypes to facilitate tailored treatment.
Acknowledgments
The authors wish to acknowledge the International Working Group for Gastrointestinal Motility and Function for initiating the consensus meetings and for providing material support for the consensus process. This process was endorsed by the European Society of Neurogastroenterology and Motility (ESNM) with representation and support from members of the American Neurogastroenterology and Motility Society (ANMS), the South American and Latin Society (SLNG), the Asian Neurogastroenterology and Motility Association (ANMA) and members of the Australasian Neurogastroenterology and Motility Association (ANGMA). Financial support was provided by the United European Gastroenterology (UEG) Education Committee, registration fees for meetings and sponsorship from major manufacturers of physiological measurement equipment.
References
Footnotes
Contributors All authors contributed to the content of the manuscript, and reviewed, edited and approved the final draft.
Funding The consensus process was supported by the Working Group for Gastrointestinal Motility and Function. This group received an educational grant from United European Gastroenterology (UEG).
Competing interests CPG: consulting: Ironwood, Torax, Quintiles; teaching and speaking: Medtronic, Diversatek, Reckitt-Benckiser. ES: consulting: AbbVie, Allergan, MSD, Takeda, Sofar, Janssen; teaching and speaking: Medtronic, Reckitt-Benckiser, Malesci, Zambon. FZ: research support: Medtronic, Sandhill Scientific; consulting: Allergan, Reckitt-Benckiser; speaking and teaching: Ipsen Pharma, Biocodex, Coloplast, Takeda, Vifor Pharma, Mayoly Spindler. PJK: consulting: Ironwood. FM: teaching and speaking: Laborie, Medtronic; consulting: Allergan, Endostim. AJPMS: none. MV: Vanderbilt University and Diversatek co-own patent on mucosal impedance technology. DS: research support: Diversatek, Reckitt-Benckiser; OMOM, Jinshan Science & Technology (Group) Co. Ltd., Chongqing, China. MRF: research support: Given Imaging/Covidien, Reckitt Benckiser, Mui Scientific. Educational events: Given Imaging/Covidien, MMS, Sandhill Scientific Instruments. Speaking and teaching: Given Imaging/Covidien, Reckitt Benckiser, Shire, Almirall. MV: consulting: Torax. RT: teaching: Laborie. JT: consulting: Ironwood. AJB: research support: Danone, Bayer; speaking and/or consulting: MMS, Astellas, AstraZeneca, Bayer, Almirall and Allergan. JP: research support: Impleo; speaking and/or consulting: Medtronic, Diversatek, Torax, Ironwood, Takeda, AstraZeneca; stock options: Crospon. SR: research support: Sandhill Scientific, Crospon; teaching: Medtronic; speaker: Mayoly Spindler.
Provenance and peer review Commissioned; externally peer reviewed.
Correction notice This article has been corrected since it published Online First. The acknowledgement and funding statements and affiliation for Mark Fox have been updated.