Article Text

Abstract
Background The gold-standard treatment for acute exacerbation of chronic obstructive pulmonary disease (ae-COPD) is non-invasive ventilation (NIV). However, NIV failures may be observed, and invasive mechanical ventilation (IMV) is required. Extracorporeal CO₂ removal (ECCO₂R) devices can be an alternative to intubation. The aim of the study was to assess ECCO₂R effectiveness and safety.
Methods Patients with consecutive ae-COPD who experienced NIV failure were retrospectively assessed over two periods of time: before and after ECCO₂R device implementation in our ICU in 2015 (Xenios AG).
Results Both groups (ECCO₂R: n=26, control group: n=25) were comparable at baseline, except for BMI, which was significantly higher in the ECCO₂R group (30 kg/m² vs 25 kg/m²). pH and PaCO₂ significantly improved in both groups. The mean time on ECCO₂R was 5.4 days versus 27 days for IMV in the control group. Four patients required IMV in the ECCO₂R group, of whom three received IMV after ECCO₂R weaning. Seven major bleeding events were observed with ECCO₂R, but only three led to premature discontinuation of ECCO₂R. Eight cases of ventilator-associated pneumonia were observed in the control group. Mean time spent in the ICU and mean hospital stay in the ECCO₂R and control groups were, respectively, 18 vs 30 days, 29 vs 49 days, and the 90-day mortality rates were 15% vs 28%.
Conclusions ECCO₂R was associated with significant improvement of pH and PaCO₂ in patients with ae-COPD failing NIV therapy. It also led to avoiding intubation in 85% of cases, with low complication rates.
Trial registration number ClinicalTrials.gov, NCT04882410. Date of registration 12 May 2021, retrospectively registered.
- COPD exacerbations
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
The key question: extracorporeal CO₂ removal (ECCO₂R) effectiveness and safety
We observed a much better clinical response compared with previous studies, leading to avoiding intubation in 85% of cases despite including severe patients with chronic obstructive pulmonary disease (COPD), some of them receiving long-term oxygen therapy or NIV at home (which were excluded in previous studies). Indeed, only four patients of the ECCO2R group had to be intubated. For all but one, intubation occurred after ECCO2R weaning.
We observed a much lower rate of major bleeding complications compared with previous studies. Just over 20% of patients with ECCO₂R (six patients) experienced significant bleeding complications and only three led to premature discontinuation of ECCO₂R (despite patients being obese and thus more difficult to cannulate). In the ÉCLAIR study (by Braune et al15), 11 major bleeding events occurred among the 25 patients treated with the same ECCO2R device.
Good results and low complication rate are likely to revive the discussion about the role of ECCO2R in the therapeutic arsenal of COPD acute decompensation.
Background
Chronic obstructive pulmonary disease (COPD) is a frequent pathology. It is commonly complicated by acute exacerbations (ae-COPD), which are associated with a significant increase in mortality.1
Independently of the aetiologic treatment of exacerbations, non-invasive ventilation (NIV) has significantly improved the prognosis of these exacerbations. Nevertheless, nearly 20% of NIV-treated patients require invasive mechanical ventilation (IMV).2 3 IMV initiation is unquestionably considered a failure and is associated with significant mortality,4 5 particularly due to ventilator-associated pneumonia.6
The extracorporeal CO2 removal (ECCO2R) device eliminates a portion of CO2 through extracorporeal circulation but cannot oxygenate the blood because of the low flow system. Advances in technology and a better knowledge of the technique have enabled its use in patients with ae-COPD.7 Combined with NIV, the use of ECCO2R in patients with ae-COPD may enhance CO2 removal effectiveness, lowering the respiratory rate and, thus, minimising dynamic hyperinflation and intrinsic positive end-expiratory pressure (PEEP). Thus, work of breathing can be reduced and CO2 production from respiratory muscles lowered.8 The absence of sedation allows patients to receive active physiotherapy preventing muscle deconditioning.
Two potential benefits for patients with ae-COPD are currently being investigated, that is, to avoid the use of IMV in case of NIV failure and to facilitate IMV weaning.9–12 Studies assessing ECCO2R in patients with ae-COPD are scarce and all had a small study sample.
Besides potential benefits, ECCO2R is associated with adverse effects. This technique requires inserting intravascular cannulas and administering anticoagulant therapy, which expose patients to major bleeding risks. A benefit-risk approach is, therefore, necessary before offering this treatment on a larger scale.
