

A 25-year-old man presented with sudden onset of left flank pain upon standing up from a chair 3 weeks after undergoing renal biopsy. The procedure had been an ultrasonographically guided percutaneous renal biopsy of the lower pole of the left kidney, with 3 passes, to evaluate hematuria and nephritic-range proteinuria and had resulted in the diagnosis of immunoglobulin A (IgA) nephropathy.
The patient had a history of hypertension, for which he was taking nifedipine 40 mg daily, which had been keeping his blood pressure below 130/80 mm Hg. As an infant he had had congenital hydrocephalus, for which a ventriculoperitoneal shunt had been placed.
On examination, his blood pressure was elevated at 160/80 mm Hg; other vital signs were stable. Abdominal examination revealed left flank tenderness and left costovertebral angle tenderness. The rest of the physical examination was unremarkable.
His blood urea nitrogen level was 13 mg/dL (reference range 8–20), and his serum creatinine was 1.40 mg/dL, up from 1.20 mg/dL before the biopsy (reference range 0.65–1.07). His electrolyte levels, liver function test results, and complete blood cell counts were normal.
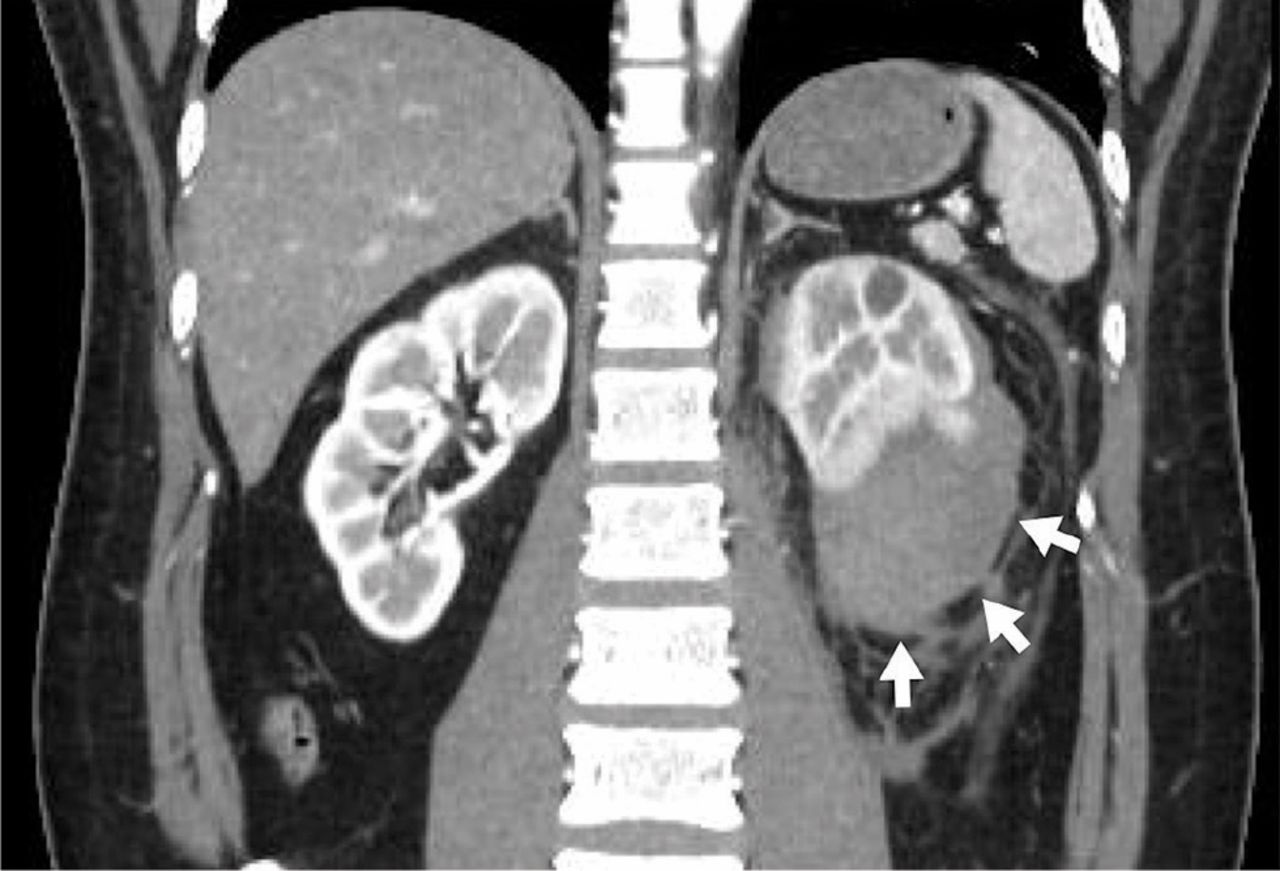
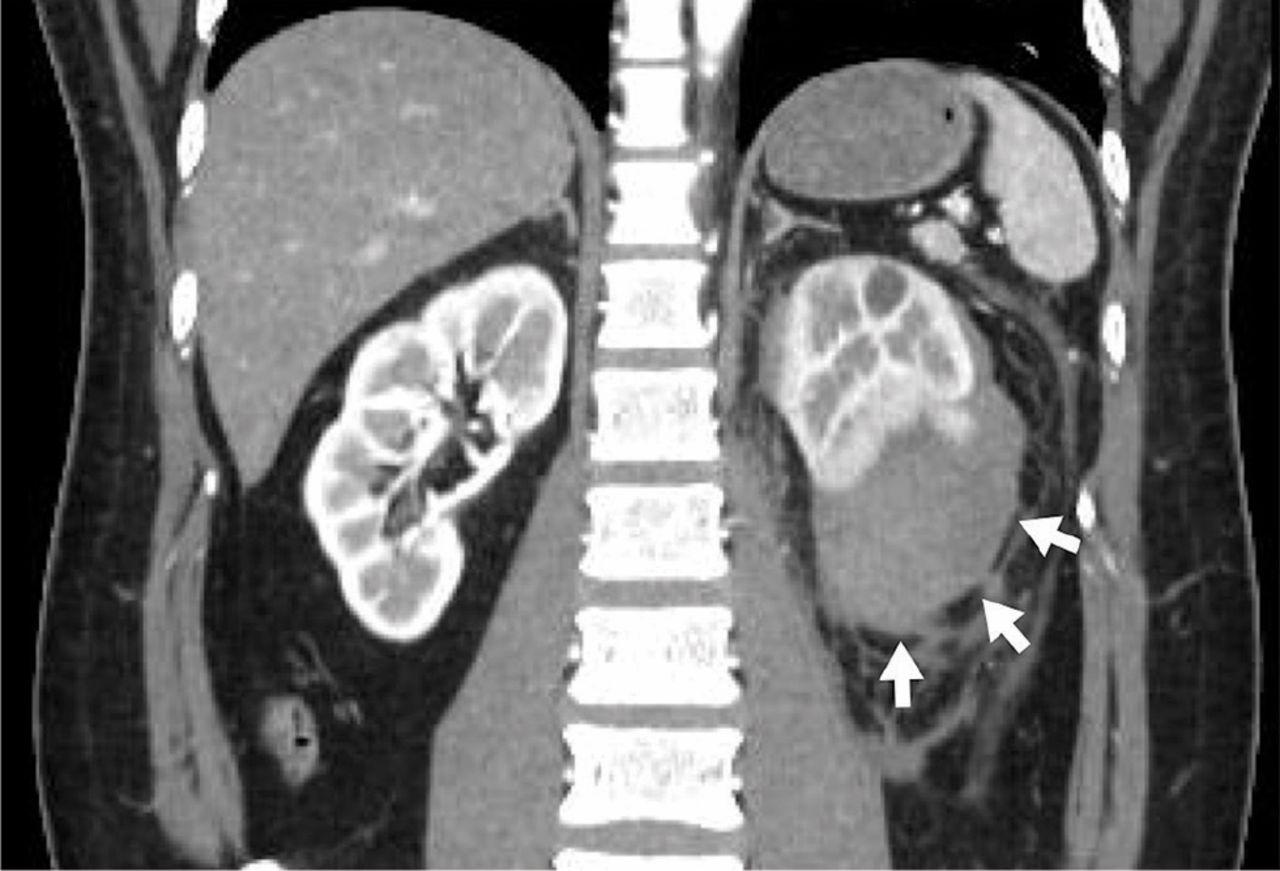
Computed tomography (CT) with contrast revealed a large pericapsular collection with high attenuation (70 Hounsfield units [HU]) in the left kidney, compressing the renal parenchyma (Figures 1 and 2).

