

A 53-year-old man with a 2-month history of progressive pain and intermittent claudication of both lower extremities presented to the outpatient clinic. He was a smoker and had untreated diabetes mellitus, but he had no previous cardiovascular or gastrointestinal problems. He also denied any drug misuse, lead poisoning, ergotism, or abdominal injury.
His vital signs were normal. Physical examination revealed pallor of his toes, cold extremities, dry skin, and absence of bilateral femoral pulses. He also disclosed that he had erectile dysfunction.
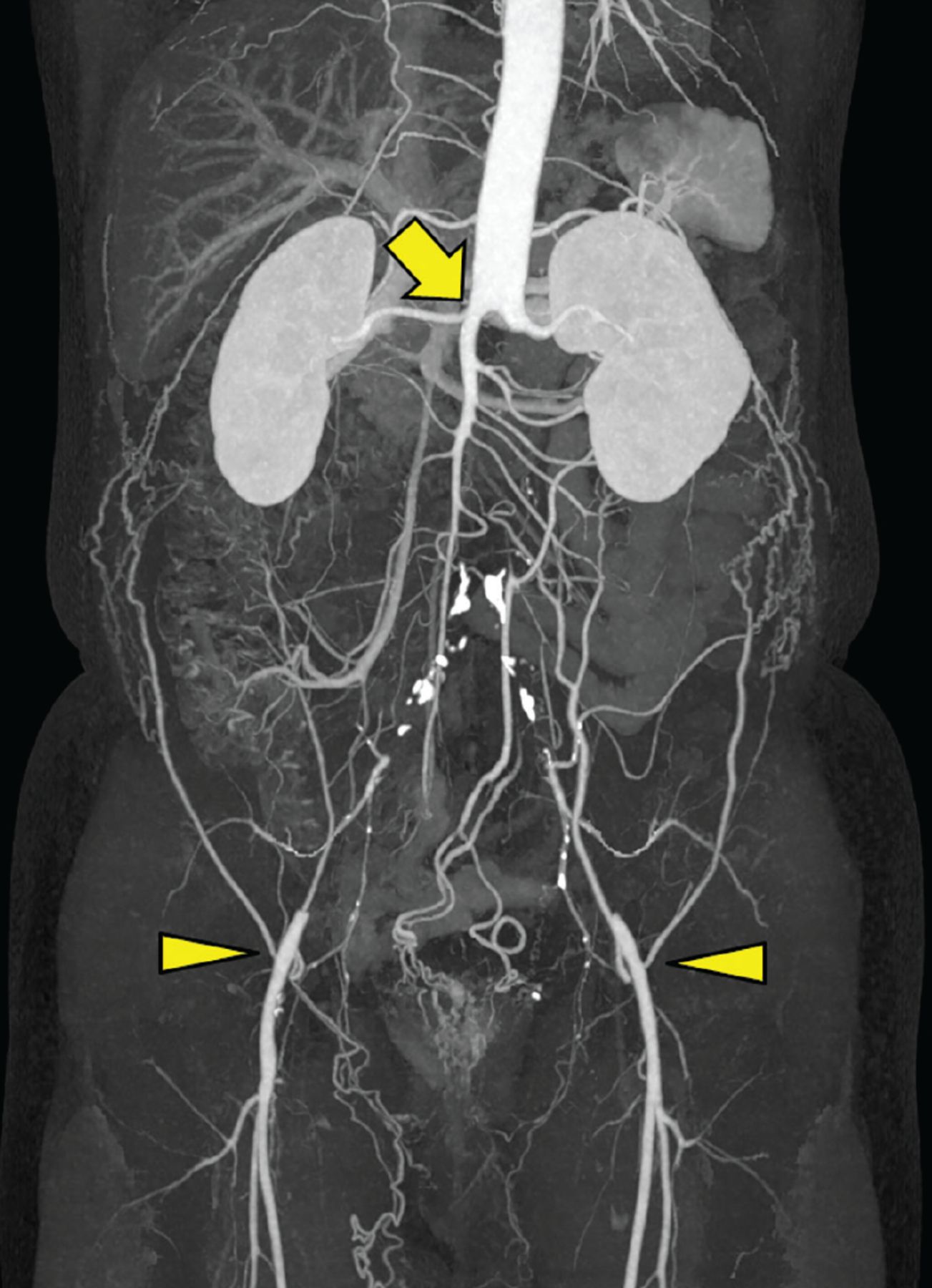
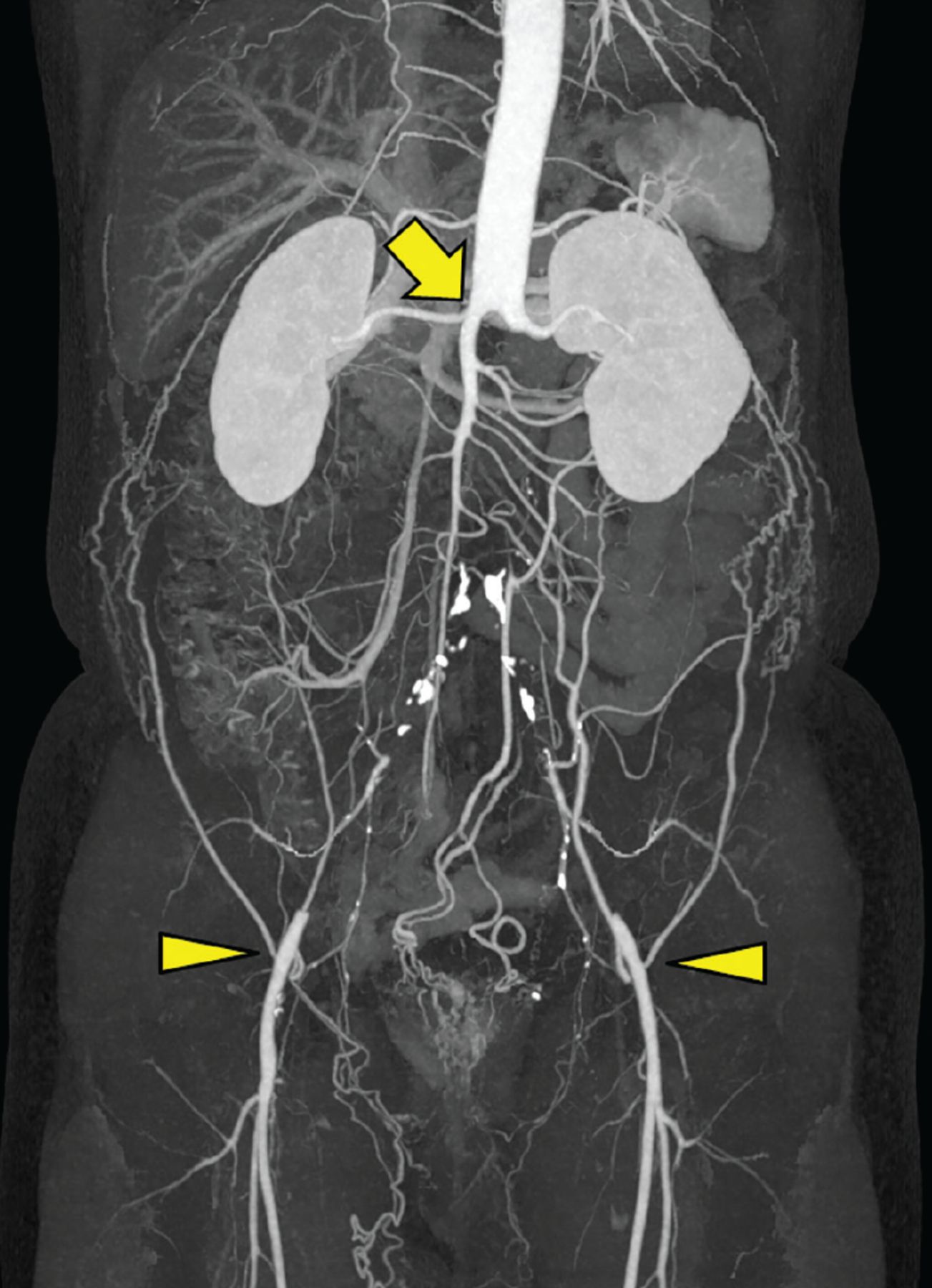
The ankle-brachial index was 0.28 on the right side and 0.47 on the left side, indicating severe bilateral vascular disease. Abdominal computed tomography with contrast enhancement revealed complete occlusion of the infrarenal abdominal aorta, with collateral pathways (Figure 1). Based on the clinical and radiographic findings, we made a diagnosis of aortoiliac occlusive disease, also called Leriche syndrome.
{kind=link}
Abdominal contrast-enhanced computed tomography showed complete occlusion of the infrarenal abdominal aorta (arrow). The collateral pathways provided blood flow to both external iliac arteries (arrowheads).
CLUES TO THE DIAGNOSIS
