

Introduction
Dyspnea, the sensation of difficult or labored breathing, is the most common symptom in chronic obstructive pulmonary disease (COPD) and the primary symptom that limits physical activity in more advanced disease.1 According to the American Thoracic Society, dyspnea may be measured according to 3 domains2:
what breathing feels like for the patient
how distressed the patient feels when breathing
how dyspnea affects functional ability, employment, health-related quality of life, or health status.
Several studies have shown that patients find dyspnea and other COPD symptoms most cumbersome in the early morning and at night-time.3,4 However, symptoms can often be underreported by patients.5 The impact of COPD symptoms manifests in various aspects of patients’ day-to-day lives, perhaps none more significantly than in the context of physical activity. Inability to engage in sustained physical activity is a common feature of COPD, and even in cases of mild COPD, activity restriction can be evident.6 An estimated 29% to 44% of patients with COPD report persistent and troublesome activity-related dyspnea, which may occur early in the disease course.6,7 While a number of factors are thought to contribute to the reduced physical activity observed in COPD patients, dyspnea has been identified as a primary contributor.8 Patients with COPD may enter a downward spiral of dyspnea-induced inactivity, resulting in muscular and aerobic deconditioning (FIGURE 1),9,10 which, in turn, results in an increased unwillingness to attempt activity in the future.11

The dyspnea spiral10
As disease severity increases, breathlessness becomes more disabling at lower activity levels. These changes further impact the quality of life of patients, and can lead to anxiety and depression.11
Physical inactivity is often considered to be a major contributor to the progression of COPD,6 and is linked to hospitalizations and increased all-cause mortality.12 There is therefore a need to recognize symptoms early and treat them accordingly.
The relationship between lung hyperinflation and dyspnea in COPD
In COPD, pathologic changes give rise to physiologic abnormalities such as mucus hypersecretion and ciliary dysfunction, gas exchange abnormalities, pulmonary hypertension, and airflow limitation and lung hyperinflation.13 Lung hyperinflation, an increase in resting functional residual volume above a normal level, represents a mechanical link between the characteristic expiratory airflow impairment, dyspnea, and physical activity limitation in COPD.1
The lungs of patients with COPD can be hyperinflated both at rest (static hyperinflation) and/or during exercise (dynamic hyperinflation).14 Static hyperinflation is caused by a decrease in elasticity of the lung due to emphysema, resulting in decreased lung recoil pressure and a higher resting lung volume.15 In dynamic hyperinflation (FIGURE 2),15,16 the lungs operate at progressively higher volumes of air with each breath, approaching total lung capacity (TLC); this is made worse during exertion as the respiratory rate increases, allowing less time for exhalation.17 As a result, the volume of air taken in on each breath becomes more limited by higher end-expiratory lung volumes, and the “work” of breathing is increased.17

Changes in operational lung volumes shown as ventilation increases in (A) healthy individuals and (B) patients with COPD16
Although patients can compensate for several of the negative consequences of hyperinflation (eg, altering the chest wall due to overdistended lungs), such compensatory mechanisms are unable to cope with large increases in ventilation, such as those that occur during exercise.1 Air trapping, together with ineffectiveness of respiratory muscle function, leads to increased ventilation requirements and dynamic pulmonary hyperinflation, resulting in dyspnea.1
Patients with COPD describe a sensation of “air hunger,” reporting “unsatisfied” or “unrewarded” inhalation, “shallow breathing,” and a feeling that they “cannot get a deep breath,”18 whereas, in fact, they are limited in their ability to fully exhale. Verbal descriptors (eg, “air hunger” or “chest tightness”) are important tools in understanding a patient’s experience with dyspnea, and a patient’s choice of descriptor may be related to dyspnea severity, and the level of distress that dyspnea causes a given patient.19 Air hunger in turn encourages faster breathing, leading to further shortness of breath and more dynamic hyperinflation.1,20
