Article Text

Statistics from Altmetric.com
Heart disease is the joint most common cause of maternal death in the UK.1 The most common cardiac causes of death involve cardiomyopathy and pulmonary hypertension (fig 1⇓).

Cardiac causes of maternal deaths in the UK: confidential enquiry into maternal deaths 1997–99 (total maternal deaths = 409, cardiac deaths = 41).1
Congenital heart disease (CHD) is infrequently associated with maternal death, but forms the greatest workload in a cardiac antenatal clinic and may be associated with significant maternal morbidity. The population of adults with CHD is growing rapidly both in numbers and complexity of disease. There were an estimated 133 000 adults with CHD in the UK in 2000, 10 000 with complex disease; the population is expected to grow to 166 000 by 2010 with a 50% increase in those with complex conditions. Half this population are women, the majority of whom are well enough to contemplate pregnancy; this can either be seen as a major problem, or as an indication of the successes of congenital cardiac surgery and cardiology.
Preventing maternal death must be the prime aim of all cardiologists involved in the care of pregnant women. However, many women with heart disease can have a successful pregnancy; it is important that their doctors are educated so that they are not inappropriately advised against pregnancy. Conversely, patients for whom pregnancy carries an unacceptable risk (table 1⇓) must be correctly counselled and given contraceptive advice. A detailed review of contraception in heart disease is beyond the scope of this article.
Pregnancy contraindications
PRE-PREGNANCY COUNSELLING
Complex heart disease is no bar to sexual activity. Discussions on future pregnancies and their prevention should begin in adolescence, both to prevent accidental and possibly dangerous pregnancies and to allow patients to come to terms with their future childbearing potential.
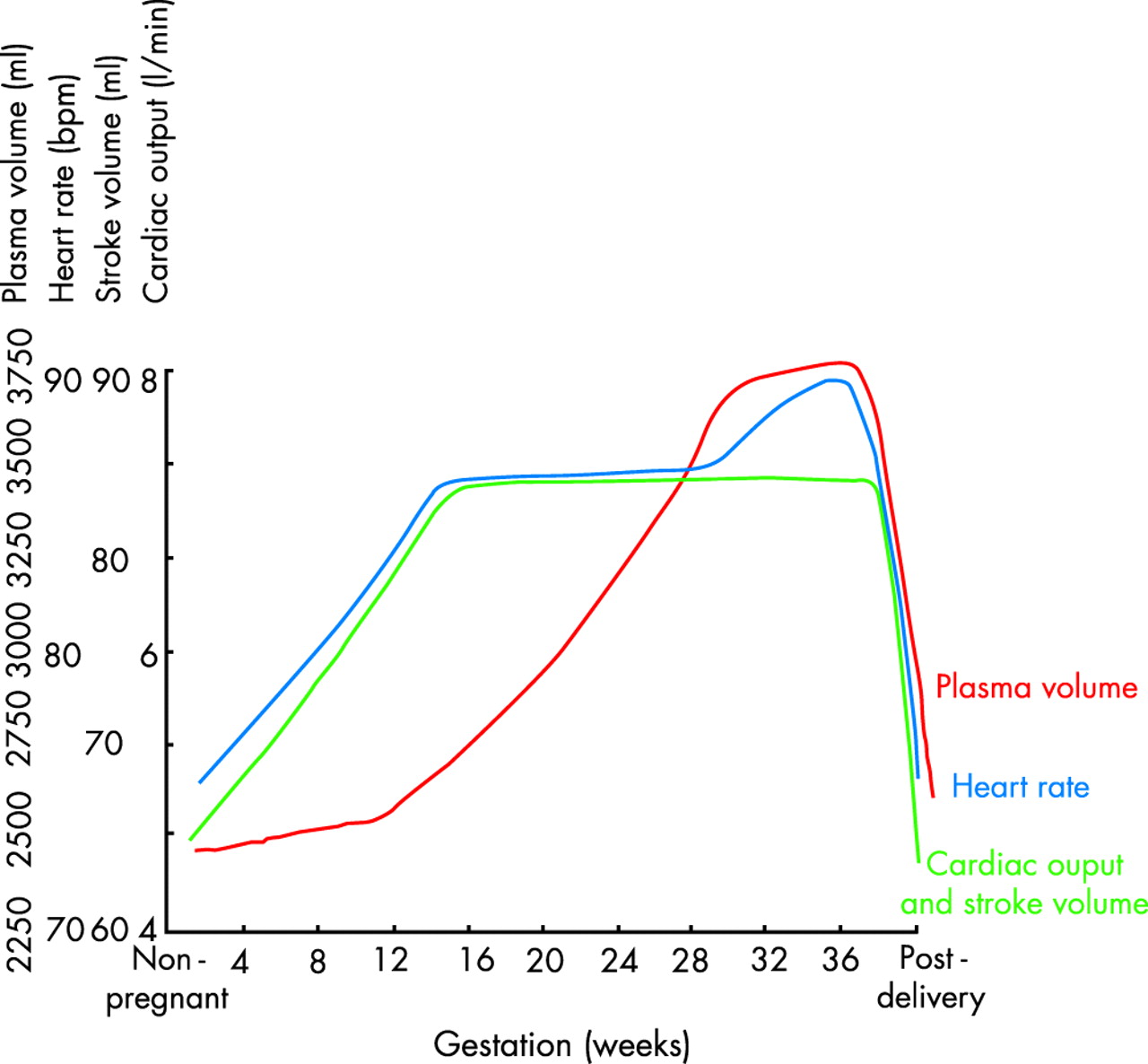
For some complex conditions, there is little or no evidence to support the advice given by the cardiologist, either because of the rarity of the patient’s disease or because they represent a new cohort of survivors to adulthood with surgically modified disease. These patients need a thorough assessment of their current cardiac status and appropriate advice based on how their cardiovascular system is likely to adapt to the physiological changes of pregnancy (fig 2⇓).

