Article Text

Abstract
Background Roflumilast, a phosphodiesterase 4 inhibitor, has been approved for the prevention of chronic obstructive pulmonary disease (COPD) exacerbations. It is unclear which patients will have a favourable benefit–harm balance with roflumilast. Our aim was to quantitatively assess the benefits and harms of roflumilast (500 µg/day) compared with placebo.
Methods We used summary data released by the US Food and Drug Administration to estimate the treatment effects of roflumilast. Data from trials and observational studies were used to estimate the baseline risks for COPD exacerbations and gastrointestinal, neurological and psychiatric harms associated with roflumilast. Using simulation, we calculated the probability that roflumilast provides net benefit. We examined the impacts of different baseline risks for exacerbations and the severity of exacerbations, and varied weights (ie, relative importance) for outcomes and treated death as a competing risk in the analyses.
Results The probability that roflumilast provides net benefit approximates 0% across different age categories of men and women with varying baseline risks for exacerbations. Using different weights for outcomes did not change the probability that roflumilast provides a net benefit. Only in the sensitivity analysis restricted to the prevention of severe exacerbations was there a probability of >50% that roflumilast provides a net benefit if the baseline risk of having at least one severe exacerbation per year exceeds 22%.
Conclusions Our results suggest that roflumilast only provides a net benefit to patients at a high risk of severe exacerbations. Guideline developers should consider different recommendations for patients with COPD at different baseline risks for exacerbations.
Statistics from Altmetric.com
Key messages
What is the key question?
-
What is the benefit–harm balance of roflumilast (500 µg/day) in patients with moderate to severe COPD and a history of exacerbations compared with placebo?
What is the bottom line?
-
The benefit–harm balance of roflumilast is only favourable for a small subgroup of patients with COPD at high risk for severe exacerbations and guideline developers should consider different recommendations for and against roflumilast for patients at different risks for moderate or severe exacerbations, respectively.
Why read on?
-
This is one of the first benefit–harm assessments of roflumilast that used a quantitative, comprehensive and transparent approach.
Introduction
Chronic obstructive pulmonary disease (COPD) poses a great burden for patients and healthcare systems because it is a leading cause of mortality and morbidity worldwide.1 ,2 While inhaled drug treatments, pulmonary rehabilitation, long-term oxygen and surgery provide some benefits to patients with COPD,3 finding additional drug treatments that can effectively target important goals of the management of COPD such as symptom relief and reduction of COPD exacerbations is currently a major focus of research and drug development.4–7
Phosphodiesterase 4 (PDE4) inhibitors are among the drugs that have raised hope for more effective COPD treatment. Many phase II and III randomised controlled trials (RCTs) have explored the efficacy and safety of the PDE4 inhibitors roflumilast and cilomilast in patients with COPD. As a result, roflumilast was recently approved by the US Food and Drug Administration (FDA) and the European Medicines Agency (EMA) for reducing the risk of exacerbations in patients with severe COPD and a history of exacerbations.8 ,9 Cilomilast was not approved by the FDA or EMA in large part because its benefits did not appear to exceed its harms. A Cochrane systematic review of PDE4 inhibitors in COPD concluded that, while roflumilast reduced the (relative) risk of exacerbations by around 20% compared with placebo, it was indeed associated with harms such as diarrhoea, nausea, depression and weight loss.10
Currently, it is still difficult to judge whether or not the benefits of roflumilast outweigh the harms. Clinicians are left with uncertainty about whether or not to recommend roflumilast to patients and whether the balance of benefits and harms varies among subpopulations within the approved population. Judging the benefit–harm balance of roflumilast is challenging because the drug has differential effects on distinct outcomes that are of varying importance to patients and that occur with different frequency. Trial reports and systematic reviews typically provide data on benefit and harm outcomes separately, with no attempt to integrate the two types of outcomes.
The aim of this study was to estimate the benefits and harms of roflumilast compared with placebo in patients with COPD giving consideration to multiple outcomes, baseline risks and patient preferences, and using a systematic approach for identifying and synthesising relevant sources of evidence.
Methods
Definition of the target population, intervention and outcomes
The population of interest included patients with moderate to severe COPD with a history of exacerbations, for whom roflumilast (1×500 µg tablet per day) was approved.9 The outcomes, evaluated over 1 year, included moderate or severe exacerbations prevented and harms. We defined a moderate exacerbation, following the definition of the manufacturer, as a COPD event requiring outpatient treatment and defined a severe exacerbation as a COPD event resulting in hospitalisation or death.11 Harm outcomes included gastrointestinal (acute pancreatitis, diarrhoea, nausea and weight loss), psychiatric (insomnia, anxiety, depression and suicide) and neurological (headache and dizziness) symptoms or disorders.