Leriche syndrome is a progressive disease that presents as a triad of claudication, erectile dysfunction, and decreased distal pulses. Risk factors are hypertension, diabetes mellitus, hyperlipidemia, and smoking. Some patients are asymptomatic because of sufficient collateral blood flow. Symptoms are often vague and include bilateral buttocks claudication, impotence, leg pain, pallor, and absent femoral pulses.
The differential diagnosis of Leriche syndrome includes abdominal aortic dissection, neuropathy, spinal canal stenosis, spinal disc herniation, and Guillain-Barré syndrome.1
Measuring the ankle-brachial index is a noninvasive and inexpensive part of the evaluation of suspected Leriche syndrome. Imaging with Doppler ultrasonography, aortic angiography, and computed tomographic angiography can aid in confirming the diagnosis and the location of stenosis.
TREATMENT
Treatments for Leriche syndrome are aortobifemoral bypass, aortoiliac endarterectomy, extra-anatomic bypass grafting, and endovascular bypass.2
Medical management to prevent progression of the disease should target hyperlipidemia, diabetes mellitus, and hyperglycemia, and smoking cessation is also important.3 Our patient quit smoking and was treated with aspirin and a statin.
Untreated Leriche syndrome is progressive and results in serious complications. Thus, early identification is essential.
DISCLOSURES
The authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
- Copyright © 2021 The Cleveland Clinic Foundation. All Rights Reserved.