The study objective was to confirm the effectiveness of this technique in a selected population of patients with COPD for whom NIV proved insufficient to improve clinical condition (both alveolar ventilation and work of breathing). The primary endpoint was to record ECCO2R failure (IMV or death by day 90). Secondary endpoints were effectiveness, safety and observational data.
Methods
Study design
We performed an observational, single centre (Centre Hospitalier de Saint-Denis, Saint-Denis, France), retrospective study. Successive patients with ae-COPD with NIV failure were assessed over two periods of time: before and after ECCO2R device implementation.
Criteria used to include patients in both groups were: no improvement or worsening of respiratory acidosis after NIV treatment, and no improvement of respiratory distress signs or decreased level of consciousness. Exclusion criteria were severe hypoxaemia (FIO2 >40% for an oxygen saturation ≥90% with NIV), contraindications to anticoagulant therapy, contraindications to continuation of active treatment for reasons of futility.
In the control group, intubation criteria were the same as the inclusion criteria mentioned above for defining NIV failure. In the ECCO2R group, patients underwent intubation during/after ECCO2R treatment using the same criteria to which we added agitation potentially leading to self-inflicted dislocation of ECCO2R cannulas, deteriorating neurological status with loss of airway protective reflexes, development of unmanageable copious pulmonary secretions or progressive hypoxemia.
From January 2010 to February 2015—before implementation of the ECCO2R device in the ward—67 of 206 patients with ae-COPD required invasive ventilatory support. After applying the exclusion criteria, 25 patients were included in the control group (figure 1). From February 2015 to February 2020, 32 of 354 patients with ae-COPD were treated with ECCO2R (without invasive ventilation weaning). After applying the exclusion criteria, 26 patients were included in the ECCO2R group (figure 1).

Flow chart. Ae-COPD, acute exacerbation of chronic obstructive pulmonary disease; DNR, do not resuscitate order; ECCO2R, extracorporeal CO2 removal; NIV, non-invasive ventilation.
NIV management
NIV was performed with Respironics V60 Ventilator (Philips Respironics: USA) in S/T mode, as recommended in our unit protocol: the pressure support was increased by 2 cmH2O steps depending on the patient’s tolerance, up to a maximum of 20 cmH2O to reach a tidal volume of 8 mL/kg of ideal body weight. The expiratory positive airway pressure was between 5 cmH2O and 10 cmH2O. The FiO2 was adapted to reach an oxygen saturation of 90%–92%. The interface was a full-face mask (PerformaTrak, Philips Respironics).
ECCO2R device
ECCO2R was performed with the Xenios console, iLA active iLA kit (Xenios AG, Heilbronn, Germany). The membrane used for every patient had a gas exchange area of 1.3 m2. Anticoagulant therapy was maintained with continuous intravenous unfractionated heparin with anti-Xa monitoring. The anticoagulant therapy target was 0.3 IU anti-Xa/mL. Most patients had femoral cannulation with Novaport twin 24 Fr (on the right side, except for one patient). Only two patients had jugular cannulation (18 and 22 Fr). Targeted blood flow through the circuit was 1 L/min. Initiation of ECCO2R was medically and collectively decided, and cannulation was performed by a medical doctor.
IMV and sedation management
A protocol was developed for the ventilation weaning strategy and the sedation withdrawal strategy. Sedation was systematically adjusted by the nursing staff to ensure the patients’ comfort and safety according to the ward’s protocol, using the Richmond agitation sedation scale (RASS) score. As for weaning from mechanical ventilation and according to pre-established criteria, pressure support was reduced until patients were considered ready for extubation.
Data collection
Data collected (patient characteristics, arterial blood gas, report of ECCO2R adverse effects, outcomes, and duration) during the two periods (before and after ECCO₂R device implementation in the ward) were extracted from each patient’s electronic health record. A first request including the inclusion criteria allowed identification of each patient. Data were then exported to a single anonymised datasheet from the various databases containing texts, treatments, biological results and various dates to calculate duration of hospitalisation, etc. Analyses were then carried out using this material.
Blood gas tests were performed at various time points: 6 hours before intervention (ECCO2R or endotracheal intubation), 2 hours before intervention, 6 hours after intervention, 24 hours after intervention and before decannulation or extubation. Major bleedings were defined by fatal bleeding or symptomatic bleeding in a critical site or fall in haemoglobin level of more than 2 g/dL or bleeding leading to transfusion of two or more units of packed red blood cells.13 Thrombocytopenia was defined by a blood platelet count below 100 G/L with more than half of the baseline count. Haemodynamic instability was defined by the need for catecholamine administration.