Selection of data sources
Treatment effect estimates
We identified a Cochrane review10 of PDE4 inhibitors and the FDA documents publicly available online (medical reviews of roflumilast)11 as the best available data source for estimating the treatment effects of roflumilast. The FDA documents included all data presented in the Cochrane review but provided substantial additional information—for example, on incidence rate ratios and on harm outcomes.
Baseline risks without roflumilast for a time period of 1 year
The baseline risk (the risk for outcomes at treatment initiation) has a large impact on benefit–harm assessment. We relied on observational studies for estimating the baseline risk for outcomes whenever possible because the control group risk in RCTs might not reflect the risk of patients with COPD seen in practice. For some outcomes where we could not find appropriate data from observational studies, we used the risk in the control group of RCTs. Although a time horizon of >1 year would be relevant for patients and physicians, we decided not to do any analyses beyond 1 year because of the absence of trial data on the long-term effects of roflumilast.
Weights (relative importance) for outcomes
We considered that the benefit and harm outcomes are, on average, of different importance to patients. We could not find a study (eg, preference-eliciting survey) that provides weights for all outcomes for our decision-making context. We therefore used various approaches to assigning weights to outcomes in the analysis to explore how they affect the benefit–harm balance.
Statistical analysis
We conducted a benefit–harm assessment of roflumilast following the Gail approach that was developed by the National Cancer Institute to estimate the benefit–harm balance of tamoxifen for the prevention of breast cancer.12 This approach combines data on treatment effects, baseline risks and relative importance of outcomes to provide a net benefit–harm index for decision-making. For a patient with COPD of a certain age, sex and with a certain baseline risk of exacerbations, the net benefit–harm index indicates whether roflumilast increases or decreases the occurrence of patient-centered outcomes overall (weighted by relative importance of outcomes) compared with placebo over 1 year. A positive index indicates that roflumilast provides more benefit than harm. We used simulation to calculate the probability of roflumilast being beneficial as the probability that the index is positive. In sensitivity analyses, we examined the impacts of the severity of exacerbations on the index. Details of the Gail approach are provided in the online appendix.
Results
Data inputs
Table 1 lists the data selected for the benefit–harm assessment of roflumilast. Treatment effect estimates of roflumilast on exacerbations are based on data from the ‘pivotal studies pool’ of the FDA documents. It consisted of two pivotal RCTs that focused on a population with severe COPD and a history of exacerbations, which reflected the indication for roflumilast.13 In all other RCTs the inclusion criteria did not require participants to have a history of exacerbations and exacerbations were not the primary outcome. Treatment effect estimates on harms are based on data from the ‘COPD safety pool’ of the FDA documents, which consisted of 14 RCTs. The harms associated with roflumilast are likely to be independent of the history of exacerbations, so we did not restrict the safety data to the pivotal RCTs. For sensitivity analysis focusing on severe exacerbations, we used the specific treatment effect for severe exacerbations as the outcome for the analysis.
Data for the benefit–harm assessment of roflumilast for patients with COPD
Estimates for the incidence of depression14 and weight loss15 are based on observational studies in patients with COPD. Estimates for the incidence of acute pancreatitis16 and suicide17 are from observational studies or surveillance of general populations because these are more rare events for which COPD-specific data are not available or are very imprecise. Baseline risks for other harm outcomes where we could not find appropriate data from observational studies are based on the placebo group in the FDA's ‘COPD safety pool’.11 Estimates of mortality stratified by age (<65 years or ≥65 years) and sex are from 10 COPD cohorts with 13 914 patients (1350 deaths).18 As the Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) study suggested,19 around 70% of patients with ≥1 exacerbations in year 1 (ie, those who would potentially qualify for roflumilast) had at least one exacerbation in year 2 of the study. To cover a realistic spectrum of COPD patients with different baseline risks, we performed the analysis for patients at 30%, 60% or 90% risk for at least one moderate or severe exacerbation per year, respectively. In sensitivity analysis restricted to the prevention of severe exacerbations, we considered three different levels of baseline risk (10%, 20% or 30% risk for at least one severe exacerbation per year) because that reflects a range around the risk of severe exacerbations observed in the control group of the pivotal trials (16%).
