Article Text

Abstract
Objective We evaluated agreement in diagnoses for bacterial vaginosis (BV), Trichomonas vaginalis (TV) and vulvovaginal candidiasis (VVC) between clinicians examining the patient and performing diagnostic tests versus a clinician with access only to the patient's history and diagnostic findings from self-obtained vaginal swabs (SOVS).
Design Women presenting with vaginal discharge to a sexually transmitted infections clinic provided SOVS for evaluation and completed the study and qualitative questionnaires. A clinician then obtained a history and performed speculum and bimanual examinations. Participants’ history and diagnostic test results from SOVS were provided to a masked non-examining clinician who rendered independent diagnoses. Overall agreement in diagnoses and κ statistics was calculated.
Results The prevalence of infections among the 197 participants was 63.4% (BV), 19% (TV) and 14% (VVC). The per cent agreement between the examining and non-examining clinician for the diagnoses of BV was 68.5%, 90.9% for TV and 91.9% for VVC. Of the 105 women diagnosed with BV by the examining clinician, 34 (32%) were missed by the non-examining clinician. The non-examining clinician missed 13 (48%) of 27 women and 12 (34%) of 35 women treated for VVC and TV, respectively. Four women who all presented with abdominal pain were diagnosed with pelvic inflammatory disease.
Conclusions Tests from SOVS and history alone cannot be used to adequately diagnose BV, TV and VVC in women presenting with symptomatic vaginal discharge. Cost benefits from eliminating the speculum examination and using only tests from SOVS may be negated by long-term costs of mistreatment.
- Vaginal Discharge
- Women
- Bacterial Vaginosis
- Candida
- Diagnosis
Statistics from Altmetric.com
Introduction
Symptomatic vaginal discharge is a common gynaecological complaint.1 Current clinical practice includes a speculum examination (SE) for evaluating the discharge. The clinician inspects the external genitalia, vagina and cervix; assesses characteristics of the discharge; notes physical signs such as inflammation and lesions; and collects specimens for laboratory testing. Many clinicians also perform a bimanual examination. The SE requires time, supplies and a trained clinician. Additionally, discomfort of a pelvic exam may lead women to delay or avoid seeking care.2–4 Developing accurate approaches to diagnosing lower genital infections without a SE would be advantageous to both clinicians and patients.
Highly sensitive and specific nucleic acid amplification tests (NAATs) have been developed for the detection of Neisseria gonorrhoeae (GC), Chlamydia trachomatis (CT) and Trichomonas vaginalis (TV). NAATs are superior to conventional tests.5 ,6 Novel methods of obtaining and testing pelvic specimens have been developed and validated.7 ,8 Studies demonstrate the comparability of self-obtained vaginal swabs (SOVS) and provider obtained specimens.9 ,10 Patient-inserted tampons, first void urine collection, and self-obtained vaginal, introital, vulvar or perineal swabs have all performed better than provider obtained tests in the detection of CT, GC and TV.5 ,6 ,11 ,12 These tests could change the way clinicians diagnose abnormal vaginal discharge.
A previous study showed that elimination of SE in women presenting to a sexually transmitted infections (STI) clinic resulted in few missed serious diagnoses using NAATs to detect GC, CT and TV and standard serological tests for syphilis and HIV.13 The goal of this study was to determine if SE could be eliminated in the evaluation of vaginitis syndromes (bacterial vaginosis (BV), TV and vulvovaginal candidiasis (VVC)). Specifically, we aimed to assess the accuracy of history alone and SOVS in establishing the correct diagnosis in women presenting with symptomatic vaginal discharge. We also sought to determine if eliminating the SE would lead to significant missed diagnoses.
Methods
Study design
In this prospective cross-sectional study, diagnoses of common vaginal infections (TV, BV, VVC) made by SOVS were compared with diagnoses made by the combination of clinician obtained swabs (COS) and SE.