Statistical analysis
The R Studio software (V.1.2.1335 2009–2019 RStudio) was used for analyses. Variables are reported as mean±SD for quantitative data and number (percentage) for categorical data. Population distribution was tested with the Shapiro-Wilk normality test. Quantitative variables were compared with t test or paired t test with a 95% CI and with Welch’s two-sample t test when the two populations had unequal variances. As one of the variables was not following a normal distribution, we used Wilcoxon rank sum test with continuity correction. Qualitative variables were compared with Pearson’s χ2 test, with or without Yates’ continuity correction, depending on the theoretical distribution of variables. The analyses were conducted at a two-sided alpha level of 5%.
Patient and public involvement
Patients with ae-COPD experiencing NIV failure require mechanical ventilation, preventing them from talking and moving. One of our motivations was to find an alternative for them to regain some autonomy during the hospital stay.
We performed a non-randomised study with a before/after design. Patients were not involved in the study design, neither were they involved in the recruitment or conduct of the study.
The study results will be disseminated to study participants on request, in accordance with French law. They will also be published on the hospital website.
Ethics
Individual patient information, collective information within the facility, opposition possibility and a data protection strategy were, thus, required. Patients were informed by individual letters of the use of their anonymous data, with the possibility to object to their participation in the study.
The database was declared to the French Data Protection Authority (CNIL, ‘Commission nationale de l’informatique et des libertés’). Data processing was conducted on an anonymised datasheet.
Results
Patient characteristics
Patients were mostly men (72%) with a mean±SD age of 69±11 years. Both groups (ECCO2R group: n=26, IMV group: n=25) were comparable at baseline, except for BMI, which was significantly higher in the ECCO2R group (30 kg/m² vs 25 kg/m²) (table 1). Comorbidities were similar in both groups (hypertension, diabetes, heart failure, coronary heart disease, atrial fibrillation, stroke). In the ECCO2R group, 11 (42%) and 7 (27%) patients, respectively, received long-term oxygen therapy (LTOT) and NIV prior to hospitalisation. No significant difference was observed compared with the IMV group. Four patients (15%) had an exacerbation related to influenza in the ECCO2R group, whereas none of them in the IMV group.
Baseline patient characteristics
Arterial blood gas tests (pH, PaCO2, PaO2 and HCO3-) carried out 6 hours before intervention did not differ between both groups. All patients had pH <7.35 and PaCO2 >45 mm Hg. In the ECCO2R group, 19 patients (73%) had a PaCO2 ˃ 75 mm Hg and 15 patients (58%) had a pH <7.25 before intervention.
Main objective
The primary endpoint was to record ECCO2R failure (IMV or death) by day 90. Five patients (19%) experienced ECCO2R failure: four patients (15%) were intubated in the ECCO2R group, among whom, three patients were no longer alive at day 90. One patient died without being intubated due to multiple organ failure.
Among these four patients requiring IMV, intubation occurred after ECCO2R weaning due to recurrent hypercapnia for three of them. Only one patient required IMV during the ECCO2R procedure, due to a haemothorax (jugular cannulation). Duration between ECCO2R weaning and IMV was 3,2±4 days (mean).
Four patients (15%) died by day 90 in the ECCO2R group compared with seven patients (28%) in the IMV group. For two patients of the ECCO2R group, death occurred after ICU discharge (table 2) (figures 2 and 3).
