

A 57-year-old man was transferred to our hospital with leg pain and confusion. His family reported that he had injured his leg while launching a motorized personal watercraft at the North Carolina seashore 2 days before. He had a history of cirrhosis secondary to hepatitis C and alcohol abuse.
Physical examination revealed rashes on his legs with hemorrhagic bullous lesions and ecchymosis (Figure 1). He was hypotensive and had lactic acidosis, with blood lactate levels as high as 9.4 mmol/L (reference range 0.5–2.2 mmol/L). Despite aggressive hydration and broad-spectrum antibiotics provided at a previous hospital, he needed increasing vasopressor treatment.

Left leg: bullous lesions from Vibrio vulnificus infection.
Given his septicemia and recent marine exposure, Vibrio vulnificus infection was suspected, and antibiotics were switched to doxycycline and ceftazidime. He underwent urgent surgical debridement, ultimately requiring above-the-knee amputation of his right leg. He also required additional surgeries on his left leg.
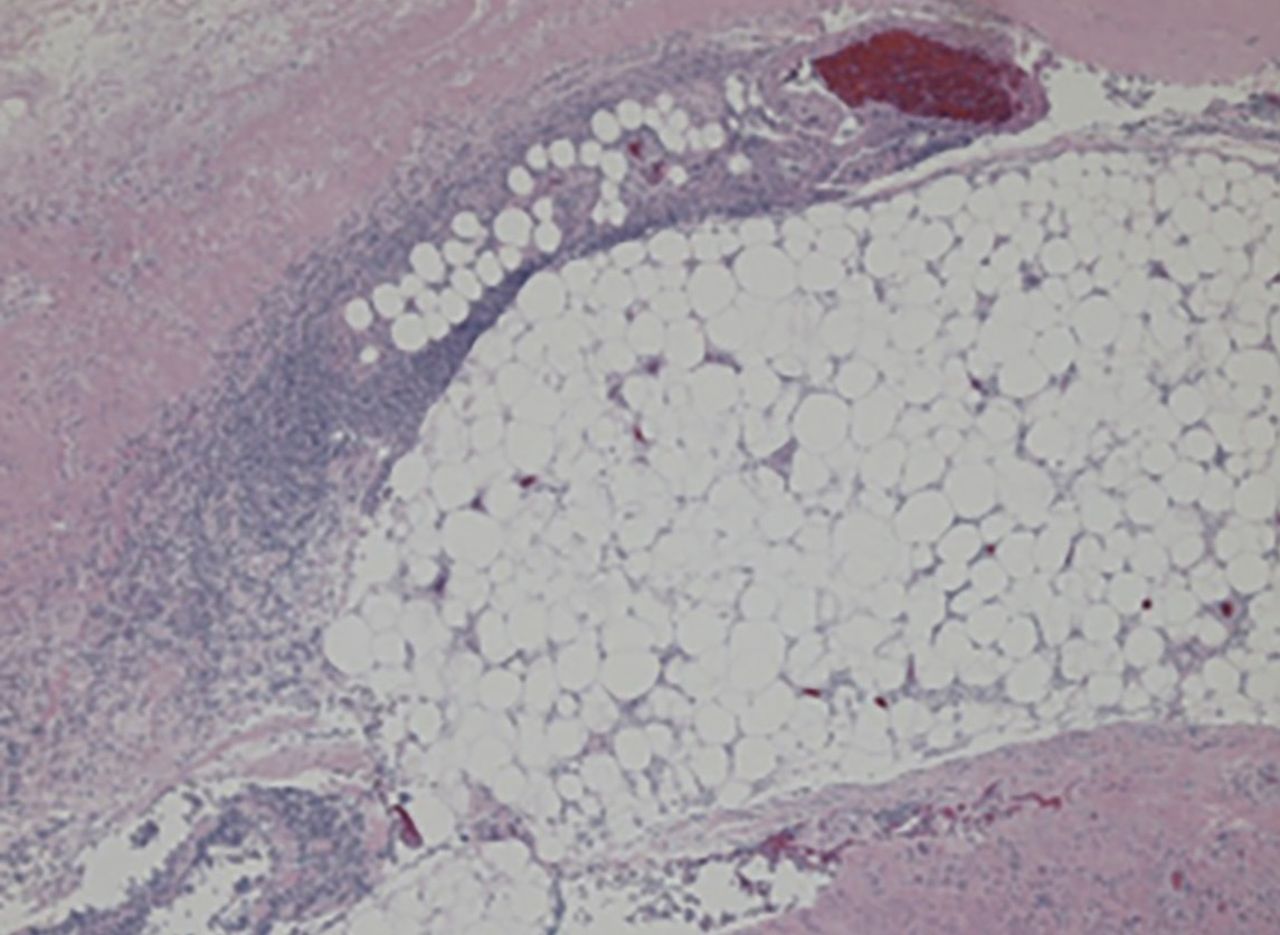
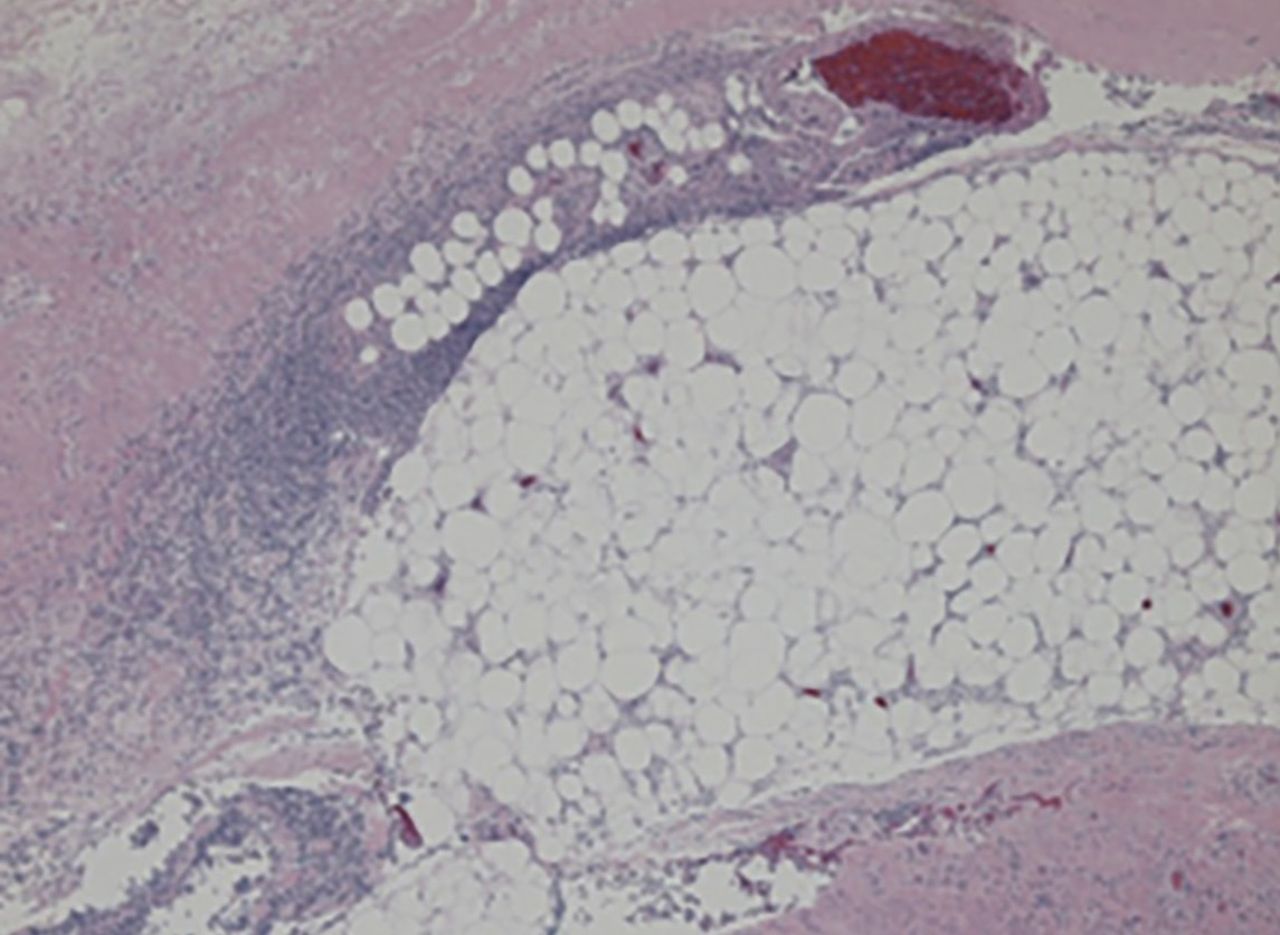
Blood and wound cultures eventually grew V vulnificus, and surgical pathology confirmed the diagnosis of necrotizing fasciitis (Figure 2).
{kind=link}
{kind=link}
Necrosis of deep dermis, subcutaneous fat, and fascial tissue with polymorphonuclear cell infiltration (hematoxylin and eosin, × 200).
RISE IN V VULNIFICUS INFECTIONS IS ATTRIBUTED TO GLOBAL WARMING
V vulnificus infection occurs most commonly from consuming raw shellfish, especially oysters, but it also occurs after exposure of an open wound to contaminated salt water. The pathogen is a gram-negative bacterium that resides in coastal waters worldwide, but in the United States it is usually seen on the Pacific and Gulf coasts1 during the summer.2
Although only 58 cases of V vulnificus infection were reported to the US Centers for Disease Control and Prevention in 1997, the number more than doubled to 124 in 2014.1 This rise is suspected to be due in part to warmer coastal waters associated with global warming.2
Various marine pathogens can cause wound infections, but V vulnificus is most commonly implicated in deaths and hospitalizations.2 Immunocompromised patients and those with liver disease are at particularly high risk of rapid progression to septic shock.
First-line antibiotics are doxycycline plus a third-generation cephalosporin.3 Studies have shown a direct correlation between delay of antibiotics and death,4 and early surgery is critical.5
Given the rising incidence of V vulnificus infection, it is increasingly important for providers across the United States to be aware of this infection.
- Copyright © 2018 The Cleveland Clinic Foundation. All Rights Reserved.