Article Text

Abstract
Timely detection of oesophageal adenocarcinoma (OAC) and even more so its precursor Barrett’s oesophagus (BO) could contribute to decrease OAC incidence and mortality. An accurate, minimally-invasive screening method for BO for widespread use is currently not available. In a proof-of-principle study in 402 patients, we developed and cross-validated a BO prediction model using volatile organic compounds (VOCs) analysis with an electronic nose device. This electronic nose was able to distinguish between patients with and without BO with good diagnostic accuracy (sensitivity 91% specificity 74%) and seemed to be independent of proton pump inhibitor use, the presence of hiatal hernia, and reflux. This technique may enable an efficient, well-tolerated, and sensitive and specific screening method to select high-risk individuals to undergo upper endoscopy.
- barrett's oesophagus
- oesophageal cancer
- screening
- breath tests
- endoscopy
Statistics from Altmetric.com
Study background
The incidence of oesophageal adenocarcinoma (OAC) has risen by sixfold over the last few decades.1 The majority of patients with OAC present with advanced disease, resulting in poor survival rates.2 Although Barrett’s oesophagus (BO) is a known precursor of OAC, >90% of patients with OAC never had prior endoscopy and OAC is usually diagnosed outside BO surveillance.3 Upper endoscopy, the current standard for BO detection, is invasive and expensive and therefore