To deflate the lungs of patients with COPD, physiologic, pharmacologic, and possibly surgical interventions are required:
Controlled breathing techniques (eg, purse-lipped breathing) that encourage slow and deep breathing can correct abnormal chest wall motion, decrease the work of breathing, increase breathing efficiency, and improve the distribution of ventilation to empty the lungs.21
Bronchodilators can help to achieve lung deflation by improving ventilatory mechanics, as shown by increases in inspiratory capacity and vital capacity.22
Lung volume reduction surgery can also be considered to treat severe hyperinflation in emphysematous patients5; bronchoscopic interventions that lower lung volumes are also in development.23
The impact of lung hyperinflation and dyspnea on physical activity in COPD
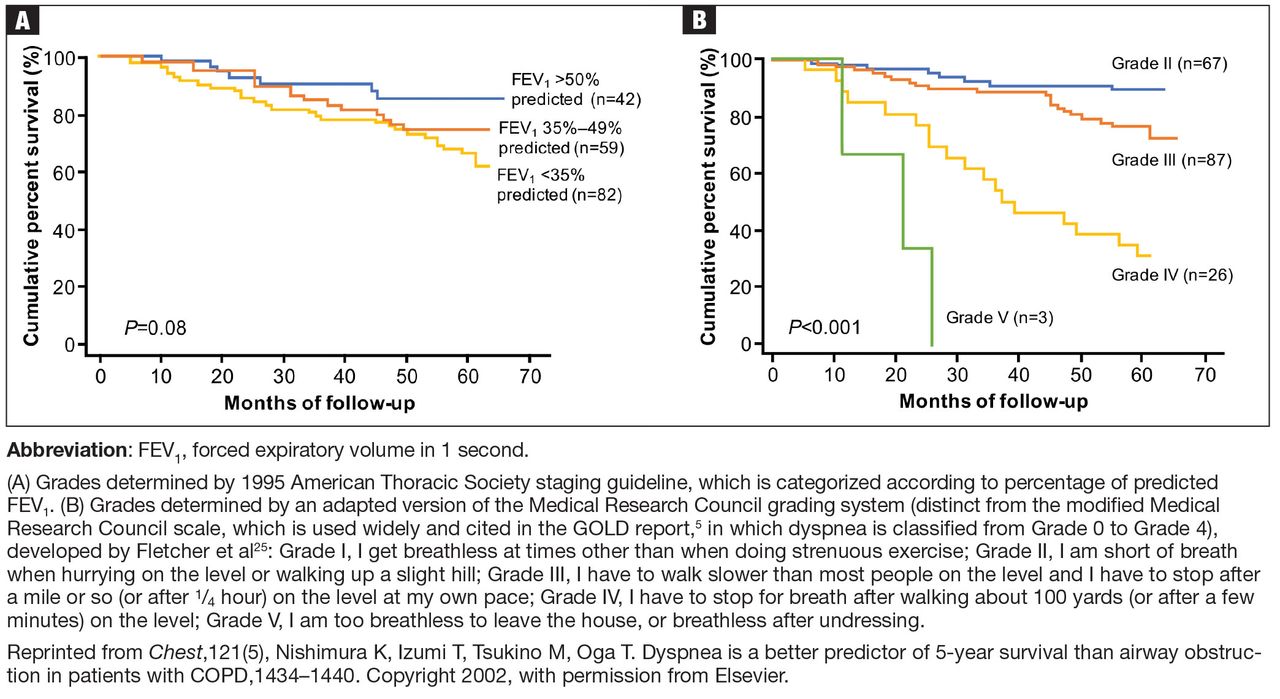
Dynamic hyperinflation can develop early in COPD, when patients generally experience dyspnea only during more intense exertion.11,22 However, as COPD progresses and airflow limitation increases, patients begin to experience shortness of breath with minimal effort and, eventually, during activities of daily living (ADLs), or even at rest.5,11 It is important that dyspnea, as well as airway obstruction, is considered as a variable that affects mortality in patients with COPD. Categorizing patients with COPD based on dyspnea severity has been shown to be a more effective predictor of mortality than using classifications based on percentage of predicted forced expiratory volume in 1 second (FEV1) (FIGURE 3).24 Similarly, inspiratory capacity (IC), a surrogate measure of hyperinflation, shows better correlation with exercise endurance time than FEV1.26 Resting IC, measured as the IC/TLC ratio (which is approximately 60% in healthy individuals27) has also been identified as an independent risk factor for mortality in patients with COPD28; in their study, Casanova et al examined the predictive capacity of various IC/TLC ratios, ranging from 15% to 40%, and found that an IC/TLC threshold of 25% provided the best power to predict mortality in patients with COPD.28

Five-year survival according to (A) percentage of predicted FEV and (B) dyspnea level24
Dyspnea and hyperinflation are closely interrelated with physical activity limitation,16,29,30 and so can be viewed as significant contributors to patient disability. During an acute exacerbation, patients with COPD will experience worsening airway obstruction, dynamic hyperinflation, and dyspnea.31 Patients with a greater number of comorbid conditions may also have greater shortness of breath.32 In addition, patients with COPD and hyperinflation perform less physical activity than individuals without hyperinflation, regardless of COPD severity, as assessed using the 2007 Global Initiative for Chronic Obstructive Lung Disease (GOLD) staging (stage I, mild; stage II, moderate; stage III, severe; stage IV, very severe) and BODE (Body-mass index, airflow Obstruction, Dyspnea, and Exercise) index.33 These patients also exhibit increases in dyspnea perception during commonly performed ADLs, which may limit physical activity and worsen lung hyperinflation.33 More limited physical activity also contributes to higher dyspnea scores during ADLs.8
Furthermore, the ability to perform typical ADLs may be significantly altered or eliminated altogether in patients with COPD.11 Leisure activities are often the first to be dropped by patients, as they generally require greater effort than simpler tasks, and are not critical to daily life.11 Eventually, these activities become progressively more difficult, and most patients with moderate or severe COPD can struggle to complete even the most basic daily activities.11
In addition to the morbidity burden and impact on ADLs, lower levels of physical activity in patients with COPD have also been shown to increase the risk of mortality and exacerbations, and elevate the risk of comorbidities such as heart disease and metabolic disease.34 In light of these observations, improving exercise capacity should be a key goal in COPD management.