Study population
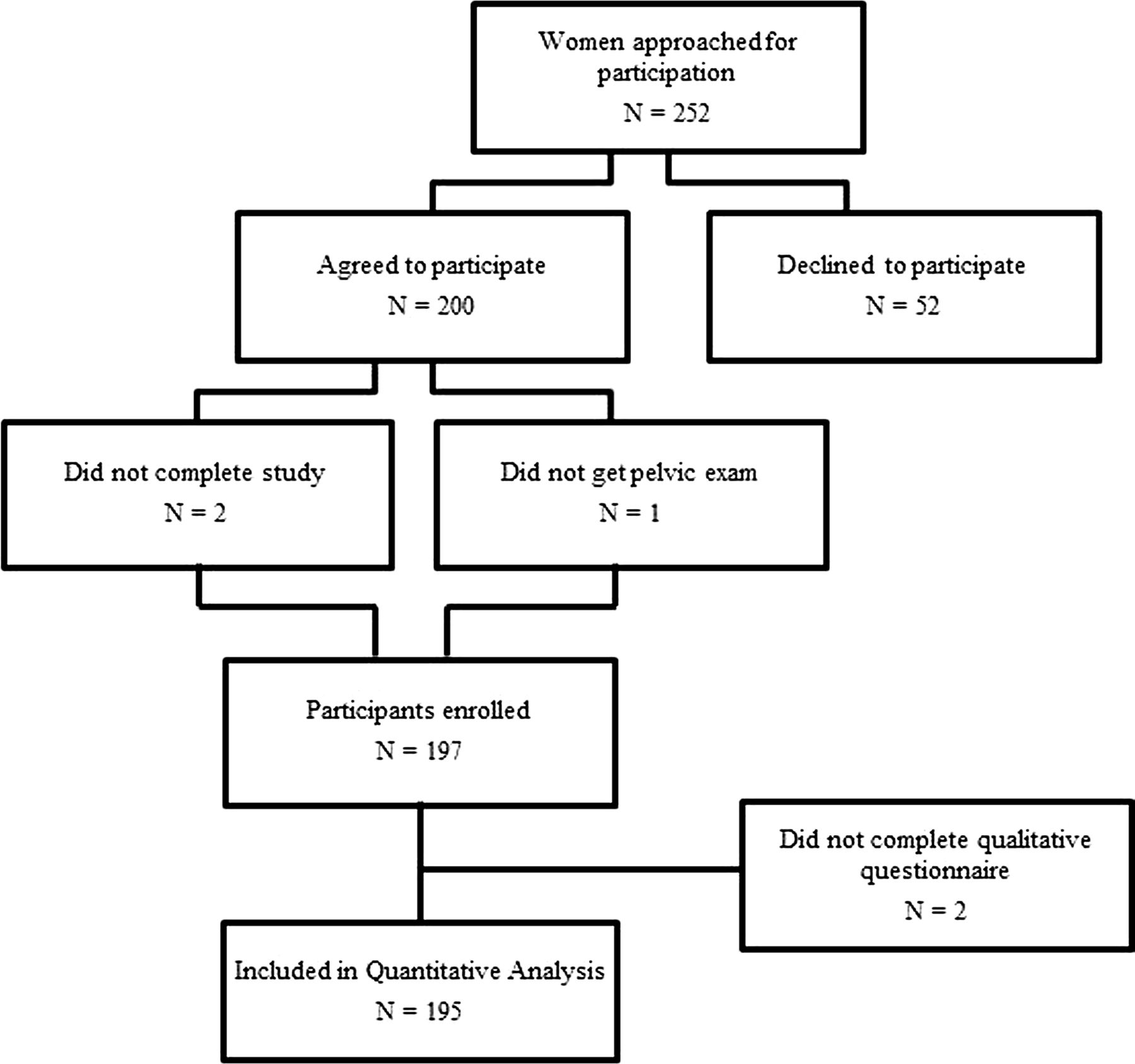
Women ages 18–45 years presenting with symptoms of abnormal vaginal discharge were recruited from an STI clinic in Baltimore, Maryland, USA, from March 2005 to August 2006 (figure 1). Exclusion criteria included abnormal vaginal bleeding, pregnancy and evaluation in the preceding 30 days for similar symptoms. Participants who met inclusion criteria and agreed to participate received a $10 gift card. All participants provided written informed consent. The institutional review boards of the Johns Hopkins Medical Institutions and the public health committee of Baltimore City Health Department approved this study.

