

A 70-year-old woman was admitted for epigastric pain and generalized skin eruptions. Three months before admission, she was on chemotherapy for acute lymphocytic leukemia.
She had a history of herpes zoster and was vaccinated against varicella. She was taking 2 nonsteroidal anti-inflammatory drugs (NSAIDs), loxoprofen and celecoxib, for chronic back pain caused by degenerative lumbar spondylosis.
On hospital day 1, she described the epigastric pain as of gradual onset, intermittent, and crampy. She reported no odynophagia . Eruptions appeared on her head on day 6. The NSAIDs were discontinued on suspicion of NSAID-related gastritis, and a proton pump inhibitor was administered. However, the epigastric pain worsened, and the eruptions spread to the trunk.
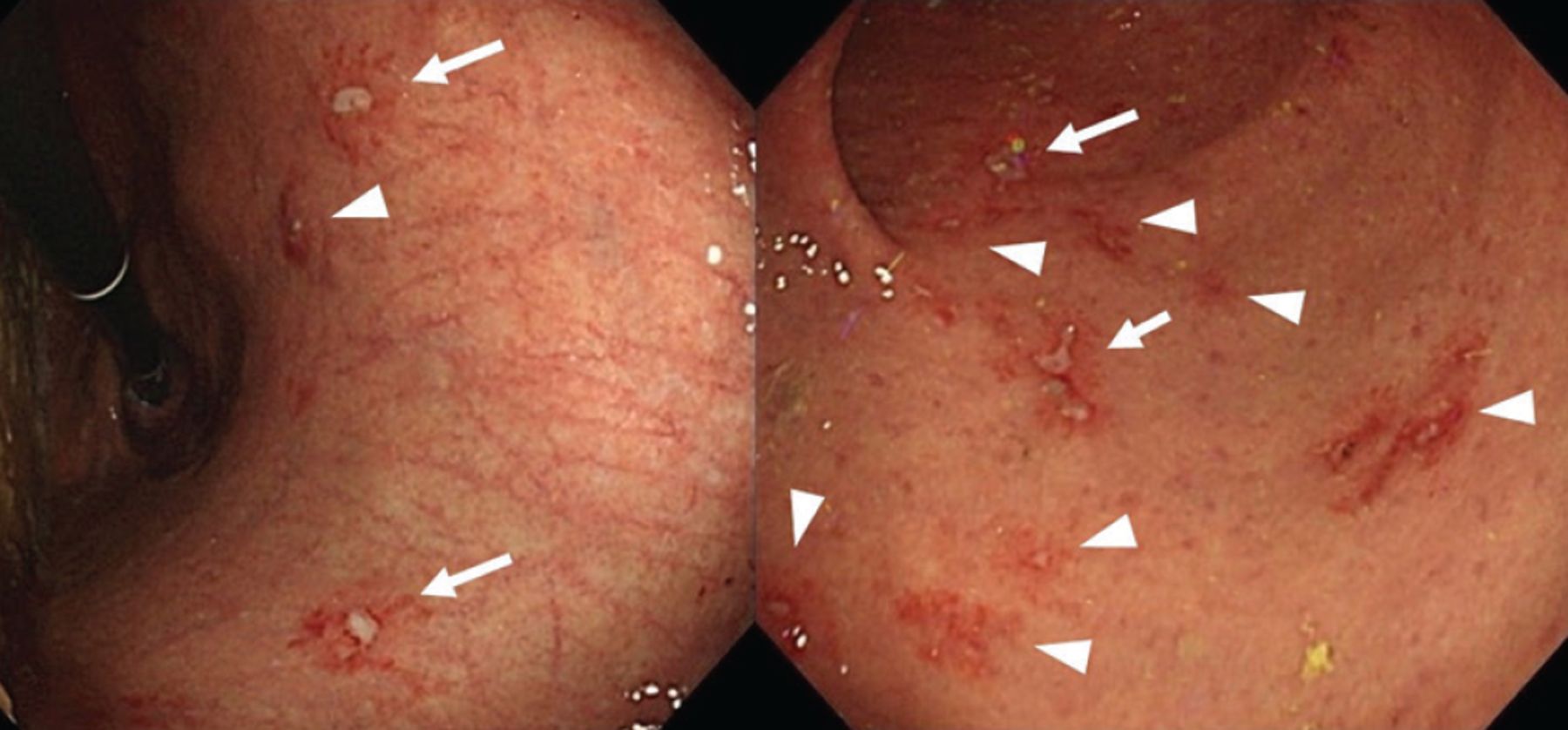
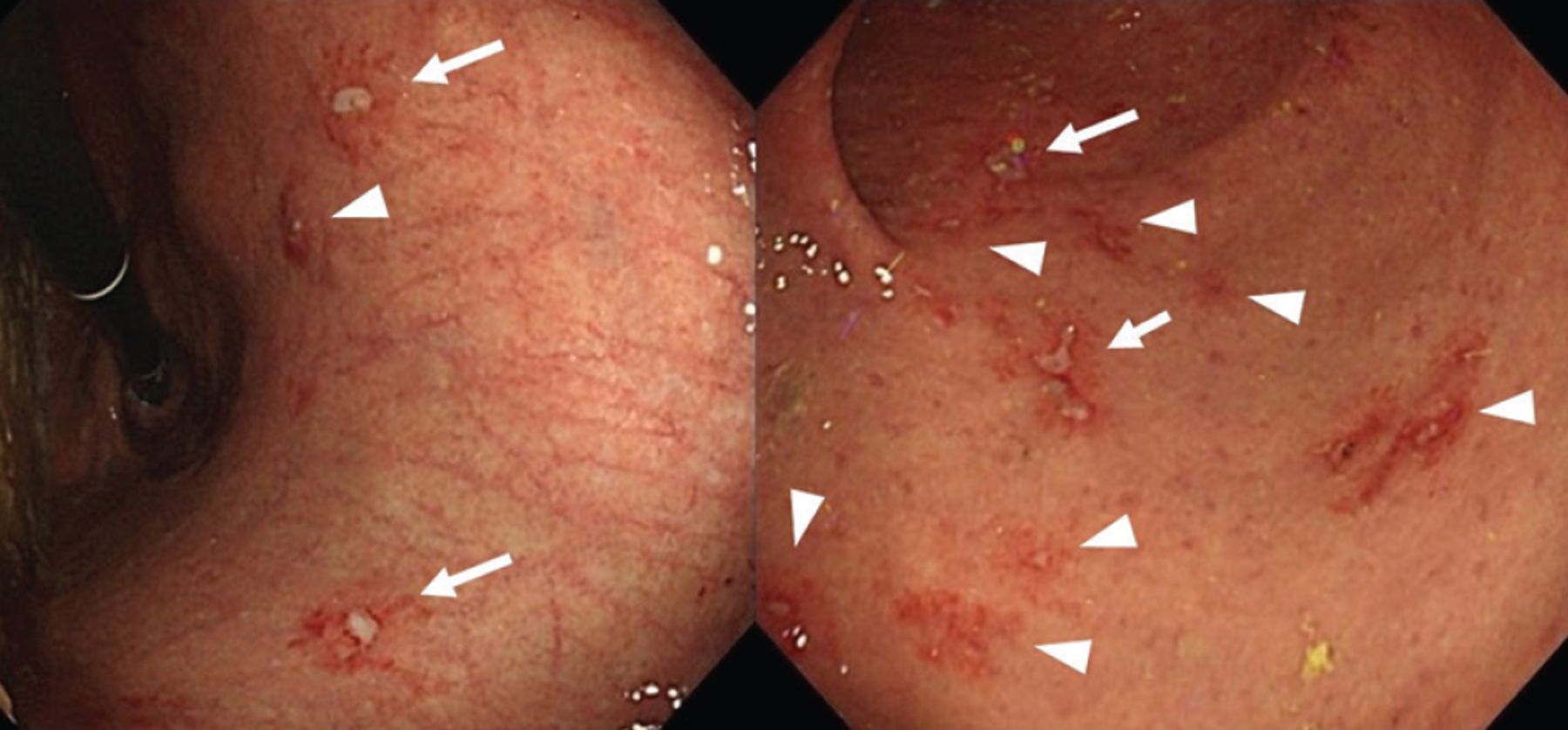
On day 11, partly hemorrhagic vesicles of various sizes with red haloes were observed on her entire body (Figure 1). With a tentative diagnosis of varicella, intravenous acyclovir 250 mg every 8 hour was initiated. Varicella-zoster virus (VZV) antigen was detected from the vesicular lesions via fluorescent antibody assay. On day 17, esophagogastroduodenoscopy showed small, shallow ulcers and erosions surrounded by red haloes, spread diffusely throughout the stomach and duodenum (Figure 2). No esophageal lesions were observed, and the mucosal biopsy was negative for gastric infiltration of acute lymphocytic leukemia. Immunostaining was negative for cytomegalovirus, and VZV-DNA was detected by polymerase chain reaction. She was diagnosed with gastrointestinal VZV infection. After 8 days of antiviral therapy, her symptoms improved, and she was discharged.