not suitable for population-based screening. Analysis of volatile organic compounds (VOCs) in exhaled breath may be a promising technique to detect undiagnosed cases of BO in the population.4 VOCs are gaseous end products resulting from physiologic metabolic processes in the body, pathophysiologic processes such as inflammation or oxidative stress-related activity, or external factors such as medication use or changes in the microbiome.5 Therefore, VOC profiles may serve as a biomarker for various diseases. Electronic noses represent a potential technique for real-time, high throughput exhaled VOC pattern analysis. In this multicentre, proof-of-principle study, we assessed the accuracy of exhaled VOCs analysis using an electronic nose device for detection of BO compared with endoscopy and biopsy as the reference standard.
Methods
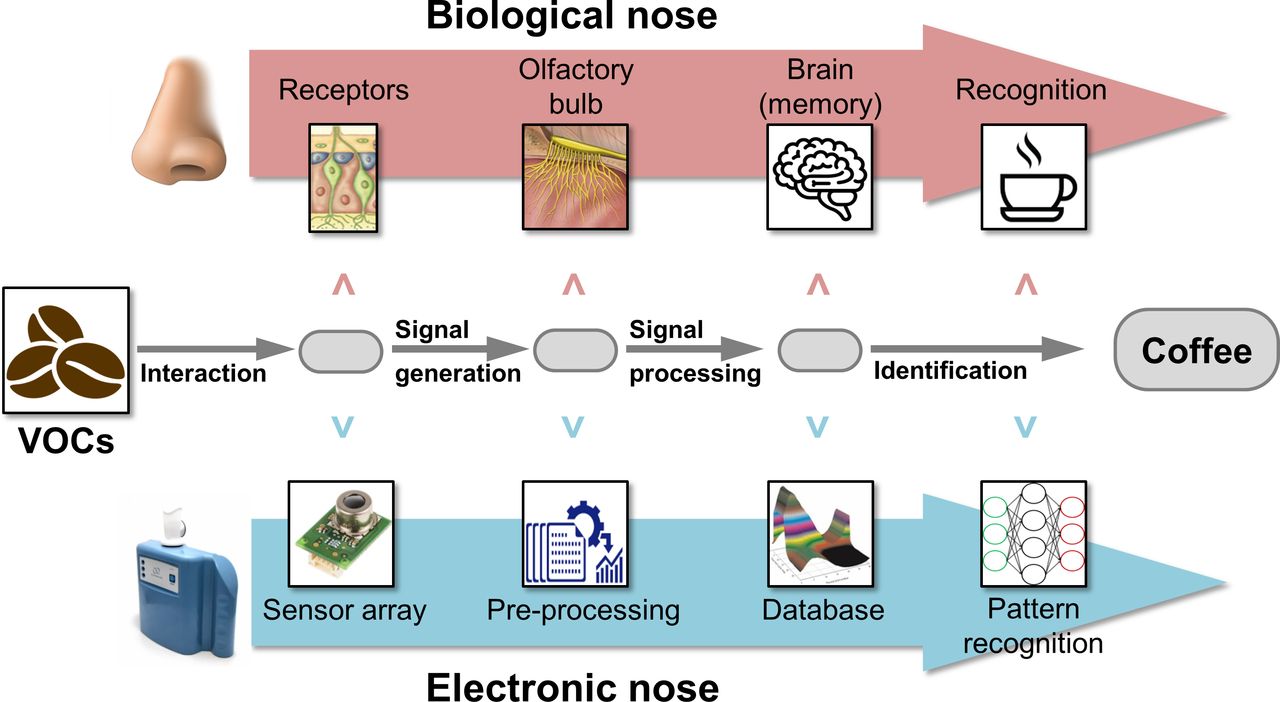
Adult patients undergoing a clinically indicated upper endoscopy were invited to provide a 5 min breath sample using an electronic nose immediately before a scheduled endoscopy. VOC analysis by an electronic nose device is based on pattern recognition and resembles mammalian olfaction (figure 1).6 7 The Aeonose (the eNose company, Zutphen, the Netherlands) consists of three metal-oxide sensors and uses chemical to electrical interfaces to measure subtle VOC profiles of different diseases in exhaled breath. Data were analysed by an artificial neural network in a supervised fashion to identify