{kind=link}
Flow chart for patient recruitment.
Data collection and laboratory methods
Participants completed a self-administered written questionnaire including information on demographics, medical, reproductive, contraceptive and sexual history and current vaginal discharge symptoms (table 1). After detailed instructions, each participant provided three SOVS. Each swab was inserted up to two inches into the vagina, rotated several times to sample the vaginal fluid and placed in its sterile container. The study recruiter collected the questionnaire and SOVS from the participants after unobserved sampling and processed the specimens according to the study protocol.
Self-obtained vaginal swabs
Testing for SOVS including pH, preparation and interpretation of slides for microscopy of vaginal secretions in saline and 20% potassium hydroxide (KOH) and an amine odour (‘Whiff’) test was completed by the onsite laboratory technician using one swab. A second swab was used to prepare a dry slide for Gram staining, which was stored with the third swab for testing for GC, CT and TV.
Using Nugent's system,14 Gram stains are scored from 0 to 10 and assigned to one of three categories: normal (0–3), intermediate (4–6) and positive (7–10) for BV. Slides with a score of 7–10 were classified as positive for BV while 0–6 were classified as negative. The remaining SOVS and dry slide were collected twice a week and transported to an off-site laboratory for processing. GC and CT were tested by a US Food and Drug Administration approved strand displacement amplification assay (BDProbe Tec, Becton Dickenson (Franklin Lakes, New Jersey, USA). TV was tested from the same swab by research polymerase chain amplification (PCR) method in routine use at the Johns Hopkins University International STI laboratory.15 ,16 Testing was completed in weekly batches and all positive results were immediately distributed to clinicians.
Routine clinical assessment
After providing the SOVS, participants were evaluated and managed according to clinic protocol which included pertinent history, physical examination, laboratory testing, treatment and referrals as needed. The physical examination included evaluation of the vulva/vagina, SE with collection of vaginal/cervical specimens and a bimanual examination. Standard laboratory evaluation for COS included point of care (POC) and delayed testing. POC testing included a vaginal swab used for pH determination and microscopy with saline and KOH slides and Whiff test for BV, VVC and TV diagnosis; and an endocervical Gram stain for the presence of inflammation and/or Gram-negative diplococci. Diagnosis of BV was based on Amsel's Criteria.17 TV required visualisation of the pathogen on wet mount. Centers for Disease Control and Prevention (CDC, 2010) define VVC diagnosis as based on vaginal discharge, irritation/pruritus, vulvovaginal oedema or erythema, pH and identification of yeast on KOH microscopy. Delayed testing consisted of an additional endocervical swab for GC culture and CT NAATs (Amplicor; Roche Molecular, Indianapolis, Indiana, USA). Women were treated based on the results of the POC testing. If the endocervical Gram stain demonstrated inflammation alone, the woman was presumptively treated for CT; if both inflammation and Gram-negative intracellular diplococci were present, she was treated for GC and CT. Delayed test results were assessed 48–72 h later; if a diagnosis of GC or CT was missed on the initial POC testing, the woman was appropriately treated. Furthermore, if testing for pathogens from the SOVS was positive (eg, TV), the woman was treated if she had not already received medication.
Reference standards
Gram stained smears prepared from the SOVS served as the reference standard for BV. The reference standard for TV was based on the research PCR method from the SOVS.15 ,16 The diagnosis of VVC rendered by the examining clinician and based on 2010 CDC criteria18 served as the reference standard for VVC. Wet mounts prepared from SOVS were tested by experienced onsite laboratory technicians. The examining clinicians (N=4) at the STI clinic trained in microscopy prepared and interpreted their own saline and KOH slides.