Assessment and measurement of dyspnea and hyperinflation
Reducing hyperinflation and dyspnea is essential for improving physical activity endurance and overall physical activity in patients with COPD; therefore, measuring the degree of impairment is important.22 Clinicians should be aware that some patients may have relief of dyspnea due to improvements in hyperinflation, despite relatively mild changes in FEV1.35 Lung volume measures, including total lung capacity, residual volume and functional residual capacity, are valuable tools in the assessment of lung hyperinflation in COPD, and therefore constitute a key component of pulmonary function testing.36 However, expanded pulmonary function testing may be required for patients with severe dyspnea that does not correspond to spirometric findings, or cases in which diagnosis is uncertain.37
Lung volumes are evaluated primarily by body plethysmography, during which a patient sits inside an airtight “body box” equipped to measure pressure and volume changes.14,38 Helium dilution and nitrogen washing can also be used to measure functional residual capacity in patients with COPD,14 but body plethysmography is considered to be a more accurate method of lung volume evaluation in patients with severe airflow obstruction.14,38 Radiographic techniques can also be used, but due to a lack of standardization, they are not typically utilized in clinical practice.14 Measurement of IC may complement other lung volume measures as part of assessment of hyperinflation.16 This can be measured using either spirometry or body plethysmography.39,40
In addition to evaluating hyperinflation, ADLs, physical activity, exercise capacity, and dyspnea should all be assessed in patients with COPD in primary care. It is known that patients may self-limit ADLs to avoid symptoms of COPD; in doing so, worsening symptoms may be underappreciated, and subsequently underreported, by the patient. Th us, it is essential that physicians ask patients with COPD, as well as individuals at risk of COPD, questions about changes in their physical activity or ability to perform common tasks. There are a number of methods to measure functional performance, but for a simple assessment of ADLs, clinicians can ask the patient or caregiver questions related to basic daily tasks.11 In early COPD, patients who experience mild dyspnea during exercise should be able to perform most productive activities. Patients with stable COPD and moderate dyspnea during exercise should be able to carry out most of the higher functioning ADLs, whereas patients with severe COPD may struggle to complete basic ADLs without assistance.11 It should be noted, however, that patients may experience dyspnea with fairly routine activities, and even reduce physical activity at relatively early stages of airflow limitation.41,42
There is a clear distinction between symptom assessment tools that should be used, and which of these can be used practically in primary care. Although family physicians rarely perform spirometry or measure lung volumes in the clinic, it is important to highlight that spirometry assessment is conducted by some primary care practitioners, and should be utilized more readily in primary care to provide reinforcement of diagnoses. Similarly, the St. George’s Respiratory Questionnaire and the Chronic Respiratory Questionnaire, which are widely used in the scientific literature to assess symptoms, are generally considered to be too time-consuming for use in routine clinical practice5; the Transition Dyspnea Index is similarly lengthy.43 However, shorter measures, such as the COPD Assessment Test (CAT) and the COPD Control Questionnaire are suitable,5 with the CAT score representing the best available tool for primary care physicians to evaluate COPD symptoms (TABLE 1). The International Primary Care Respiratory Group Research Subcommittee was set up to provide guidance on the best measures of quality of life in COPD.44 The committee scored the CAT, COPD Control Questionnaire, and Chronic Respiratory Questionnaire highly for a primary care population.44 An additional tool often useful in clinical practice is the Medical Research Council (MRC) Dyspnea Scale,5 but it is important to note that this measure does not provide information on any symptoms other than dyspnea.