Main objective
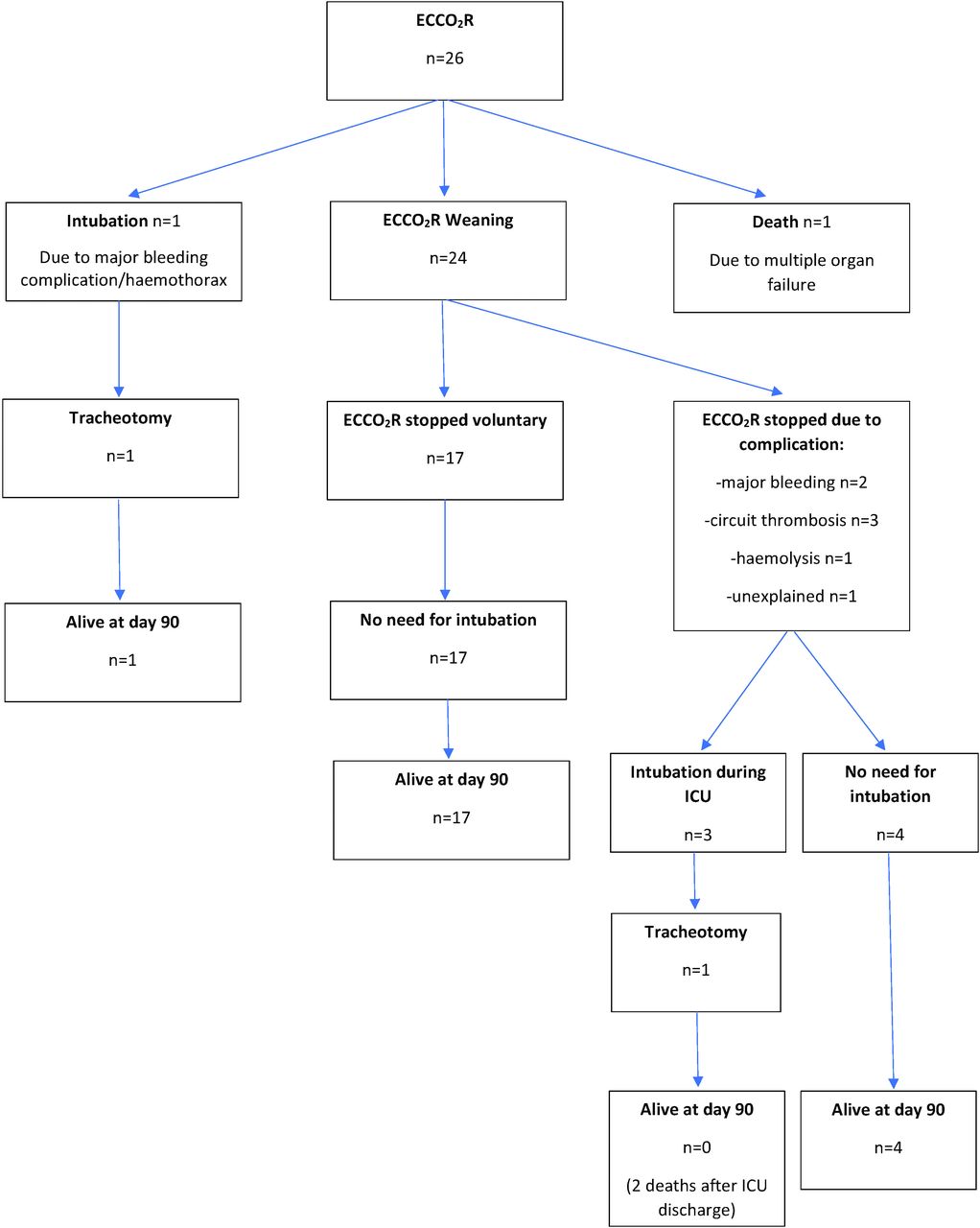
ECCO2R group outcomes. ECCO2R, extracorporeal CO2 removal; ICU, intensive care unit.

IMV group outcomes. IMV, invasive mechanical ventilation; N/A, non-available; VAP, ventilator-associated pneumonia. *With catecholamine administration required.
Effectiveness
pH and PaCO2 values quickly improved in both groups without any significant difference between them (figure 4).
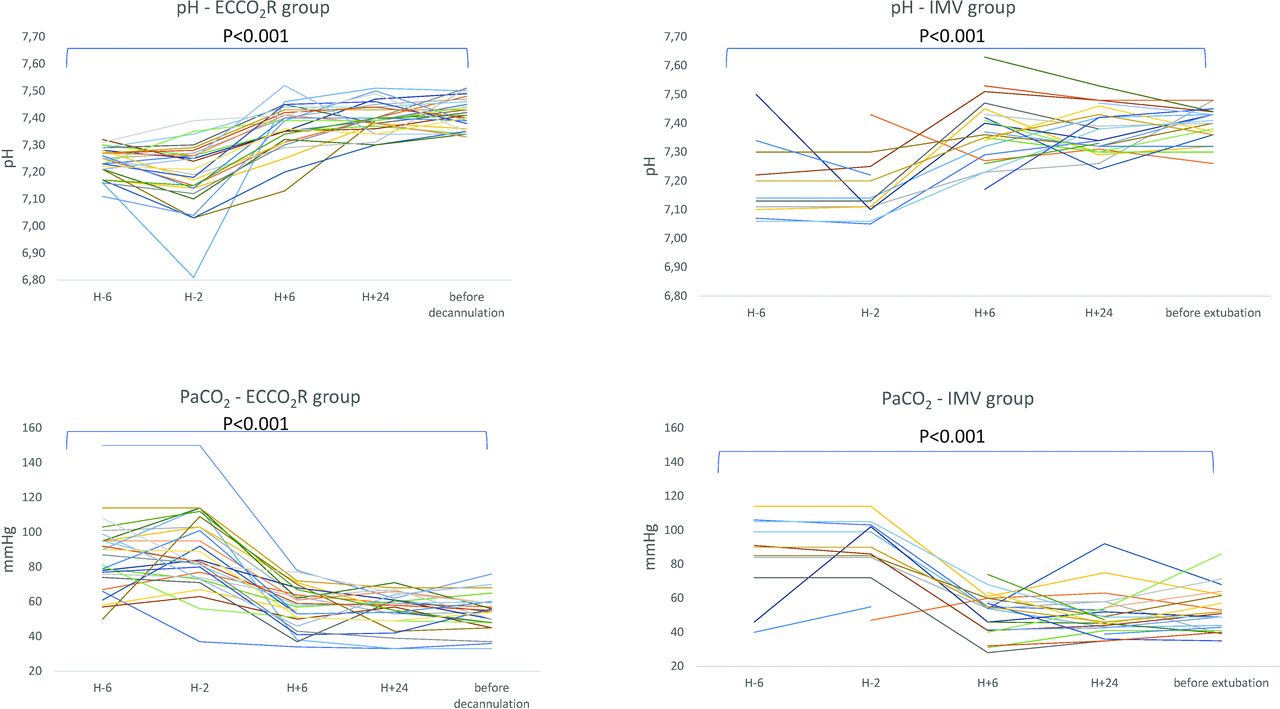
Evolution of pH and carbon dioxide arterial pressure (PaCO2) from 6 hours before cannulation or intubation until before weaning. ECCO2R, extracorporeal CO2 removal; IMV, invasive mechanical ventilation.
The pH value was significantly lower 6 hours before ECCO2R (7.24±0.05) compared with time of decannulation (7.41±0.06) (p<0.001). Likewise, the PaCO2 value 6 hours before ECCO2R was significantly higher (86±21 mm Hg) than at the time of decannulation (53±10 mm Hg) (p<0.001). In the IMV group, the mean arterial blood pH value 6 hours before intubation was 7.23±0.13 and increased to 7.39±0.06 before extubation (p<0.001). The mean PaCO2 value 6 hours before IMV was 82±24 mm Hg and decreased to 52±13 mm Hg before extubation (p<0.001).
