

A 79-year-old man with cortical cerebellar atrophy presented to the gastroenterology department with a 7-day history of progressive abdominal distention and constipation. He had a history of chronic constipation due to neurogenic bowel dysfunction. The dysfunction had been managed with laxatives.
On physical examination, his abdomen was distended and tender, and bowel sounds were absent. There was no fever, abdominal rigidity, or guarding.
‘COFFEE BEAN’ SIGN AND ‘WHIRL’ SIGN
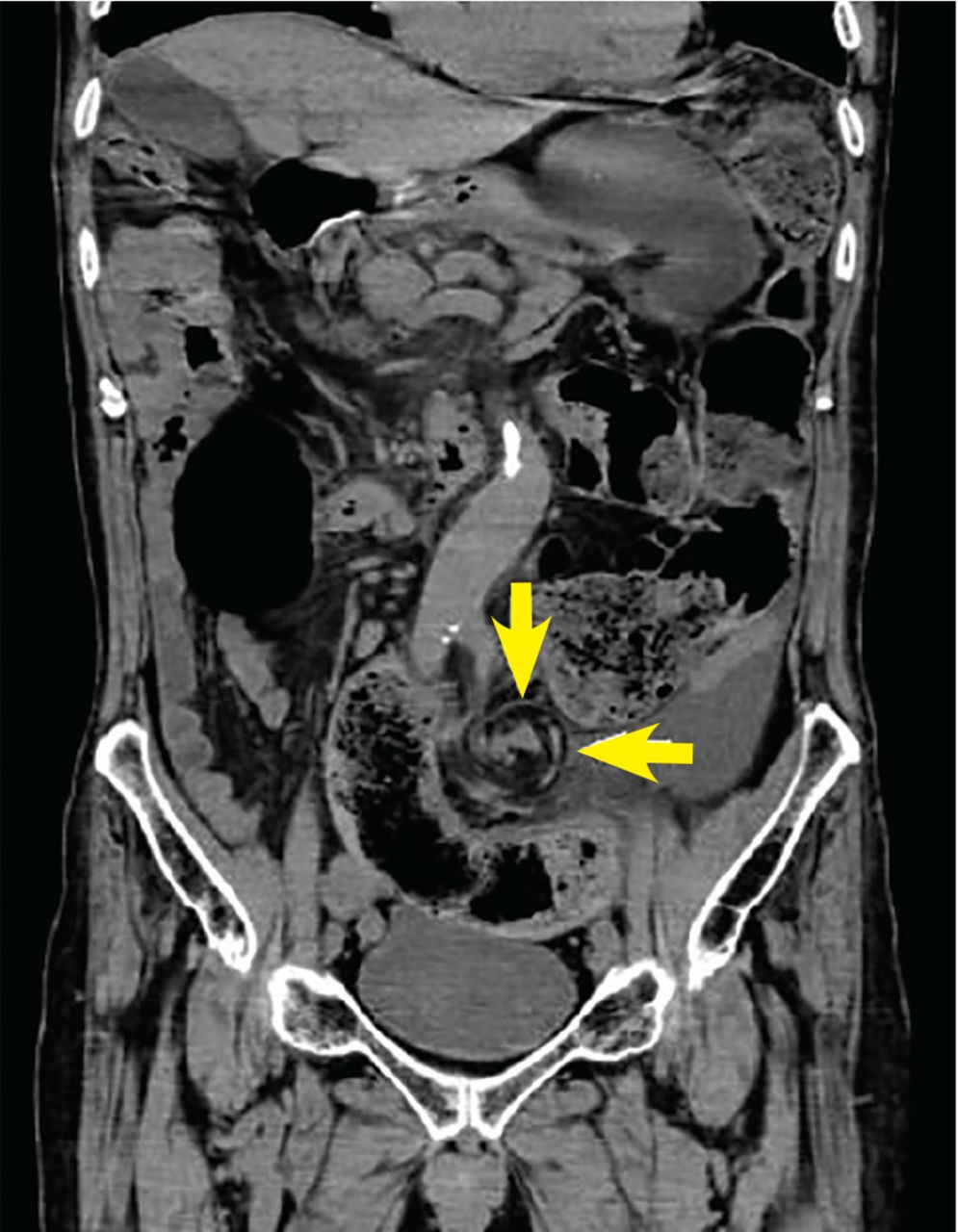
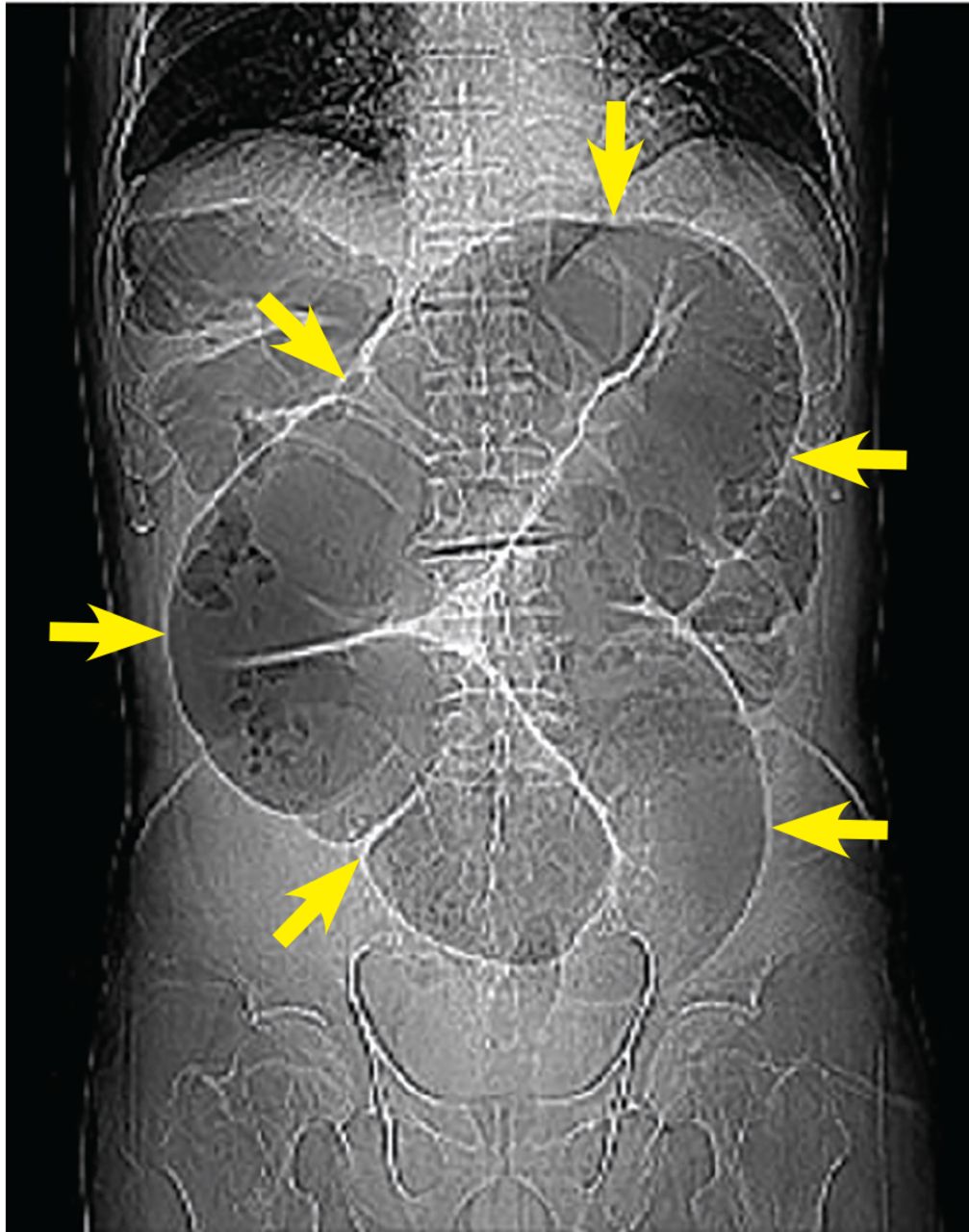
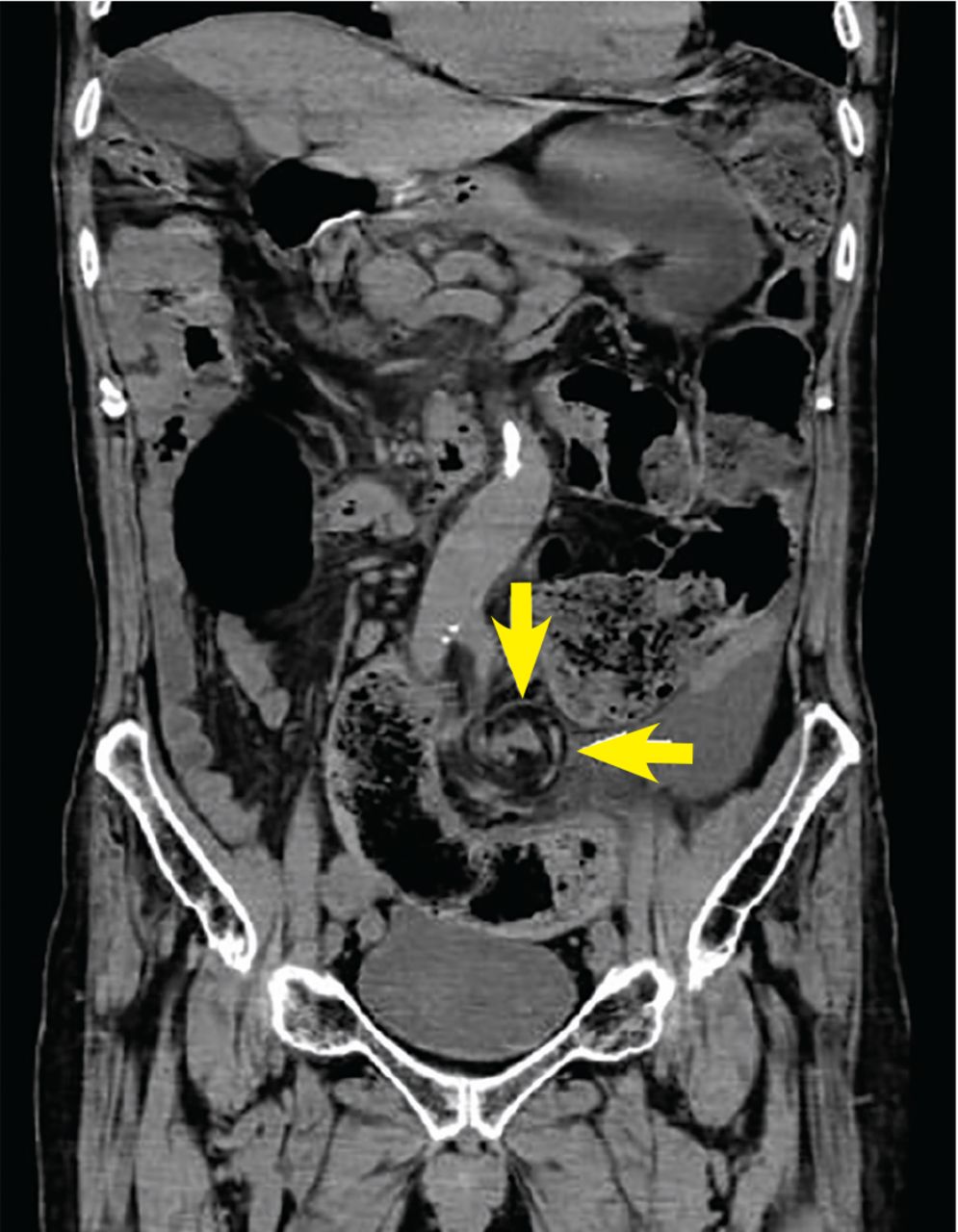
The preliminary view on abdominal computed tomography (CT) showed a distended sigmoid loop with an inverted U-shape, also known as the coffee bean sign, bent innertube sign, or kidney bean sign (Figure 1). This feature was also seen on plain abdominal radiography. In