data classifiers to extract breath print differences between patients with BO, gastro-oesophageal reflux disease (GORD), and controls. Leave-10%-out cross-validation of data was performed after training the artificial neural network to make sure the prediction model generated was disease-specific. More details on the methods and the electronic nose technology can be found in the online supplementary file.8 9
Supplemental material
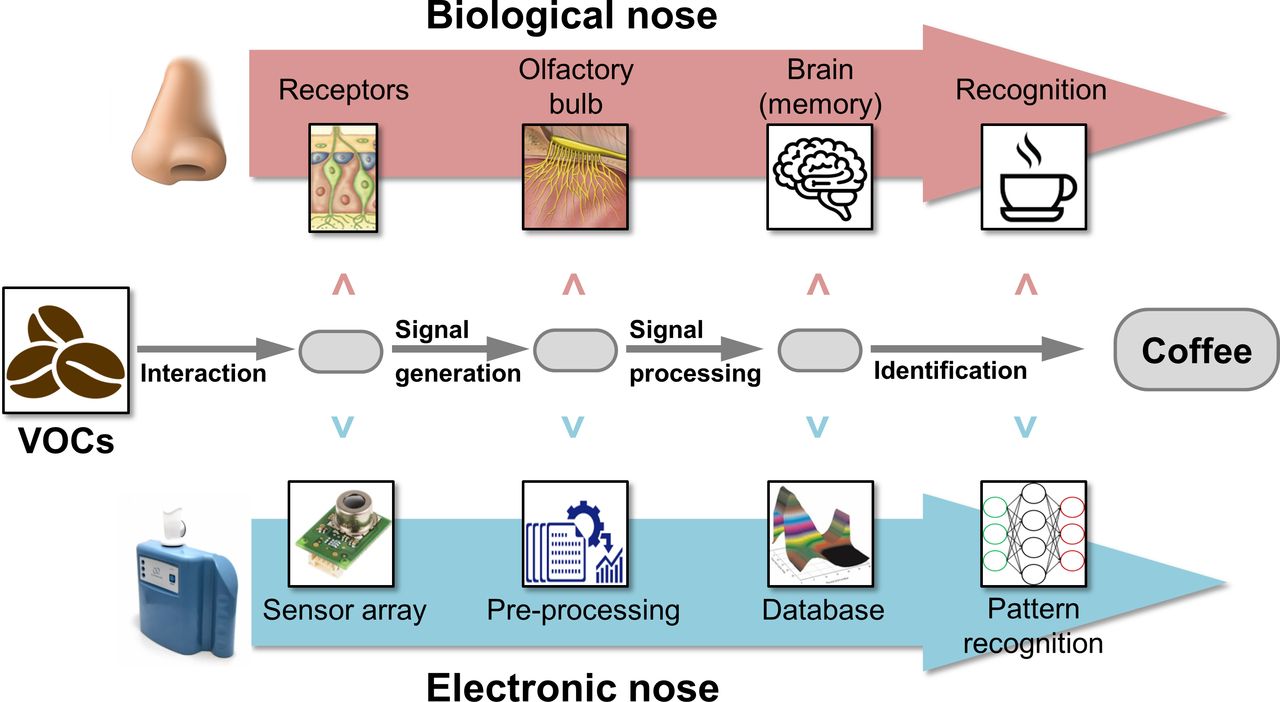
The electronic nose concept resembles mammalian olfaction. Volatile organic compounds (VOCs) are presented to a metal-oxide sensor array. VOCs interact with these sensors based on their chemical characteristics. Combinations of individual sensor measurements generate a digital signal, which can be analysed by pattern recognition and artificial neural networks. Adapted from Santos et al. 7
Results
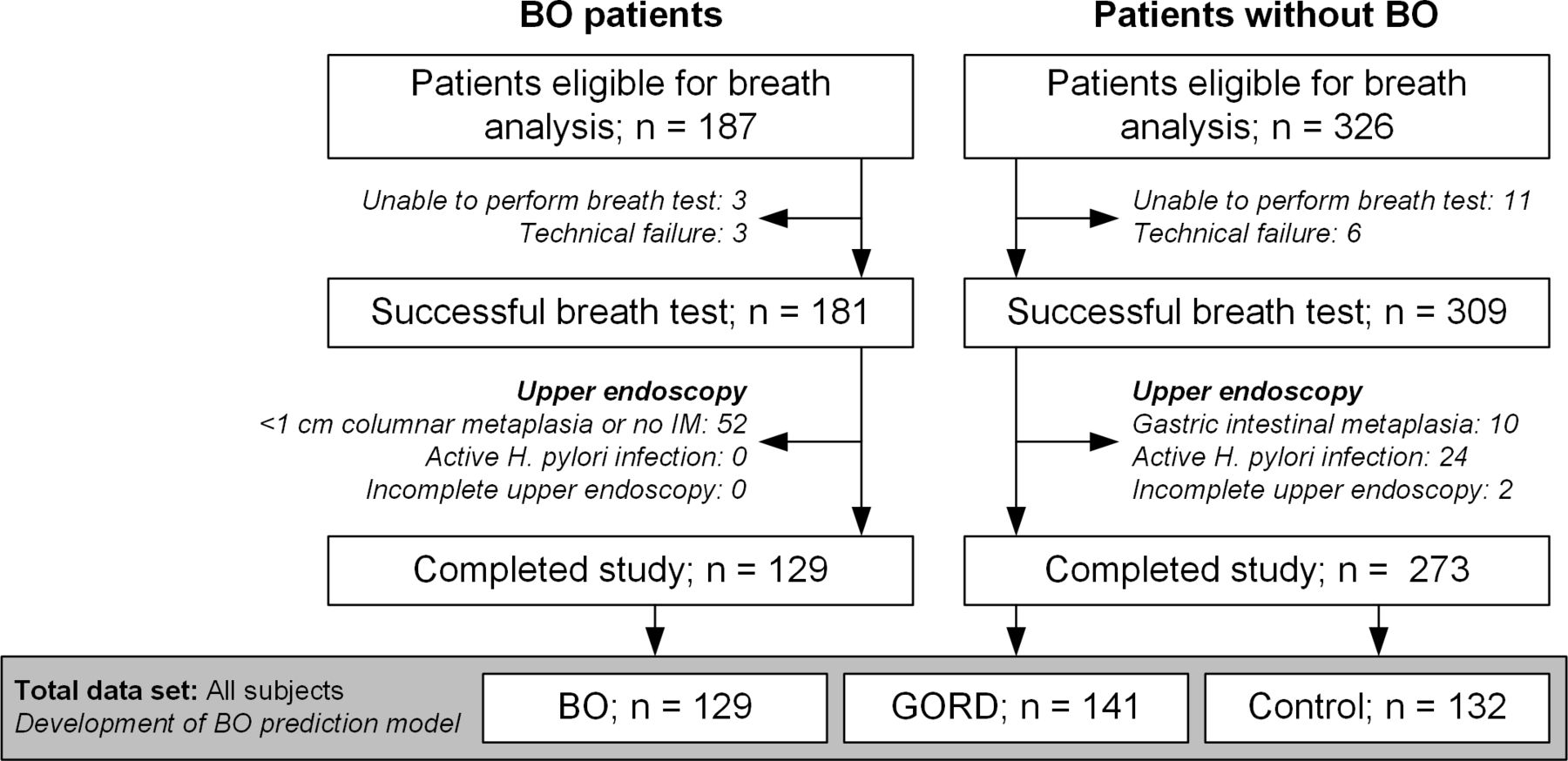
Breath samples were obtained from 513 individuals, resulting in a patient acceptability rate of 91.4% (figure 2). No adverse events were observed during breath analysis. After exclusions, 402 patients in total were included; 129 patients with BO, 141 patients with GORD (50 with reflux oesophagitis (35.5%)), and 132 patients in the control group. In the latter group, 76 (57.6%) patients had a normal upper gastrointestinal tract on endoscopy or only the presence of a hiatal hernia. Table 1 summarises the main characteristics of all patients enrolled in this study.