The ICU length of stay in the ECCO2R group was 18±14 days compared with 30±43 days in the IMV group. The length of hospital stay was 29±22 days in the ECCO2R group compared with 49±53 days in the IMV group. No significant difference was identified for these parameters, nor for the 28-day or 90-day mortality. The 90-day mortality rate was, respectively, 15% and 28% in the ECCO2R and IMV groups (table 3).
Effectiveness
Safety
Complications in the ECCO2R group
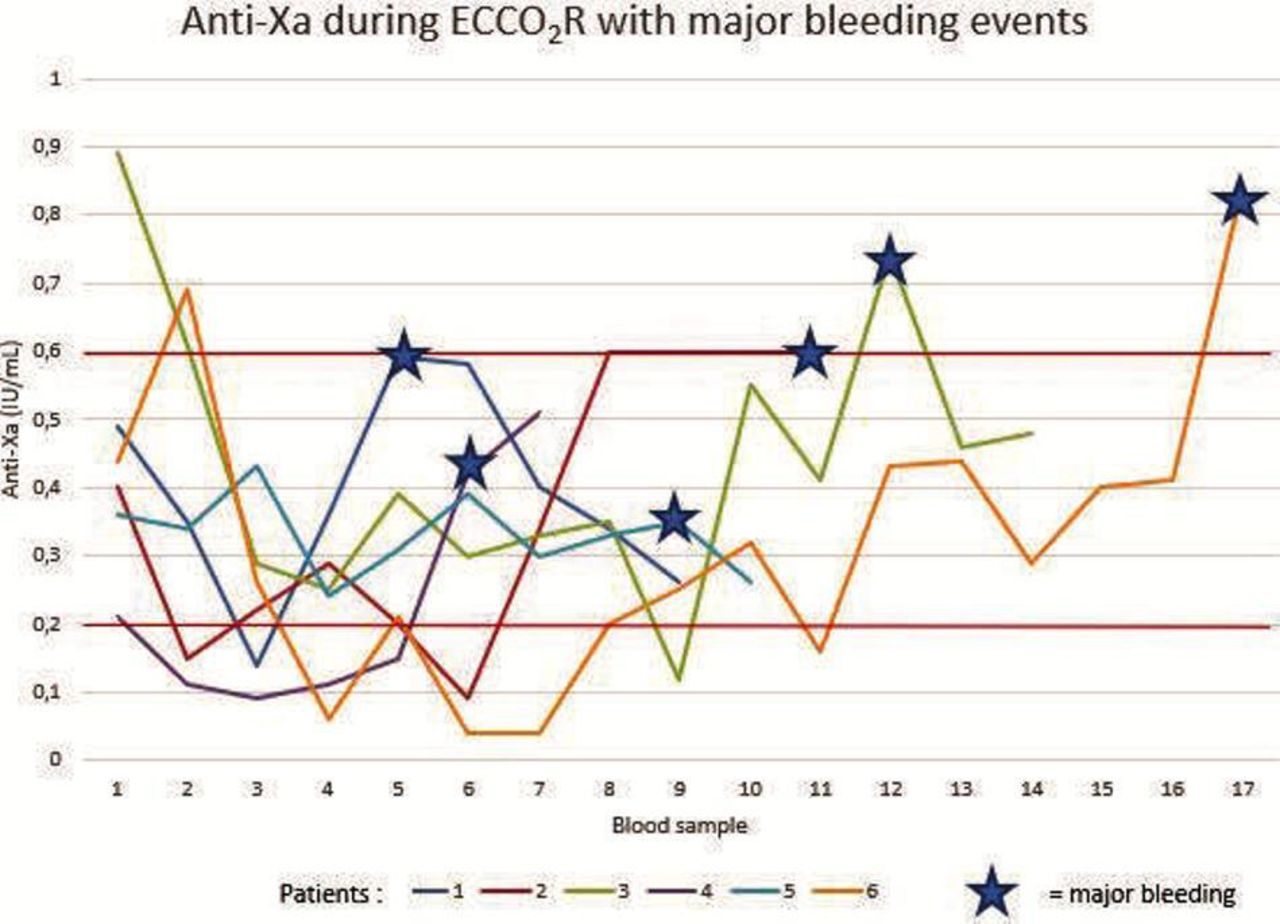
Seven major bleeding events occurred in six patients (23%) of the ECCO2R group.
ECCO2R was discontinued due to bleeding for 11% of patients (three patients): one patient underwent haemorrhagic shock and respiratory distress due to haemothorax during jugular cannula insertion (18 French) complicated by cardiac arrest requiring emergency intubation (the patient was still alive at day 90); another patient experienced recurrent bleeding at the cannula insertion femoral site with rectus abdominis muscle haematoma; the remaining patient had an haematoma of the right pectoral muscle (jugular insertion 22 French cannula). Of seven major bleeding events, four occurred with anti-Xa ≥0.60 IU/mL (figure 5). There were six minor bleeding episodes (minor Scarpa’s fascia bleeding, epistaxis, haematuria) in five patients (20%). No cerebral or digestive bleeding event was observed (table 4).
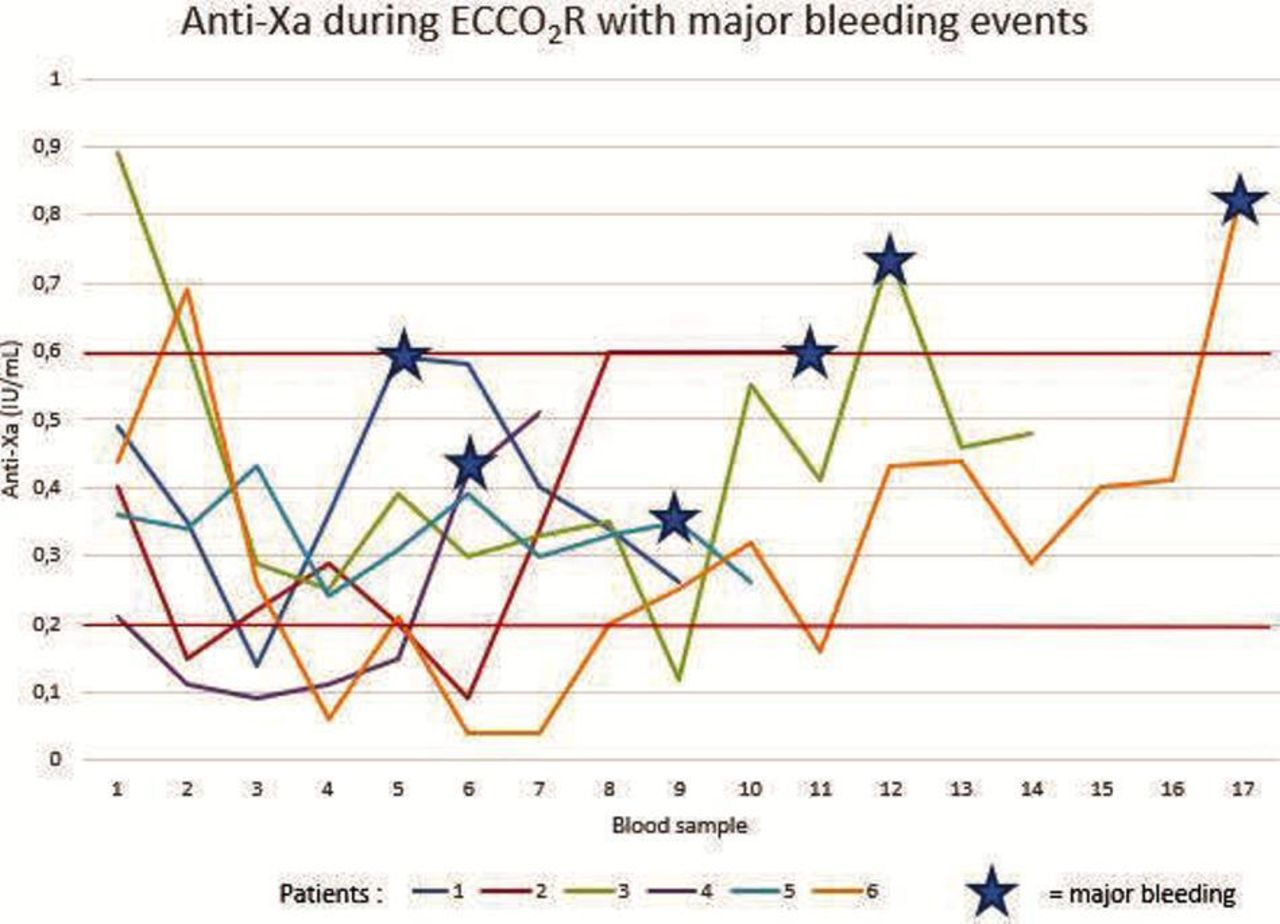
Anti-Xa in ECCO2 patients with major bleeding events.
ECCO2R-associated adverse effects