Hemorrhagic vesicles with red haloes of various sizes distributed over the whole body.
{kind=link}
{kind=link}
Esophagogastroduodenoscopy of the stomach showed small, shallow ulcers (arrows) and erosions (arrowheads) surrounded by red haloes spread diffusely in the stomach and duodenum.
RECOGNIZING RISK FOR GASTROINTESTINAL VZV
Gastrointestinal VZV infection should be considered in immunocompromised patients with a history of VZV infection presenting with abdominal pain. Visceral VZV infection is related to reactivation of the latent virus in the enteric nervous system.1 It occurs in 3% to 15% of immunocompromised patients with herpes zoster, with some developing gastrointestinal manifestations.2 In patients who have undergone bone marrow transplant, the risk factors include a highly immunosuppressed state, active graft-vs-host disease, and possibly a history of nondisseminated herpes zoster.
The mortality rate in patients with gastrointestinal VZV infection has been reported to range from 28.6% to 50% despite antiviral therapy.3,4 Although this patient had not undergone bone marrow transplant, the chemotherapy she had received was a potential predisposing factor.2 Esophagogastroduodenos copy should be considered in patients with these risk factors.
Suspicion of gastrointestinal VZV infection and prompt initiation of antiviral therapy are important when gastric ulcers similar to the skin lesions are present. With NSAID-related ulcers, multiple, irregularly shaped lesions are frequently observed in the gastric antrum.5 In contrast, VZV infection-related lesions present as multiple erosions disseminated in the stomach.6 Furthermore, the esophagus, duodenum (as observed in this patient), and the small and large intestines can be involved.7
It is also important to differentiate gastrointestinal VZV infection from gastrointestinal cytomegalovirus infection observed in immunocompromised patients. There has been no direct comparison of gastrointestinal VZV and cytomegalovirus. In one report, the endoscopic appearance of upper-gastrointestinal cytomegalovirus infection was variable and nonspecific, ranging from normal or minimally inflamed mucosa to deep ulceration.8 Therefore, it may be difficult to distinguish gastrointestinal VZV from cytomegalovirus infection based on endoscopic findings alone. However, in the case of gastrointestinal VZV infection, abdominal symptoms can precede the skin lesions by 1 to 10 days, and this more strongly supports VZV.2,3
In this patient, the epigastric pain that preceded the varicella-like skin eruptions, and the diffuse gastroduodenal erosions that resembled the skin lesions revealed on esophagogastroduodenoscopy led to the diagnosis. Treatment with acyclovir before obtaining the definitive diagnosis (by polymerase chain reaction testing) ameliorated the patient’s symptoms. Thus, clinicians should be vigilant for gastrointestinal VZV infection in patients with gastric ulcers and skin lesions.
DISCLOSURES
The authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
- Copyright © 2021 The Cleveland Clinic Foundation. All Rights Reserved.