The different approaches to assigning weight (relative importance of outcomes) are shown in table 1. We considered first equal weights (1.0) for all outcomes, and then weights of 1.0 for life-threatening outcomes, 0.5 for serious and 0.1 for mild outcomes, a similar approach to that proposed by Gail.12 In order not to overestimate the harms, we considered smaller weights (0.25 or 0.05) for those harm outcomes that tend to occur together (eg, patients may have both depression and anxiety). For sensitivity analysis focusing on severe exacerbations, we considered the same weights as in our main analysis but changed the weight for exacerbations from 0.5 to 1.0.
Benefit–harm assessment
Table 2 shows the expected number of cases for the 11 outcomes in 10 000 men aged <65 years treated with and without roflumilast over 1 year, stratified by the patients’ baseline risk of moderate to severe exacerbations. For example, in men aged <65 years with a baseline risk where 60% of patients have at least one moderate or severe exacerbation over the year, 4055 patients are expected to have at least one exacerbation in the treatment group and 4338 patients in the placebo group (accounted for mortality using Gail approach). Hence, moderate to severe exacerbations are prevented in 284 patients if 10 000 patients are treated with roflumilast. However, at the same time, four cases of acute pancreatitis are expected in the treatment group while one case is expected in the placebo group. Thus, there are three excess cases of acute pancreatitis. As the patients’ baseline risk of moderate to severe exacerbations increases, more cases of exacerbation would be prevented (positive numbers) whereas the harms would remain the same (negative numbers).
Expected numbers of cases (patients with ≥1 events) over 1 year for every 10 000 patients (men, age <65 years) treated with and without roflumilast
In table 3 the benefits and harms are combined (ie, net benefit–harm index using the established Gail approach) for men and women in different age groups (<65 years or ≥65 years) with a varying baseline risk of moderate to severe exacerbations. We conducted three types of analyses using different weights as shown in table 1, where we weighted the outcomes equally (analysis I), based on the importance of outcomes (analysis II), or based on both the importance and co-occurrence of harm outcomes (analysis III, main analysis). For example, in men aged <65 where 60% of patients have at least one moderate or severe exacerbation per year, the net benefit–harm index is −148 with a 0.0% probability that the index is positive and roflumilast beneficial. We found that roflumilast had no net benefit in every scenario in table 3 (patients at different baseline risks of moderate or severe exacerbations), and the probabilities that the index is positive all equal 0.0%. We found that sex and age had little effect on the estimates of the net benefit–harm index.
Net benefit–harm index for treatment of COPD with roflumilast
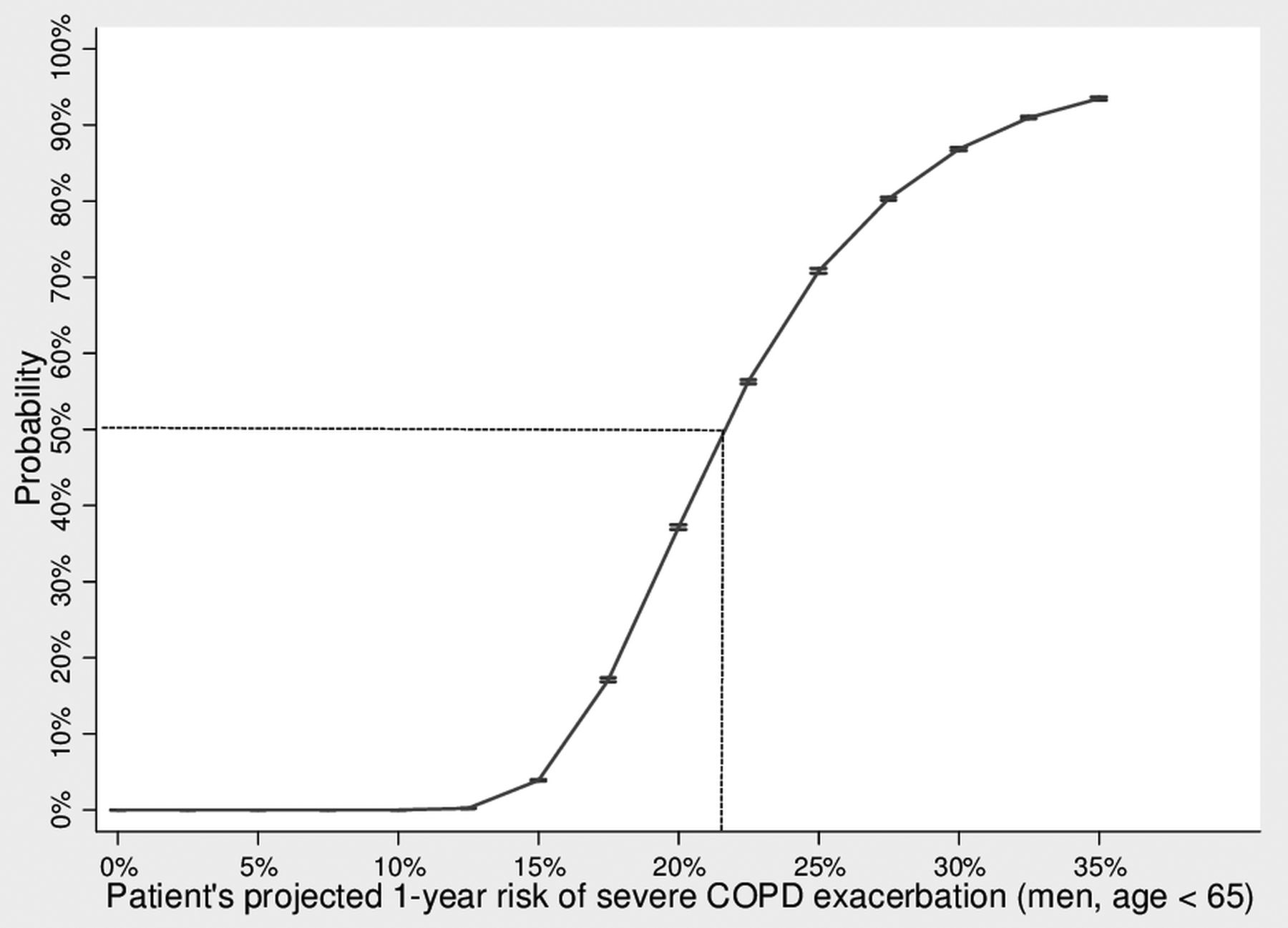
We also conducted a sensitivity analysis focusing on severe COPD exacerbations (table 3). Roflumilast was found to be beneficial, as the indexes suggest, in some patients with an elevated baseline risk of severe exacerbations. Figure 1 shows that the probability that the index is positive is greater than 50% if the patients’ baseline risk of severe exacerbations is greater than 22%.