Qualitative instrument
After completing the SE, participants completed a self-administered qualitative questionnaire to assess their experience with SOVS versus SE. Using visual analogue scales, participants scored questions about their comfort with obtaining their own specimens, discomfort or pain with SOVS and SE, and preference of SOVS versus SE for evaluation of vaginal discharge. On a scale of 0–10 cm the visual analogue scale scored from easy to difficult, no pain to a lot of pain, very comfortable to very uncomfortable and not important to very important. For comparisons between the SOVS and SE, the former was placed at 0 and the latter at 10.
Diagnoses of non-examining clinician
To identify the accuracy of SOVS, an infectious diseases clinician experienced in managing lower genital tract infections who did not examine the participants was asked to provide a diagnosis for TV, BV and VVC for each patient in the study based on history from the questionnaire and POC tests from the SOVS. This non-examining clinician diagnosed BV if participants were positive for at least two of three Amsel's criteria17 (pH>4.5, positive for clue cells>20% and Whiff test). TV was diagnosed by the presence of trichomonads on saline microscopy from SOVS. VVC was diagnosed based on the presence of yeast cells on wet mount, and the exclusion of other causes of vaginal discharge.
Statistical methods
Sample size calculation
Our prestudy estimate was that the per cent agreement between the diagnoses made by specimens collected by the SOVS and those collected by the COS would be 90%. The sample size of at least 138 women was based on per cent agreement between SOVS and clinician diagnoses of the common vaginal infections of BV, TV and VVC. This sample size allowed us to estimate the per cent agreement to within 5 percentage points with 95% confidence when the estimated agreement is 90% or greater (n=z21−α/2 (p0q0)/L2).
Data analyses
Per cent agreement for the diagnoses of BV, TV and VVC is presented between the examining and non-examining clinician (table 2) and between clinicians and the reference standard (table 3). McNemar's test for bias, κ statistics and interpretation of κ are also reported. The reference standards included the diagnosis of BV based on the Gram stain prepared from the SOVS, TV diagnosed by PCR from the SOVS and VVC diagnosis rendered by the examining clinician. Total diagnoses for BV, TV and VVC were calculated based on the reference standard.
Results
A total of 252 women were screened: 200 (79%) agreed to participate in the study; three were excluded for missing data; and 197 were included in the final quantitative analyses (figure 1). Two participants did not complete the visual analogue scales; 195 are included in the qualitative analysis. The mean age of participants was 28.1 years. The majority were African-American (95%), heterosexual (90%) and sexually active (92%). Overall, 38% of participants reported a new sexual partner in the last month and 97% reported at least one previously diagnosed vaginal infection (table 1). About 14% of women had tried over the counter treatments and 25% had tried douching for their symptoms before evaluation at the STI clinic. Overall, 17% of participants had no infection, 58% had one infection and 25% had two or more infections.
Demographic and clinical characteristics
The prevalence of infections based on the reference standards was 63.4% (BV), 19% (TV), 14% (VVC), 4% (GC) and 12% (CT) for the study population.
Examining clinician versus non-examining clinician
Of the 105 diagnoses of BV made by the examining clinician, the non-examining clinician diagnosed 61 (table 2). Concordant results with the examining clinician for the diagnosis of BV were reported in 68% of cases with a Cohen's κ of 0.39 for the non-examining clinician. Agreement was poor (κ=0.39±0.06) for the non-examining clinician.
Diagnoses by non-examining clinician based on self-obtained vaginal swabs (SOVS)* compared with examining clinician based on speculum examination (SE)
The examining clinician diagnosed TV in 35 women, and of those the non-examining clinician correctly identified only 23. There was good agreement between the two clinicians (κ=0.66±0.07) with no bias towards underdiagnosis or overdiagnosis.
Compared with the examining clinician diagnosis for VVC (N=27), the non-examining clinician identified 14 (51.8%) cases (table 2). The non-examining clinician showed a significant bias towards underdiagnosing VVC.
Reference standard versus clinicians
The Gram stain prepared from the SOVS identified 125 positive BV diagnoses compared with 90 (72%) by the examining clinician and 68 (54.4%) by the non-examining clinician. Both clinicians showed a statistically significant bias towards underdiagnosing BV compared with the Gram stain (table 3).