Study flowchart. BO, Barrett’s oesophagus; GORD, gastro-oesophageal reflux disease; IM, intestinal metaplasia.
Characteristics of the total study cohort (n=402)
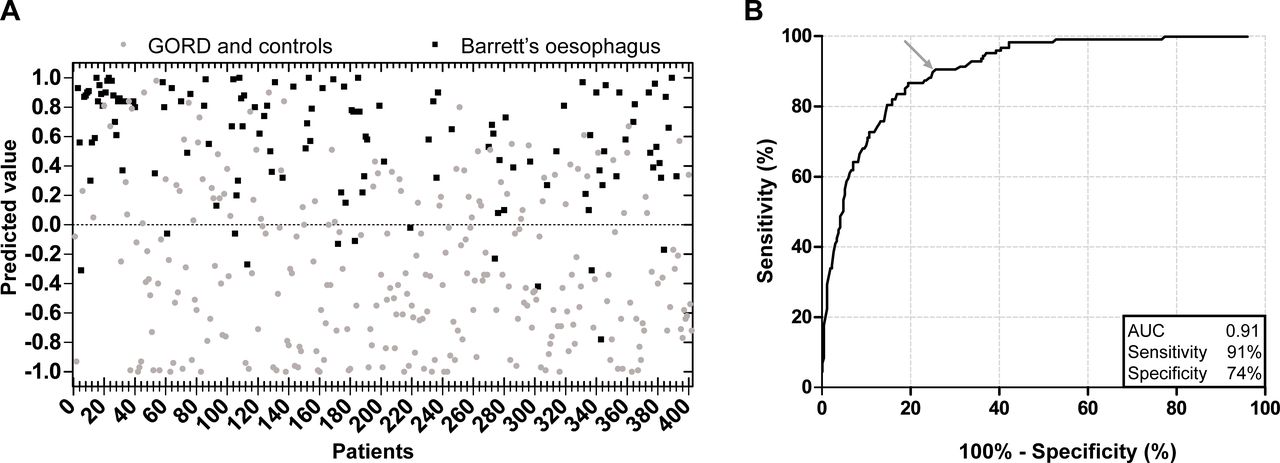
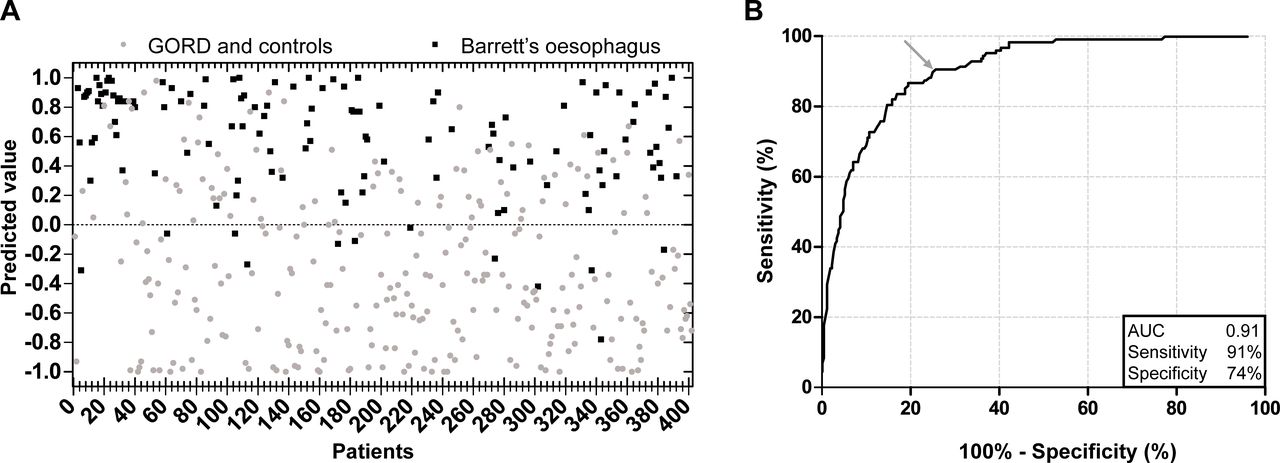
VOC profiles of patients with BO differed significantly from GORD patients and healthy controls (figure 3A). The cross-validated prediction model demonstrated the ability to detect BO with 91% (95% CI 84% to 95%) sensitivity, 74% (95% CI 69% to 79%) specificity, and an area under the curve (AUC) of 0.91 (95% CI 0.87 to 0.94). To limit the number of false-positive results (type 1 errors), a different cut-off point in the receiver operating curve can be selected with a corresponding specificity of the electronic nose for BO of 86% at the expense of test sensitivity which decreases to 71% (figure 3B). In addition, breath prints of BO patients could be differentiated from GORD patients with 64% (95% CI 55% to 72%) sensitivity and 74% (95% CI 66% to 81%) specificity (AUC 0.73, 95% CI 0.67 to 0.79). Sensitivity for detecting BO increased with length of the BO segment (M ≥3 cm) to 96% (95% CI 90% to 99%). To assess the robustness of the model and the effect of confounding factors, sensitivity analyses were performed including only patients using proton pump inhibitors (PPIs) for at least 1 month before study enrolment (n=300) and only patients with a hiatal hernia (n=205). Both analyses still showed a fair to good diagnostic accuracy for discriminating BO from GORD patients and controls (table 2).
{kind=link}
{kind=link}
{kind=link}