Physiological changes in pregnancy.8 Systemic and pulmonary vascular resistance fall during pregnancy. Blood pressure may fall in the second trimester, rising slightly in late pregnancy. Note that cardiac output and stroke volume peak by 16 weeks gestation.
The cardiologist’s role is to give the woman an estimate of both maternal and fetal risk to allow her to make an informed decision about embarking on a pregnancy, and to provide appropriate antenatal care. Information should include:
Estimate of maternal mortality as well as morbidity—for example, the likelihood of pregnancy resulting in heart failure requiring hospital admission, exacerbation of arrhythmias, long term deterioration in ventricular function
Minimising maternal risk:
–if necessary by catheter or surgical intervention before conception
–timing of pregnancy—for those with a systemic right ventricle or univentricular heart, pregnancy is likely to be tolerated better when the patient is in her 20s rather than her late 30s
Estimation and minimising fetal risk including:
–recurrence risk (may need referral to geneticist)—for the majority of women, with no family history of CHD and no chromosomal abnormality, the risk of recurrence of CHD in the fetus is around 5%
–maternal drug treatment may need changing before conception or once pregnant
–maternal factors which may compromise the fetus—for example, cyanosis, uncontrolled arrhythmia
Joint antenatal care with a high risk pregnancy obstetric team. Women with important cardiac disease should be managed in a centre with appropriate expertise despite the inconvenience of distance.
For most cardiac conditions a normal vaginal delivery with good analgesia and a low threshold for forceps assistance is the safest mode of delivery for the mother, since it associated with less blood loss and less rapid haemodynamic changes than caesarean section. The few maternal cardiac indications for delivery by section include Marfan syndrome, aortic aneurysm of any cause, and an acutely unwell mother. Women with a mechanical Bjork-Shiley mitral valve who have opted for warfarin anticoagulation should also be considered for elective section to reduce the time off warfarin.