Diagnoses by clinicians compared with reference standard*
Compared with the reference standard that diagnosed 37 TV infections, the examining and non-examining clinicians correctly diagnosed 28 and 24 infections, respectively. Both clinicians had good agreement with the reference standard (table 3).
Based on the reference standard of gram stain for BV and NAAT for CT and TV, 21 (11.1%) participants had both BV and TV and 16 (8.5%) had BV and CT. In a subanalysis of these two groups of infections, there was no difference in the per cent agreement or accurate diagnosis by the non-examining and examining clinicians. Both fared poorly in identifying multiple concurrent infections.
Four participants were diagnosed with presumptive pelvic inflammatory disease and all presented with abdominal pain. Four were diagnosed with genital warts (2%) and less than 1% were diagnosed with pregnancy, herpes and syphilis.
When participants used a 10 cm visual analogue scale to rate difficulty and discomfort with SOVS, mean scores were 0.68 (±1.14) and 0.84 (±1.26). Women felt comfortable obtaining samples from themselves (1.71±2.04) and with the SE (2.94±3.03). Pain and discomfort with SE was greater than with SOVS (p<0.001). Most participants rated the SE as an important part of their assessment (8.14±2.22). Women indicated a strong preference for obtaining their own samples and preferred SOVS for future assessment of vaginal discharge. All responses were statistically significant (p<0.001) from the mid-point.
Discussion
This study showed that history and SOVS alone are not accurate in establishing the correct diagnosis for BV and VVC in women presenting with symptomatic vaginal discharge. SOVS are a convenient, efficient, and effective way to diagnose GC, CT and TV. Our study suggests, however, that bypassing the physical examination would result in misdiagnosing both VVC and BV. In addition, women with two or more infections would be inadequately diagnosed and treated. The study also confirmed the finding from our previous retrospective study that eliminating the SE would not lead to significant missed diagnoses.13
Compared with the reference standard for BV (Gram stain), both clinicians underdiagnosed BV. Even with Amsel's clinical criteria, the non-examining clinician showed a statistically significant bias towards underdiagnosing BV compared with the examining clinician. While the use of two instead of three Amsel's criteria to diagnose BV increased the number of participants diagnosed with BV, it also resulted in overtreatment of 25 infections.
Our findings contradict those of Gutman et al who showed that the clinical criteria for diagnosing BV can be reduced from three to two without loss of sensitivity and specificity; two criteria had a sensitivity of 61%–69% and a specificity of 86%–95%.19 In our study, the sensitivity and specificity of two criteria compared with the Gram stain were 42%–50% and 92%–97%, respectively. The differences may result from the study of different populations with different prevalence of BV or the use of slightly more sensitive pH cut-off. A modification to clinical criteria may be needed to accurately diagnose BV from SOVS or alternatively the Gram stain from SOVS could be used for diagnosis.
The examining clinician diagnosed VVC based on the 2010 CDC sexually transmitted diseases Treatment Guidelines.18 The non-examining clinician who used the presence of yeast on wet mount and the absence of another aetiology for the discharge as the diagnostic criteria for VVC underestimated the diagnosis of VVC compared with the examining clinician (reference standard for VVC). Using the presence of yeast alone on wet mount from the SOVS would have had a sensitivity of 52% and a specificity of 98%.
Consistent with previous studies, saline microscopy was 65% sensitive compared with molecular tests in diagnosing TV.5 ,16 Despite good data, most clinical settings do not use NAAT to diagnose TV. Reasons for continued use of the wet mount include simplicity, convenience to provide immediate results and cost. In our study, up to 25% of participants diagnosed with TV by the reference standard were called back for treatment because the wet mount was negative and the molecular test was positive. In high prevalence settings, more accurate diagnoses may justify the increased cost of molecular testing.
TV infections were diagnosed by wet mount obtained from the SOVS less often compared with the COS in our study. COS are immediately taken to the laboratory by clinicians following the SE; SOVS were collected by participants, handed to the research assistant and then transferred to the laboratory. All on-site testing was conducted in the same laboratory by clinic personnel, and occasionally POC clinic testing took precedence over SOVS testing. This delay, although usually less than 10 min, decreased the sensitivity of the wet mount. If POC testing from SOVS is used, clinics must ensure that specimens are processed immediately.