Scatter plot and receiver operating characteristic (ROC) curve of the cross-validated disease-specific model for detecting Barrett’s oesophagus (BO) based on 129 breath tests of patients with BO and 273 breath tests of gastro-oesophageal reflux disease (GORD) and control patients. (A) Scatterplot with optimal cut-off value. Values between −1 and +1 indicate the degree to which a subject was classified as positive (maximum value +1) or negative (minimum value −1) for BO. (B). ROC curve for detecting BO. AUC,area under the curve.
Diagnostic performance of 10-fold cross-validated VOC analyses of breath samples of Barrett’s oesophagus, GORD patients and controls
Comments
The limitations of the currently recommended screening method for BO, upper endoscopy, have initiated the development of novel, minimally invasive screening techniques that can be performed in a primary care setting.10 11 This proof-of-concept study indicates that exhaled breath VOCs hold great potential for the non-invasive identification of patients most likely to have BO, thus at higher risk of developing OAC. Hence, it could be possible to reduce mortality from OAC in patients at risk, who otherwise would not have undergone upper endoscopy.
The findings of our study provide evidence that patients with BO have VOC breath prints different from those without BO. We showed as a proof of concept that it is possible to non-invasively detect the presence of BO by VOC breath analysis using an electronic nose device in patients with and without GORD with a sensitivity of 91% and a specificity of 74%. The accuracy increases with BO segment length. Models were still able to differentiate between BO and controls in sensitivity analyses, which indicates that VOC analyses were only minimally affected by confounding factors such as PPI use, GORD symptoms, and the presence of a hiatal hernia. Furthermore, the observed slight decrease in accuracy could also be attributed to the relatively low number of patients included in these sensitivity analyses.