addition, the CT coronal view revealed the whirl sign, representing twisted bowel and mesentery (Figure 2). These findings were consistent with sigmoid volvulus.

Computed tomography preliminary view showed a distended sigmoid loop with an inverted U-shape (arrows), also known as the coffee bean sign.
{kind=link}
{kind=link}
Computed tomography coronal view showed the whirl sign, representing twisted bowel and mesentery (arrows).
Emergency endoscopy confirmed torsion of the sigmoid colon without mucosal ischemia or masses. The colonoscope was successfully passed through the volvulus and into the dilated colon, resulting in reduction of the volvulus.
SIGMOID VOLVULUS
Sigmoid volvulus is the third most common cause of bowel obstruction after cancer and diverticulitis.1 Risk factors include chronic constipation, diabetes mellitus, neurologic disorders, and previous abdominal surgery.2 The classic clinical presentation is a triad of abdominal pain, distention, and constipation.3
Sigmoid volvulus is potentially life-threatening, and early diagnosis and treatment are essential. Endoscopic procedures such as decompression and reduction are the emergency treatments of choice in uncomplicated acute sigmoid volvulus.2 Flexible sigmoidoscopy or even rigid proctoscopy is usually used as nonoperative treatment; colonoscopy is not necessarily needed for decompression.
Emergency surgery is an option only when nonoperative treatment is unsuccessful, or in patients with perforation, bowel infarction, or peritonitis.2,4
Because of the high recurrence rate after endoscopic treatment, elective surgery is recommended to reduce morbidity and mortality risk.4
- Copyright © 2020 The Cleveland Clinic Foundation. All Rights Reserved.