Three patients (11%) had haemolysis due to ECCO2R. Six patients had thrombocytopenia <100 G/L. Three cases of circuit thrombosis were observed, all leading to premature discontinuation of ECCO2R. They occurred at 4.8 days (mean) of ECCO2R. One of these patients never received the adequate dosing (under dosed) (figure 6). Anti-Xa control was usually performed two times a day.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Anti-Xa in ECCO2R patients with circuit thrombosis event.
No patient of the ECCO2R group developed pneumonia.
Complications in the IMV group
Eight patients (32%) experienced ventilator associated pneumonia (VAP). Most of these cases were late pneumonia. Twenty-five haemodynamic instability events with catecholamine administration requirement occurred in 19 patients (76%). Self-extubation was observed in six patients: all but one required reintubation (table 5).
IMV-associated adverse effects
Three patients (12%) died due to IMV-related complications: one patient had a pneumomediastinum following reintubation (self-extubation) consequently to a high intrinsic PEEP; another patient was discovered disconnected from the respiratory device; the remaining patient died due to haemorrhagic shock and respiratory distress after tracheotomy-related massive bleeding.
Observational data
Therapy initiation (IMV or ECCO2R) seems to have been started earlier in the IMV group than in the ECCO2R group: respectively 20±35 hours and 42±69 hours from NIV initiation (p=0.15).
Thirteen (50%) cannulations were performed during the night shift (between 19:00 and 08:00).
NIV was continued for 18 patients (69%) of the ECCO2R group. Nine patients (35%) had high-flow nasal oxygen therapy during ECCO2R treatment because of mild hypoxemia.
ECCO2R and IMV interventions lasted 5.4±4 and 27±43 days (p=0.019), respectively. Seven patients (28%) required neuromuscular blocking agent after intubation because of high intrinsic PEEP. The rate of tracheotomy in the IMV group was 20% (five patients) and 8% (two patients) in the ECCO2R group (table 6).
Observational data
Discussion
This study has numerous limitations. It is a retrospective, monocentric and observational study. The before/after design of the study and the extended study period may also have altered the results. However, treatments were protocolised, thus minimising the impact on our results. International recommendations on NIV, invasive ventilation and sedation were followed. These strategies are likely to homogenise the historical group of patients treated with IMV. In addition, analysed data are mostly objective numerical data that are not affected by the retrospective design. Finally, we aimed to document the feasibility of ECCO2R and not to compare ECCO2R with IMV, which is associated with different adverse effects and for which we already know the consequences in patients with COPD.