To date, only three studies—one using VOC pattern recognition and two using mass spectrometric analysis—have been reported on VOC analysis in BO or OAC, showing a good accuracy for detecting either of them.12–14 Although evidence for VOC pattern recognition for BO is limited, analysis of VOCs in exhaled breath has been shown to be a potential diagnostic biomarker for various types of cancer, but also for the detection of several gastrointestinal diseases.15 16 Hence, exhaled breath seems to contain biomarkers with clear diagnostic potential, a finding we reproduced in this study aiming at the early detection of BO. The sensitivity and specificity of breath testing for BO are comparable to existing technologies such as mammography for breast cancer screening, faecal occult blood testing for colorectal cancer, and the cytosponge for BO.17–19
The exact biochemical mechanism of exhaled VOCs and the connection with cancer and related neoplastic lesions is still under debate. It is thought that differences in patterns of VOCs may involve changes at a genetic and cellular level causing metabolic alterations of the BO mucosa, but also changes in the local microenvironment.5 20 21 Oesophageal microbiome changes associated with BO may also be a contributing factor to the production of VOCs.22
VOC analysis based on pattern recognition of disease-specific VOC profiles is only one of the methods used for breath sampling. Other methods focus on identification and quantification of specific individual VOCs for diseases of interest using chemical analytical techniques such as gas chromatography-mass spectrometry. Although the quality is high, chemical analytical techniques are expensive, time-consuming and require well-trained personnel for its operation, analysis and maintenance.23 Therefore, electronic nose technology seems better suited for population-based screening than chemical analytical techniques, because it is fast, potentially cost-effective, and allows for real-time breath analysis results. Furthermore, the electronic nose type used in this study offers the opportunity for transferring calibration models.9 This implies that once a calibration model for BO has been developed, it can easily be transferred to other electronic nose devices and therefore enables large-scale application.
A limitation of electronic nose technology is the inability to identify individual VOC biomarkers at a molecular level. Other limitations include the inability to correct for the influence of various exogenous factors and unmeasured confounding variables that could have influenced VOC patterns. Furthermore, sensor drift over time, although adjusted for in data analysis, may cause reproducibility issues.24 Future studies should focus on standardisation of all phases of VOC analysis based on characteristics most optimal for screening purposes, including optimisation of sensor arrays most sensitive to detect BO-specific VOCs, sampling protocols, and data analysis adjusted for technical and (patho)physiological confounders.25 Despite the promising results of this cross-validated training model, it is important to bear in mind that future research is needed to externally validate the diagnostic accuracy on independent patient cohorts that have not been previously exposed to the artificial neural network. Hence, a large external validation study is currently ongoing to test the developed training model on new patients and to assess reproducibility and intra-individual variation of breath prints. Finally, the case–control setting of this study makes it possible to obtain accurate test accuracy data but has limitations regarding generalisability to a primary care population consulting for GORD symptoms. Therefore, a multi-site validation study of breath testing for patients with chronic GORD symptoms in primary care is in preparation.
In conclusion, this portable electronic nose is able to detect the presence or absence of BO in patients with and without GORD with good diagnostic accuracy. Given the high tolerability, high acceptability and low costs, breath testing may be a promising approach to be used for non-invasive screening for BO in a primary care setting.
References
Footnotes
Contributors YP: study concept and design, patient inclusion, data acquisition, quality control of data and algorithms, data analysis and interpretation, statistical analysis, manuscript preparation, editing, and review; RWMS: contributed to study design, patient inclusion, data acquisition, critical revision of the manuscript. AT: contributed to study design, patient inclusion, data acquisition, critical revision of the manuscript. SKB: contributed to study design, patient inclusion, data acquisition, critical revision of the manuscript. BdJ: contributed to study design, patient inclusion, data acquisition, critical revision of the manuscript. PDS: study concept and design, data interpretation, manuscript editing, and review, study supervision.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors. The four Aeonose devices were supplied by the eNose Company (Zutphen, the Netherlands) at no costs.
Competing interests The Aeonose™ devices are provided by the eNose Company (Zutphen, the Netherlands) for use in research. No additional funding for this study was received and all research was investigator initiated.
Patient consent for publication Not required.
Ethics approval The study protocol was approved by the research ethics committee of the Radboud University Nijmegen Medical Centre, the Netherlands, and thereafter by all local ethics committees of the participating centres. This study was performed in compliance with the Declaration of Helsinki and registered at the Netherlands Trial Register (Identifier NL6750 (NTR6928)).
Provenance and peer review Not commissioned; externally peer reviewed.