Axial computed tomography with contrast of the mid-kidney shows that the renal parenchyma is compressed by a contained, high-attenuation (70 HU), pericapsular collection (arrowheads).
{kind=link}
{kind=link}
Coronal computed tomography with contrast shows that the lower pole is compressed by a contained, high-attenuation, pericapsular collection (arrows).
In view of his worsening hypertension and the pericapsular hematoma in his left kidney, we suspected Page kidney as a complication of renal biopsy.
Two days after admission, his creatinine level had increased to 2.75 mg/dL. Four days after admission, his plasma renin activity was elevated to 11 μg/L/hour (reference range 0.3–2.9) and his serum aldosterone level was 337 pg/mL (reference range 29.9–159), establishing the diagnosis of Page kidney.
Intravenous nicardipine and fentanyl were given. Although his pain subsided significantly, his blood pressure remained high. Renin-angiotensin-aldosterone system (RAAS) inhibitors were initially deferred in view of his acute kidney injury, and nicardipine was continued.
The patient subsequently underwent laparoscopic evacuation of the hematoma. Afterward, CT confirmed that the hematoma was gone, but his kidney function did not improve. Therefore, 6 days after admission, enalapril 2.5 mg daily was added to his regimen, and his blood pressure returned to normal over the next several days. One month later, his serum creatinine level was down to 1.28 mg/dL, his plasma renin activity was 0.3 μg/L/hour, and his aldosterone level was 59.7 pg/mL.
PAGE KIDNEY
Page kidney, a condition in which an affected kidney is compressed by external force, is an uncommon cause of secondary hypertension and renal insufficiency. Other possible causes of secondary hypertension include renal artery stenosis, juxtaglomerular cell tumor, and malignant hypertension.
Page kidney was first reported in 1939 by Irvine Page,1 who induced it in a dog by wrapping the animal’s kidney in cellophane. The presumed mechanism is that direct external compression of the kidney causes decreased renal perfusion and increased renin secretion, resulting in activation of the RAAS system and secondary hypertension.2
The most common cause of constrictive pressure on the kidney is hematoma due to abdominal trauma, surgery, or percutaneous interventions. Page kidney has often been reported after traumatic biopsy of kidney allografts, but more rarely after native kidney biopsy.
Ultrasonography and CT are useful for detecting hematoma.
As activation of the RAAS is the central mechanism of hypertension in Page kidney, we deemed it suitable to give enalapril, a drug that blocks the RAAS, and nicardipine, a calcium channel blocker, to control hypertension and prevent further kidney damage. However, few studies have investigated optimal antihypertensive therapy in Page kidney. Percutaneous or open drainage of the hematoma may be needed for patients with uncontrolled hypertension or worsening renal function. Surgical nephrectomy is occasionally required to control hypertension.3
Page kidney should be considered in a patient with new-onset hypertension and flank pain after native kidney biopsy. Early recognition can allow for conservative treatment, which can improve this condition and preserve kidney function.4
Acknowledgment
The authors thank Dr. Rita McGill for editing this article.
- Copyright © 2020 The Cleveland Clinic Foundation. All Rights Reserved.