{kind=link}
The Figure shows the probability that the net benefit-harm index is positive (benefits outweigh harms) when treating patients with varying projected 1-year risk of severe COPD exacerbation.
Discussion
Our analyses showed that roflumilast has no net benefit for younger and older men and women with COPD and a history of moderate to severe exacerbations irrespective of how the benefit and harm outcomes were weighted and irrespective of the baseline risk for moderate to severe exacerbations. However, when we restricted the analysis to severe exacerbations, we found that roflumilast provides more benefit than harm above a baseline risk of 22% for a severe exacerbation over the course of a year.
Our results reflect the complicated regulatory history for PDE4 inhibitors where concerns about gastrointestinal, neurological and psychiatric harms delayed approval of roflumilast.20 The FDA provides a quantitative benefit–harm assessment in their publicly available statistical review of roflumilast,21 but the analysis only considered gastrointestinal harms, did not consider different baseline risks or competing risks, and made no attempt to provide an estimate of net benefit (ie, a summary of benefits and harms). The FDA statistical review explicitly stated that the benefit–harm assessment is up to clinical judgement, but the FDA medical review and the transcript of the advisory committee meeting did not entail a quantitative assessment or a discussion of the benefit–harm balance.11 ,22 In our analysis, the evidence for each key element (treatment effects, baseline risks, importance of outcomes and competing risks) is explicitly laid out and considered simultaneously, which allows consideration of different scenarios when roflumilast may provide more benefit than harm and when it may not.
In order to assess whether our analyses were robust to the selection of data sources, we conducted a series of analyses. We varied the relative weighting of outcomes, arguably the most controversial part of any benefit-harm assessment, from treating all outcomes the same (ie, assigning the same weights) to an approach where we considered some harms of less importance and where we accounted for the joint occurrence of harm outcomes in order not to overestimate harms. Exacerbations received a substantial weight in all analyses. Of note, a weight of 0.5 for exacerbations in the main analysis did not minimise their importance because all of the harm outcomes except for suicide received the same or less weight. Although suicide is rare and had a minimal impact on the benefit–harm balance, we considered it most consequential and therefore assigned the largest weight. We did not consider using different treatment effects because we believed that the pivotal and safety pool of the FDA RCTs provided the most valid evidence. Also, we did not consider different baseline risks for harm outcomes since COPD-specific estimates for some gastrointestinal, neurological and psychiatric outcomes are relatively scarce. The observational studies and the placebo groups we identified are likely to provide the best available evidence. However, it still may be reasonable to challenge our decisions about data sources, which highlights the importance of using a comprehensive and transparent approach for quantitative benefit–harm assessment.