ACQUIRED HEART DISEASE
Ischaemic heart disease
Acute myocardial infarction is rare in pregnant women, occurring in 1:10 000 pregnancies, but the incidence is increasing, perhaps reflecting the trend towards older maternal age. Mortality is 37–50%,2 and the risk of death is greatest if the infarct occurs late in pregnancy, in women under 35 years old, or if delivery is within two weeks of the infarct. There were five UK deaths from acute myocardial infarction between 1997–99.1
Cardiac troponin I is unaffected by normal pregnancy, labour, and delivery and therefore it is the investigation of choice in the diagnosis of acute coronary syndrome.3 Because of the risk of haemorrhage, systemic thrombolysis should be avoided for 10 days post-section and late in pregnancy in case of premature labour. Primary stenting may be the best option, but there are a paucity of data to guide management, so the risk of maternal death must be weighed against the risks of radiation, antiplatelet drugs, and intracoronary thrombolysis.4,5
Cardiomyopathy
Dilated cardiomyopathy
Pregnancy is poorly tolerated in women with dilated cardiomyopathy. The risk of maternal death is approximately 7% if the patient is in New York Heart Association (NYHA) functional class III or IV. Other adverse risks factors include ejection fraction < 20%, mitral regurgitation, right ventricular failure, atrial fibrillation, and systemic hypotension. Such patients should be counselled against pregnancy: as well as the risk of maternal death, there is a high risk of overt heart failure occurring during pregnancy, irreversible deterioration in ventricular function, and fetal loss.
Distinguishing the symptoms and signs of a normal pregnancy from those of heart failure requires careful clinical assessment (table 2⇓). Heart failure should be managed as in the non-pregnant patient, but angiotensin converting enzyme (ACE) inhibitors are associated with renal agenesis and should be avoided until after delivery.
Signs and symptoms of normal pregnancy versus heart failure
Hypertrophic cardiomyopathy
Asymptomatic patients with hypertrophic cardiomyopathy (HCM) usually tolerate pregnancy well and few develop symptoms for the first time during pregnancy.6,7
Maternal death is uncommon1 and there is no evidence to suggest the risk of sudden death is increased by pregnancy.6,8 There is little evidence that echocardiographic findings correlate with maternal morbidity, although massive hypertrophy may be an adverse risk factor.7 In addition, patients with heart failure and severe symptomatic restrictive physiology are unlikely to tolerate the haemodynamic changes of pregnancy and they should be advised against pregnancy.
Dyspnoea and angina may be relieved by β blockade to improve coronary perfusion and allow ventricular filling time. Atrial fibrillation is poorly tolerated because of the effects of tachycardia and loss of atrial transport; rate control and prompt reversion to sinus rhythm are needed.
Vaginal delivery is usually well tolerated. Careful fluid management is needed to maintain ventricular filling but avoid pulmonary venous congestion.
In an uncomplicated pregnancy, the main risk to the fetus is the 50% recurrence risk. Hypertrophic cardiomyopathy is rarely diagnosed in early life, and offspring should be screened until they are 20–25 years old.
Peripartum cardiomyopathy
Peripartum cardiomyopathy is defined as cardiac failure with left ventricular ejection fraction < 45% occurring in the last month of pregnancy or within five months of delivery, in the absence of any identifiable cause of heart failure.9
It is a rare condition, occurring in 1 in 3000–15 000 pregnancies. The pathogenesis is poorly understood, but some form of myocarditis, possible viral, has been postulated.10 Fetal outcome is good, as expected in a condition which is not symptomatic until the end of the third trimester. However, there is an increased incidence of prematurity and low birth weight suggesting that the underlying disease process begins before the onset of maternal symptoms.10
Maternal mortality is up to 20%. Adverse risk factors include age > 30 years, multiparity, twin pregnancy, and the 50% of women in whom left ventricular dilation and dysfunction persist.11 Treatment is the same as for any form of cardiomyopathy with impaired systolic ventricular function.
The major challenge for the cardiologist is the assessment of recurrence risk in future pregnancies. If left ventricular function is persistently abnormal a year following delivery, the risk of death in a subsequent pregnancy is around 20%. If left ventricular function is completely normal, the risk of death in a subsequent pregnancy is probably small; however, there is a substantial risk of recurrence of symptomatic heart failure and permanent impairment of left ventricular function in any subsequent pregnancy.12
Rheumatic heart disease8
Rheumatic heart disease is increasingly rare in women of childbearing age in the UK, the majority of cases occurring in immigrant populations. Stenotic valvar lesions are generally less well tolerated than regurgitant lesions, especially if severe and left sided.
Mitral stenosis
The combination of impaired diastolic flow through the stenotic valve and pregnancy induced tachycardia and increased stroke volume causes increasing left atrial pressure and dyspnoea, and may result in pulmonary oedema. The patient is further compromised if atrial fibrillation occurs. In addition, the development of secondary pulmonary hypertension may result in right ventricular failure.