Other tests may be useful in assessing the impact of an intervention, be it pharmacologic or nonpharmacologic, on dyspnea severity. For example, increases in the 6-minute-walk distance (6MWD) have been shown to correlate with improvements in dyspnea.46 The 6MWD has also been shown to be an important predictor of hospitalization and mortality in patients with COPD.47 However, it is important to note that improvements in 6MWD show only a very weak correlation with patient-reported outcomes,48 and may be a less sensitive measure for patients with less disability than those with more profound functional limitation.49 Moreover, 6MWD can be affected by a patient’s psychologic motivation,6,50 as well as other comorbidities observed in patients with COPD, such as osteoporosis, heart failure, and peripheral vascular disease.46,51 Although not used for COPD diagnosis or evaluation of dyspnea or physical activity limitation, a chest X-ray can also be a useful tool for excluding alternative diagnoses, as well as for detecting significant comorbidities in patients with COPD, such as concomitant respiratory, cardiac, and skeletal diseases.5
Management of dyspnea and hyperinflation in primary care
Physicians can utilize a variety of pharmacologic and nonpharmacologic strategies to reduce hyperinflation and dyspnea and improve physical activity in patients with COPD (FIGURE 4).34

{kind=link}
{kind=link}
{kind=link}
{kind=link}
The crucial role of daily activity in patients with COPD34
Pulmonary rehabilitation is a tailored intervention that encompasses exercise training, education, and self-management support for people with chronic respiratory disease, based on detailed assessment of their exercise capacity and symptoms.52 Pulmonary rehabilitation is as important as medication in COPD management, providing a cost-effective intervention with minimal adverse effects.53 Moreover, pulmonary rehabilitation has been shown to benefit patients with mild to severe dyspnea (as classified according to the Medical Research Council dyspnea scale), demonstrating the value of successful execution of these programs in patients with COPD, irrespective of disease severity.54 Although the most significant improvements in patient quality of life are observed when a multimodality approach is used, exercise and proper pulmonary rehabilitation programs have been shown to improve quality of life more than medication alone.5,55 Notably, there are few supporting data for the use of supplemental oxygen in patients experiencing dyspnea without hypoxemia. Oxygen supplementation is only of minimal benefit to relieving the sensation of dyspnea.56,57
The relationship between the impact of pulmonary rehabilitation in patients with COPD and frailty scores has also been evaluated. Frailty scores are calculated based on an individual’s level of physical activity, and other key criteria that are indicative of their ability to self-manage their medical condition.58 These scores are particularly relevant in the context of COPD, given the high prevalence of the condition in older people.58 Although frailty is a strong independent predictor of noncompletion of pulmonary rehabilitation, completion of a pulmonary rehabilitation program in patients who are frail has been shown to reverse their frailty in the short term.58 It is therefore important that physicians guide and encourage these patients for the duration of a pulmonary rehabilitation program, from initiation through to completion, to ensure that those who are likely to derive the greatest benefit from pulmonary rehabilitation are supported to do so.
In addition to pulmonary rehabilitation, other nonpharmacologic interventions have emerged in recent years that may help to relieve dyspnea in patients with COPD. Airway clearance devices, such as acapella (Smiths Medical; Minneapolis, MN), Flutter (Allergan; Dublin, Ireland), Lung Flute (Medical Acoustics; Buffalo, NY), Quake (Thayer Medical; Tucson, AZ), and Aerobika (Monaghan Medical; Plattsburgh, NY) promote the clearance of sputum through the application of positive expiratory pressure, possibly allowing medicines to penetrate the lungs more effectively, and improving diffuse airflow obstruction.59–61 Incorporating an airway clearance device into a bronchodilator therapy regimen has been shown to improve dyspnea scores, both before and after exercise, compared with bronchodilator therapy combined with a nonfunctional control device in patients with severe COPD.59 In addition, noninvasive forms of ventilation, such as continuous positive airway pressure and bi-level positive airway pressure (BiPAP), have been shown to effectively reduce dyspnea in patients with COPD.62,63 In a 24-month study in patients with severe COPD, resting dyspnea improved significantly in patients using the BiPAP Auto-Trak (Philips Respironics, Best, The Netherlands) in conjunction with their regular bronchodilator therapy, compared with those receiving long-term oxygen therapy in addition to their typical therapeutic regimen.63 Further studies are required to establish the impact of these devices in the management of dyspnea and other symptoms of COPD.