We believe that the results of this study will aid guideline developers to make evidence-based recommendations. The available scientific evidence and the benefit–harm balance are among the key elements for developing practice recommendations, as outlined in the frequently used frameworks such as the Grading of Recommendations Assessment, Development and Evaluation.23 ,24 Based on our analysis, the benefit–harm balance is not favourable when looking at the entire group of COPD patients with a history of prior exacerbations, with a probability of roflumilast to provide more net benefit than harm approximating 0%. A guideline panel may consider issuing a strong or at least a weak recommendation against the use of roflumilast in patients with COPD with a history of moderate exacerbations. However, for patients at high risk of a severe exacerbation, a guideline panel may come up with a weak or even strong recommendation for using roflumilast depending on cost and local circumstances. Our considerations of possible recommendations described here are not meant to be directive, but they illustrate the usefulness of having separate quantitative estimates for the benefit–harm balance according to the risk and severity of exacerbations.25
One strength of our study is the careful identification of the best available evidence. By using FDA data and data from large observational studies, we went considerably beyond the published RCTs and the Cochrane review, respectively, and relied upon the best available evidence. By using trial summary data released by the FDA, we believe that we are less prone to publication bias and, since these trials were conducted by the same manufacturer, the heterogeneity across trials is likely to be limited. Another strength is the use of a transparent approach for quantitative benefit–harm assessment that allows for sensitivity analyses as presented here and additional sensitivity analyses in the future. Also, we considered the statistical uncertainty of treatment effects and baseline risks for outcomes following the Gail approach. This allowed for assessment of a wide variety of scenarios for different patient groups and sources of evidence to facilitate identification of a risk-stratified subgroup of patients who may benefit from an intervention.
A weakness of this analysis is the incomplete adjustment for the joint distribution of outcomes. We accounted for death as a competing risk and accounted for the co-occurrence of harm outcomes. Ideally, observed correlations of all outcomes involved could inform the analyses, but this requires availability of and access to individual patient data.26 We based our analyses on RCTs that compared roflumilast with placebo and did not consider recent or ongoing RCTs that investigate roflumilast as add-on treatment to inhaled agents. In these RCTs the treatment benefits are likely to be smaller with roflumilast compared with the evidence considered here. We selected evidence for harms from a larger pool of trials that is more comprehensive, but the harm outcomes (eg, psychiatric events) may not be uniformly captured across these trials. We modelled the benefit–harm balance in 1 year for our analysis, but the time horizon would not be sufficient to include all potential harms or benefits caused by roflumilast that might occur later.
Finally, some may argue that there is insufficient evidence to attribute pancreatitis and suicide to roflumilast since the numbers of events are so small. We agree, but decided to include these outcomes for greater transparency and because benefit–harm models should include all outcomes that would be potentially important for decision makers. As we considered the low precision around the effect estimates for these outcomes, we show their (small) impact on the benefit–harm balance. Also, one may argue that weight loss can be beneficial to some patients, but we treated it as harm because the FDA considered weight loss as an adverse event. We have followed this approach but assigned a relatively small weight to weight loss in the analysis. We did not consider lung function in our benefit–harm assessment because it is a surrogate for patient important outcomes we already included in the analyses. We did not consider health-related quality of life because it combines the consequences of exacerbation avoidance and harms, whereas we were interested in specific benefit and harm outcomes and their individual contribution to the benefit–harm balance.
In conclusion, our systematic and transparent benefit–harm assessment of roflumilast for patients with COPD with a history of exacerbations suggests that roflumilast has no net benefit for most patients. However, if patients are at a high 1-year risk of severe exacerbations (>22%), roflumilast is likely to provide more benefit than harm. Guideline developers should consider issuing different recommendations for patients at different risks for moderate and severe exacerbations.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors TY contributed to the study protocol, obtained the data, contributed to the statistical analysis and drafted the first version of the report. KF contributed to the study protocol, obtained the data and additional information from the US Food and Drug Administration, contributed to the statistical analysis and revised the report. CMB, SS, COW and TL contributed to the study protocol and the statistical analysis and revised the report. RV contributed to the study protocol and the statistical analysis. MAP conceived the study idea, contributed to the study protocol, obtained the data, contributed to the statistical analysis and drafted the first version of the report.
-
Funding Supported by grant number UL1 RR 025005 from the National Center for Research Resources (NCRR), a component of the National Institutes of Health (NIH), and NIH Roadmap for Medical Research.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.