For patients with moderate uncomplicated mitral stenosis, symptoms may peak at around 20–24 weeks gestation as cardiac output and intravascular volume peaks, and then stabilise. Patients with severe mitral stenosis remain at risk of heart failure and pulmonary oedema through the third trimester and into the puerperium.
The cornerstone of treatment is bed rest, diuretics, and rate control with β blockade to allow left ventricular filling time. Heparin should be used for those with atrial arrhythmia, a dilated left atrium, and during bed rest. Balloon mitral valvoplasty may have to be considered if the mother remains haemodynamically compromised and prematurity means the fetus cannot be safely delivered.
Mechanical prosthetic heart valves
Mechanical heart valves are a major source of concern during pregnancy. The risk to the fetus of warfarin (risk of embryopathy in the first trimester, haemorrhage, and fetal loss throughout pregnancy) needs to be balanced against the risk of heparin to the mother. Heparin does not cross the placenta, but is a less effective anticoagulant; even if meticulously monitored the mother is at risk of potentially fatal valve thrombosis.13 The fetal risk of warfarin is significantly reduced if the woman is adequately anticoagulated on ⩽ 5 mg warfarin.14
There is no consensus of opinion about the best form of anticoagulation in these women. However, less thrombotic valves such as a bileaflet tilting disc in the aortic position can probably be managed with aspirin and low molecular heparin with anti-Xa monitoring. One of the most thrombotic valves is the Bjork-Shiley in the mitral position. There is no safe regimen for such patients and they need to be involved in decision making, accepting a risk of major complication of up to 10%. The safest option for the woman is to remain on warfarin throughout the pregnancy, with an elective section to reduce the time off warfarin. Alternatives are heparin plus aspirin during the first trimester, converting to warfarin in the middle of pregnancy and back to heparin from 36 weeks, or to remain on heparin plus aspirin throughout the pregnancy. Warfarin is safe in breastfeeding women and must be reinstated immediately postpartum.
The choice of heparin is also controversial. Low molecular weight heparin with anti-Xa monitoring tends to be favoured in the UK, but in the USA unfractionated heparin predominates ever since a pharmaceutical industry report suggested that low molecular weight heparin may be contraindicated for mechanical valves in pregnancy.15
CONGENITAL HEART DISEASE
Bicuspid aortic valve stenosis
Most young patients with aortic stenosis are asymptomatic. If the following criteria are also met, pregnancy is likely to be tolerated:
Normal resting ECG or voltage increase only: no ST segment depression
Normal exercise test: appropriate rise in blood pressure and heart rate, no ST segment changes
Good LV function
Pre-pregnancy aortic valve echo Doppler peak pressure drop < 80 mm Hg, mean pressure drop < 50 mm Hg. Note that the measured aortic valve gradient should increase during pregnancy as blood volume and cardiac output increase.
Signs suggestive of decompensation include disproportionate dyspnoea or tachycardia, angina, pulmonary oedema, new ECG changes, and a fall in peak echo Doppler gradient indicating a deterioration in ventricular function. Management includes bed rest and β blockade to allow coronary filling. Most patients will reach a point in the third trimester when the baby can be safely delivered. In extreme situations, balloon aortic valvotomy or aortic valve replacement may need to be considered, although the latter carries about a 30% risk of fetal loss.16,17
If the mother is well at term there is no contraindication to normal delivery, avoiding vasodilators and hypovolaemia.
Coarctation of the aorta
It is usually women with repaired coarctation who present for pregnancy. Magnetic resonance imaging should be used to assess the coarctation site before pregnancy, but can be safely performed during pregnancy if there is concern about recoarctation or aneurysm formation. The only caveats are to perform the scan in the left lateral position to avoid syncope caused by inferior vena cava compression by the gravid uterus, and the possibility that the third trimester patient may not fit in the scanner.
Blood pressure should be controlled with β blockers. Unless there is an aneurysm at the coarctation site, there is no contraindication to normal vaginal delivery as long as the second stage is not prolonged. Rarely a pregnant woman presents with a native coarctation. Blood pressure should be aggressively treated with β blockers and the baby delivered by elective section before term (~35 weeks gestation).