These nonpharmacologic interventions can be supplemented with pharmacologic treatments to help patients achieve their treatment goals of improved dyspnea and increased exercise performance. Bronchodilators, which form the basis of various COPD treatment options, include5:
short-acting muscarinic antagonists (SAMAs), such as ipratropium
short-acting β2-agonists (SABAs), such as albuterol, levalbuterol, and terbutaline
SAMA/SABA combinations
LAMAs, such as aclidinium, glycopyrrolate, tiotropium, and umeclidinium
long-acting β2-agonists (LABAs), such as arformoterol, indacaterol, formoterol, olodaterol, salmeterol, and vilanterol
LAMA/LABA combinations (umeclidinium/vilanterol, tiotropium/olodaterol, glycopyrrolate/formoterol, glycopyrrolate/indacaterol)
Inhaled corticosteroids can also be used in a fixed-dose combination with a LABA, which can be combined with a LAMA, in select patients5; however, these combination products may have minimal value in treating dyspnea unless asthma is concomitantly present.5,64 Further discussion of the different treatment options available for patients with COPD can be found in the final article of this supplement.
In addition to improving quality of life, long-acting bronchodilators, such as LAMAs, LABAs, and LAMA/LABA combinations, increase expiratory flow, reduce dynamic hyperinflation, and improve exercise capacity of patients.65–67 As disease severity worsens, physicians may opt for long-acting bronchodilator options that have twice-daily dosing, which may confer a benefit in improving night-time symptom control.68
As well as active pharmacologic and nonpharmacologic interventions, physicians should always encourage smoking cessation in patients with COPD, as this has the greatest capacity to influence the natural course of the disease.5 It is essential that health care providers continually deliver smoking cessation messages to patients with COPD; patients can also be supported to stop smoking by using nicotine replacement therapy, pharmacologic interventions, attending smoking cessation programs, and counseling.5
Lung volume reduction surgery may also be considered as a strategy for the management of dyspnea in severe, refrac tory COPD.69 Similarly, nonsurgical bronchoscopic interventions are being developed that look to achieve similar results to lung volume reduction surgery, including endobronchial one-way valves, lung volume reduction coils, airway bypasses, adhesives, and vapor therapy.23
Conclusions
Dyspnea, the most common symptom of COPD and the primary consequence of the condition’s characteristic lung hyperinflation, is a heavy burden on the lives of patients. The impact of dyspnea is perhaps most apparent in the context of physical activity, with activity limitation observed frequently in patients with COPD, regardless of disease stage. This can affect patients’ quality of life significantly, and has long-term consequences on disease progression. Improving dyspnea and increasing exercise endurance should therefore be a key goal for COPD management, which should encompass both nonpharmacologic interventions, such as pulmonary rehabilitation, and pharmacologic interventions, such as use of bronchodilator therapy.
Footnotes
DISCLOSURES
Dr. Marchetti has no conflicts of interest.
Dr. Kaplan has been a speaker or an advisory board member for AstraZeneca; Becton, Dickinson and Company; Boehringer Ingelheim, GmbH; GlaxoSmithKline; Johnson & Johnson; Mylan Laboratories Inc.; Paladin Labs Inc.; Pfizer Inc.; Purdue Pharma L.P.; Novartis Pharmaceuticals Corporation; and Trudell Medical International.
Funding for this article was provided by AstraZeneca LP (Wilmington, DE, USA). Medical writing support was provided by Hannah Burke, BSc, of Core (London, UK) and editorial support was provided by Maryam Vahdat, PGDip, of Core (London, UK), which were funded by AstraZeneca LP (Wilmington, DE, USA), in accordance with Good Publication Practice guidelines (Battisti WP et al. Ann Intern Med. 2015;163:461–464. doi: 10.7326/M15-0288).
This article is being co-published in The Journal of Family Practice and Cleveland Clinic Journal of Medicine.
- © 2019 The Cleveland Clinic Foundation. All Rights Reserved.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.
- 42.
- 43.
- 44.
- 45.
- 46.
- 47.
- 48.
- 49.
- 50.
- 51.
- 52.
- 53.
- 54.
- 55.
- 56.
- 57.
- 58.
- 59.
- 60.
- 61.
- 62.
- 63.
- 64.
- 65.
- 66.
- 67.
- 68.
- 69.