Abdominal pain as a presenting complaint was present in all four women who were diagnosed with pelvic inflammatory disease, suggesting that a complete assessment is necessary in all women complaining of abdominal pain. The single case of syphilis was diagnosed based on positive serological tests. The participant diagnosed with herpes complained of lesions at presentation, while the four women with genital warts were incidentally diagnosed on physical examination.
Our study has several limitations. There were several examining clinicians and a single non-examining clinician. This might be a source of variability in our analyses. The Gram stains for the diagnosis of BV prepared from the SOVS were interpreted only once by a single technician. Since there can be inter-observer variation in the interpretation of Nugent's score this may have led to bias. In addition, phase contrast was not used for the preparation of saline microscopy thereby reducing its sensitivity.
Another important limitation of this study was the lack of an established reference standard for the diagnosis of VVC. A culture or POC gram stain for VVC was not used because it is not part of the routine clinical evaluation at the STI clinic and would have required participants to obtain an additional SOVS. Of note, even culture is not considered to be specific for VVC since 10%–15% of asymptomatic women are colonised with candida and hence are culture positive.20
This study conducted at an STI clinic with a higher prevalence of lower genital tract infections may not apply to other clinical settings. Our study focuses on common vaginal infections (BV, TV and VVC). Less common infections like aerobic vaginitis were not diagnosed or addressed in this study. The latter would require a physical examination for diagnosis. All participants were tested for GC and CT. The STI clinic and the research laboratory, however, used different assays for testing GC and CT.
In conclusion, SOVS without a concurrent SE cannot be used to adequately diagnose BV, TV and VVC. Current diagnostic criteria for vaginitis which are partly based on physical findings must change before the SE can be eliminated from the diagnostic algorithms for vaginitis. The application of liberal diagnostic criteria would increase sensitivity but lower specificity. Cost benefits from eliminating the SE and using only tests from SOVS may be negated by long-term costs of mistreatment.
Key messages
-
Eliminating the speculum examination from the diagnosis of common vaginal infections must be accompanied by changes in current diagnostic criteria which are partly based on physical findings.
-
Cost benefits from eliminating the speculum examination may be negated by costs and consequences of overtreatment.
-
Eliminating the speculum examination does not increase the rate of missed diagnoses among women presenting with abnormal vaginal discharge and no abdominal pain.
Acknowledgments
Dr Clifford Qualls of the University of New Mexico Clinical and Translational Science Center, #1UL1RR031977-01 for help with the statistical analysis.
References
Footnotes
-
Contributors RHS: (1) Contributed to the conception and design of the study, acquisition of data, analysis and interpretation of data. (2) Drafted the article and revised it critically for important intellectual content. (3) Approved the final version of the article for publication. JMZ: (1) Contributed to the conception and design of the study. (2) Assisted with revising the article critically for important intellectual content. (3) Approved the final version of the article for publication. KMB: (1) Contributed to acquisition of data, analysis and interpretation of the data. (2) Revised the article for important intellectual content. (3) Approved the final version of the article for publication. TM: (1) Contributed to acquisition of data. (2) Revised the article critically for important intellectual content. (3) Approved the final version of the article for publication. CG: (1) Contributed to the conception and design of the study. (2) Revised the manuscript critically for important intellectual content. (3) Approved the final version of the article for publication. KGG: (1) Contributed to the conception and design of the study, analysis and interpretation of the data. (2) Assisted with drafting the article and revised it critically for important intellectual content. (3) Approved the final version of the article for publication.
-
Funding Funding from an anonymous donor to the primary author while in the Department of Obstetrics and Gynaecology at Johns Hopkins University School of Medicine was used to support this study. Funding for CG: NIH U-54EB007958 and NIH HPTN U-01 AI068613.
-
Competing interest None.
-
Patient consent Obtained.
-
Ethics approval The institutional review boards of the Johns Hopkins Medical Institutions and the public health committee of Baltimore City Health Department approved this study.
-
Provenance and peer review Not commissioned; externally peer reviewed.