The major maternal risk is of aortic dissection, but mortality from pregnancy appears to be low whether or not there is adequate repair of the coarctation.18
Marfan syndrome and aortic dissection
The main maternal risk in Marfan syndrome is type A aortic dissection, repair of which carries a 22% maternal mortality.17 Even without aortic root dilation the risk of dissection for pregnant women with Marfan syndrome is about 1%. Patients with poor family history, cardiac involvement, and aortic root > 4 cm diameter or a rapidly dilating aorta are at high risk of dissection and should be advised accordingly.19,20 Those who elect to proceed with pregnancy should be treated with β blockers and undergo elective section. Patients should also be aware of the 50% recurrence risk.
Aortic dissection can occur without pre-existing disease in pregnancy, probably because of the hormonal changes and increased cardiovascular stress of pregnancy.
Bicuspid aortic valve with dilated aortic root may also be a risk factor for aortic dissection in pregnancy, with similar histological findings to that of Marfan syndrome.21
Small ventricular septal defect
The only risk from a small haemodynamically insignificant ventricular septal defect is of endocarditis. Antibiotic prophylaxis is recommended for this and other lesions22 for instrumental or complicated deliveries.
Unoperated secundum atrial septal defect
This common lesion frequently remains undiagnosed until pregnancy when the pulmonary flow murmur is accentuated. There is a small risk of developing atrial arrhythmias in older women with longstanding right heart volume overload. The only other risk is of paradoxical embolism, so if the patient is immobilised they should receive heparin thrombosis prophylaxis and support stockings. Endocarditis prophylaxis is unnecessary.
Repaired tetralogy of Fallot
Pregnancy is well tolerated in women who have had radical repair of tetralogy of Fallot, as long as ventricular function is good and there is no significant right ventricular outflow tract obstruction. Many have significant pulmonary regurgitation and may become more tired and breathless as pregnancy progresses, occasionally needing diuretic treatment or admission for bed rest.
Congenitally corrected transposition of the great arteries
Terminology in CHD can be confusing to the non-cardiologist; obstetricians, anaesthetists, and midwives may appreciate a simple diagram (fig 3⇓) attached to the front of the patient’s notes.

Schematic representation of congenitally corrected transposition of the great arteries (atrioventricular and ventriculo-arterial discordance). Pulmonary venous blood reaches the aorta via a morphological tricuspid valve and right ventricle. Systemic venous blood reaches the pulmonary artery via a morphological left ventricle.