Numerous spirometric data are missing to acquire better knowledge of our population because most patients were managed outside the hospital. However, most of them suffered from long-term illness and had full insurance coverage, which requires a diagnosis based on spirometric data because of their oxygen or NIV home need.
This ECCO2R device is associated with significant improvement of pH and PaCO2 values in patients with ae-COPD (figure 1). However, the objective was not to normalise arterial blood gases, which can be deleterious, but to achieve both an improvement in alveolar ventilation and in work of breathing. Some very low-flow systems may not be able to remove sufficient CO2 to significantly improve the respiratory rate and intrinsic PEEP.14 Due to the retrospective design of the study, we could not collect information about pulmonary mechanics evolution such as the respiratory rate or the oesophageal pressure, which reflect inspiratory work. Gasometric improvement was comparable to that produced by IMV.
IMV was avoided in 85% of patients treated with ECCO2R (15% of ECCO2R patients had to be intubated). This result is very encouraging given that our patients were highly severe patients with COPD with, for many of them, LTOT or NIV at home (which were excluded in the ÉCLAIR study by Braune et al15). All but one ECCO2R failures were due to recurrent hypercapnia occurring after a premature discontinuation of ECCO₂R due to a complication, suggesting that decannulation was performed too early. The only intubation performed during ECCO2R was due to cardiac arrest caused by jugular cannulation complicated by haemothorax.
Caution should be exercised with hypoxemic patients, in whom ECCO2R failure seems to be more frequent in other studies.15 16 The ÉCLAIR study reported 11 patients (44%) requiring intubation in the ECCO2R group, including seven for hypoxemia. More than 90% of intubation cases reported in the ÉCLAIR study occurred during the ECCO2R treatment. Indeed, during spontaneous ventilation, excessive CO2 removal leads to a decrease in the tidal volume with increased risk of atelectasis and decrease in alveolar PO2.17
Although we used the same definition for major bleeding13 and despite our ECCO2R group patients being more obese with associated difficulties in cannulation, just over 20% of our ECCO2R patients experienced significant bleeding complications while 36% (nine patients) or 11 major bleeding events occurred in the ÉCLAIR study.15 The ÉCLAIR study may have made a higher use of jugular cannulation than we did. As patients with jugular cannulation experienced serious haemorrhagic and pulmonary complications, we should further study the site of cannulation in these patients who often present with significant pulmonary hypertension and emphysema. Furthermore, jugular cannulation requires patients to be placed in supine position while experiencing respiratory distress. Based on our acquired expertise, we stopped cannulating in jugular sites. We also learnt to target the low anti-Xa range although all major bleeding events do not occur because of heparin overdose. Other factors are probably involved in these phenomena.18
Despite a low anti-Xa target, we only observed three cases of circuit thrombosis. They all led to premature discontinuation of ECCO2R but only one patient required IMV. We did not measure plasma-free haemoglobin nor did we notice urine coloration, which can help to anticipate this complication.19 Other studies reported rates of nearly 25%.20 The higher mean blood flow throughout the circuit, therefore, seems to play a role in decreasing the circuit thrombosis occurrence. This complication, together with bleeding issue, highlights the importance of an anticoagulant strategy and of trained staff.
Conclusion
This study reveals that ae-COPD patients with NIV failure could be treated with ECCO2R. Findings show that intubation can be avoided, especially in the absence of significant hypoxemia. However, it is important to consider the adverse effects of ECCO2R treatment, especially haemorrhagic complications. Such treatment requires constant monitoring and team training. It is, therefore, important to identify the subset of patients and, when in the disease course, patients could most benefit from this technique. Finally, this article also raises the question of the optimal time of ECCO2R weaning. Prospective randomised studies are required. Technical progress may facilitate the management of this emerging technique in the near future.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
In accordance with the French legislation, the study was approved by the local hospital ethics committee of Saint-Denis Hospital, Institutional Review Board IRB00012591 (IRB/T0004).
Acknowledgments
We sincerely thank patients for their participation in this study.
References
Footnotes
Contributors MA: patient management, data acquisition, data analysis, writing, proofreading of the article and guarantor. JA: writing, proofreading. SA, DU, LF, VI, NM, TI, ML and LL: patient management and proofreading. RS: team training, proofreading. DS: coordination, study design, patient management, writing and proofreading. All authors have read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests Rita Serbouti, from Fresenius Medical Care France, Medical affairs, helped train staff in Extracorporeal CO2 Removal Device and contributed to proofreading this paper. No financial support from the industry was received.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.