Pregnancy is likely to be well tolerated in asymptomatic patients with congenitally corrected transposition of the great arteries (cTGA).23 However, systemic right ventricular function may deteriorate during pregnancy, presenting with heart failure. Systemic tricuspid atrioventricular (AV) valve regurgitation may also worsen during pregnancy but is usually well tolerated. Management is as for any patient with heart failure and AV valve regurgitation. The AV node is absent in cTGA, complete heart block occurring at any stage in life; pregnancy is better tolerated post-pacing.24
Post-Mustard or Senning repair of simple transposition of the great arteries
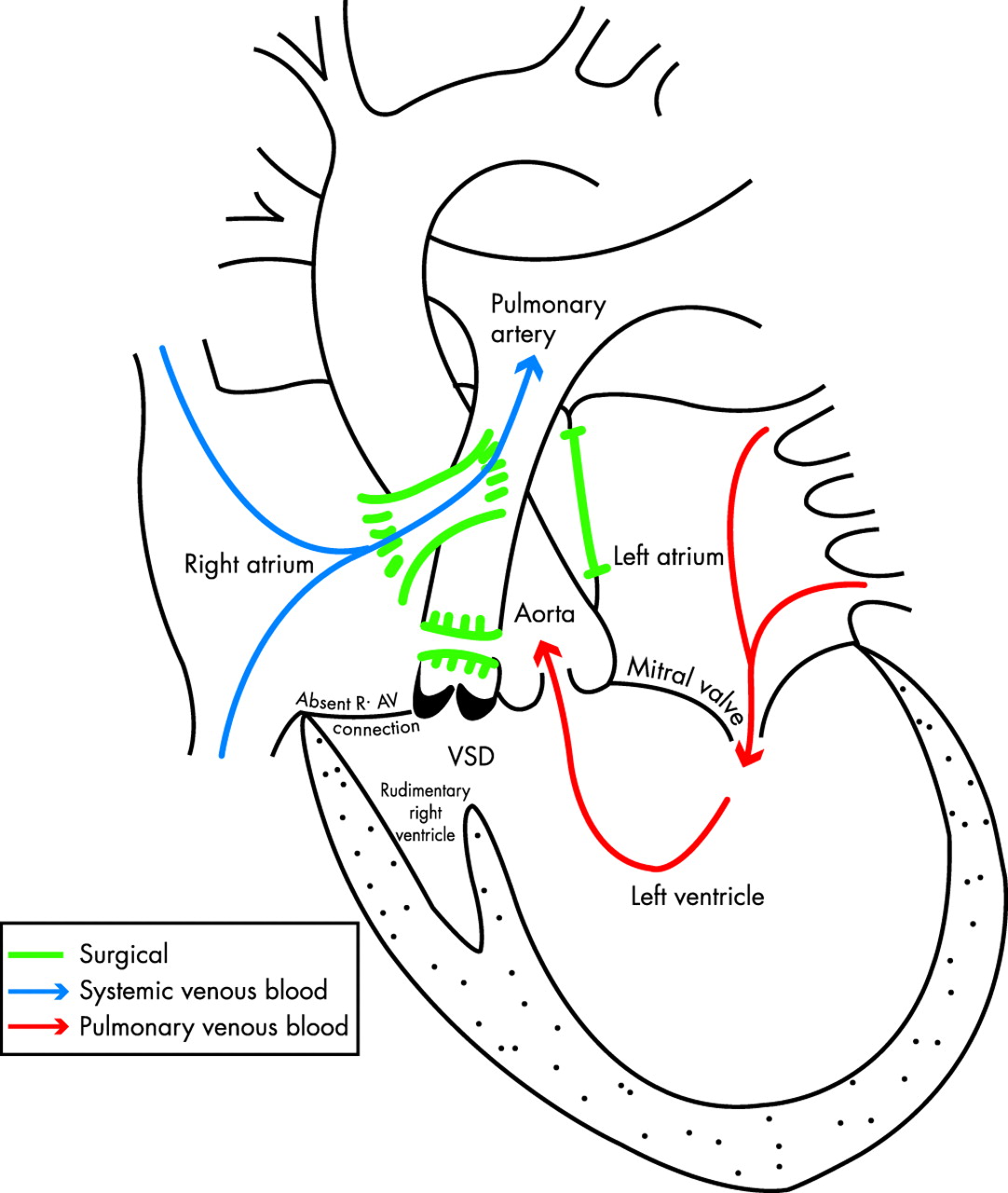
Following atrial re-routing, the tricuspid valve and right ventricle support the systemic circulation (fig 4⇓), with the same implications for pregnancy as in cTGA. AV node function is usually normal, but patients are at risk of atrial arrhythmia and sinus node disease as a result of extensive atrial surgery.

Schematic representation post-Mustard or Senning repair for simple transposition of the great arteries (atrioventricular concordance, ventriculo-arterial discordance). Re-routing of blood at the atrial level allows pulmonary venous blood to reach the aorta via a morphological tricuspid valve and right ventricle, and systemic venous blood to reach the pulmonary artery via a morphological left ventricle.
The pulmonary venous pathway must be demonstrated to be unobstructed pre-pregnancy, by transoesophageal echo or magnetic resonance imaging if transthoracic imaging is inadequate. A narrowed pulmonary venous pathway may only become symptomatic once pregnancy occurs, when the fixed obstruction acts as the physiological equivalent of severe mitral stenosis. A further caveat is that some patients develop unexplained pulmonary vascular disease in which case pregnancy is very high risk. With these exceptions, pregnancy is usually well tolerated in NYHA class I–II patients post-Mustard.25
Post-Fontan type operation
A Fontan type operation is the definitive palliative procedure for cyanotic patients with a functionally single ventricle in whom a biventricular repair is not possible. The ventricular mass is used to support the systemic circulation; there is no “pump” to support the pulmonary circulation so systemic venous blood reaches the pulmonary artery without pulsatile flow (fig 5⇓). The procedure aims to abolish cyanosis but the resulting circulation has a:

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Schematic representation of Fontan operation (atriopulmonary connection) for tricuspid atresia. The systemic and pulmonary circulations are separated by closing the atrial septal defect, ligating the pulmonary artery, and creating an anastomosis between the right atrium and the pulmonary artery.
limited ability to increase cardiac output, dependent on high systemic venous filling pressures
tendency to poorly tolerated atrial arrhythmia
prothrombotic circulation.
As a consequence, these patients are often advised against pregnancy. However, the maternal risk of pregnancy is not prohibitively high in NYHA class I–II patients, provided ventricular function is good.26 Ventricular failure and arrhythmia are the main causes of maternal morbidity. Care must be taken to maintain filling pressures during labour and delivery, avoiding dehydration and vasodilation.
The risks to the fetus include:
high (30%) risk of fetal loss
maternal drugs:
–warfarin should be converted to low molecular weight heparin
–antiarrhythmic drugs such as amiodarone may need to be continued; the risk of uncontrolled arrhythmia may outweigh the fetal risks of amiodarone.
Cyanotic heart disease in the absence of pulmonary hypertension
Women with complex cyanotic heart disease and low or normal pulmonary artery pressures do not carry the prohibitively high risk of death of the Eisenmenger syndrome patient with pulmonary hypertension.
Maternal risk for such patients depends largely on ventricular function. Other risks are:
haemorrhage: impaired clotting factors and platelet function
paradoxical embolism: all cyanotic patients shunt right to left
heart failure: precipitated by the additional volume load of pregnancy on an already volume loaded ventricle
increasing cyanosis: caused by the vasodilation of pregnancy.
The major risks to the fetus are fetal loss, low birthweight, and prematurity related to maternal cyanosis and maternal haemodynamic decompensation. If pre-pregnancy maternal oxygen saturation is < 85%, the chance of a livebirth is only 12%, compared with 92% if the oxygen saturation is > 90%.27 Prolonged admission for bed rest is an effective method of maintaining maternal oxygen saturation and hence fetal oxygenation.
Although spontaneous normal vaginal delivery is safest for the mother, in practice fetal problems often necessitate an elective section. Care must be taken to achieve meticulous haemostasis, maintain good hydration, and to avoid vasodilation (for example, with high dose epidural) and air emboli through venous lines.
Pulmonary hypertension and the Eisenmenger syndrome
Pulmonary hypertension of any cause carries a high risk of maternal death even if pulmonary artery pressures are 50% systemic.1,28 The risk of death for a patient with Eisenmenger syndrome is 40–50%, unchanged in the last four decades.29
Patients should be advised against pregnancy. Laparoscopic sterilisation may be considered, but carries a significant risk. The progesterone subdermal implant (Implanon) carries no cardiovascular risk and is at least as effective as sterilisation.
In the event of pregnancy, therapeutic termination should be offered. For those who elect to continue, admission for rest and treatment of right heart failure may be necessary. Treatment may include heparin, oxygen, prostacyclin, and nitric oxide, but there is no evidence that any intervention reduces mortality. The high risk of death continues for at least two weeks postpartum and may be sudden or with irreversible hypoxia.
Tachyarrhythmia
Many women with a normal heart experience palpitation during pregnancy and treatment is rarely necessary. For those with structural abnormalities, the increased sympathetic drive of pregnancy often worsens arrhythmia; if possible they should be established on an antiarrhythmic without fetal effects pre-pregnancy. In practice this is often difficult and some patients with refractory arrhythmia need to continue potentially toxic drugs such as amiodarone, balancing the risk to the fetus from the drug against the risk to both the mother and the fetus of an arrhythmia with haemodynamic compromise. Adenosine, verapamil, and DC cardioversion are safe for both mother and fetus.
CONCLUSION
The population of pregnant women with heart disease has changed in recent decades, with rheumatic disease becoming uncommon and complex CHD increasing. Cardiomyopathy and pulmonary hypertension continue to account for most maternal deaths.
As the number and complexity of adults survivors of CHD continue to grow, cardiologists and obstetricians need to be able to manage safely the majority of women who can tolerate a pregnancy and be able to recognise those few in whom a pregnancy is very high risk. Collaboration between cardiologist and obstetrician should result in a fall in maternal deaths from conditions already diagnosed before pregnancy and ensure that CHD does not feature more prominently in the next UK analysis of maternal deaths.
REFERENCES
Linked Articles
- Miscellanea
- Miscellanea
- Miscellanea
- Miscellanea
- Miscellanea