

ABSTRACT
Alpha-gal syndrome is an emerging condition characterized by an immunoglobulin (Ig) E–mediated reaction to galactose-alpha-1,3-galactose (alpha-gal) after consumption of mammalian-derived food products. Identified in the early 2000s, the syndrome is linked to sensitization through tick bites; in the United States, the lone star tick (Amblyomma americanum) is the main vector. Symptoms range from pruritus and hives to severe systemic reactions like anaphylaxis, and typically occur 3 to 8 hours after eating meat. Diagnosis involves a history of consistent symptoms, positive alpha-gal IgE serology, and dietary exclusion trials. Management focuses on avoiding foods and products that contain alpha-gal and preventing tick bites.
Alpha-gal syndrome should be considered when a patient from a region where lone star ticks are prevalent has unexplained gastrointestinal symptoms and a history of a recent tick bite and meat consumption.
Reactions can vary among patients and are influenced by exogenous and endogenous factors.
The characteristic delayed reaction makes an oral food challenge difficult for routine clinical practice, but it can be considered if serologic testing is unclear.
There is no cure, but avoiding alpha-gal exposure and future tick bites can lead to symptom resolution.
A 37-year-old woman from Virginia with a history of asthma presents with hives and diarrhea. She reports that 1 week prior, she experienced generalized pruritus, cramping abdominal pain, and diarrhea 3 hours after having a beefsteak for dinner. After a visit to urgent care, diphenhydramine 25 mg and dicyclomine 20 mg 4 times daily provided symptomatic relief. Notably, she reports having had a similar episode at night 1 month earlier but does not recall eating red meat that day. She notes that she is an avid hiker and has a history of several spider and tick bites.
Laboratory tests show a serum galactose-alpha-1,3-galactose (alpha-gal) immunoglobulin (Ig) E level of 41.2 kU/L (reference < 0.1 kU/L) and a total IgE level of 475 kU/L (< 130 kU/L). A presumed diagnosis of alpha-gal syndrome is made.
The patient is advised to abstain from eating mammalian meat. She reports another episode of abdominal pain after having a milkshake, despite adhering to a non–mammalian meat diet. She is advised to avoid consuming dairy products. After following an elimination diet for 3 years, her alpha-gal IgE level declines from 41.2 kU/L to 0.82 kU/L.
Because of the gradual decline in alpha-gal IgE levels, an oral challenge with 100 grams of ground beef is performed in the clinic. After 5 hours of observation, the patient remains asymptomatic. Due to a successful oral challenge, she resumes consuming mammalian meat and does not have any further reactions.
WHAT IS ALPHA-GAL SYNDROME?
Alpha-gal syndrome, also known as alpha-gal allergy, mammalian meat allergy, or tick-bite–related meat allergy, is an emerging allergic condition that triggers IgE-mediated anaphylaxis, gastrointestinal symptoms or skin reactions, or both, a few hours after an affected person consumes mammalian meat, such as beef, pork, goat, rabbit, venison, or lamb, or mammalian-derived products.1 Another phenotype, gastrointestinal alpha-gal syndrome, presents with symptoms such as abdominal pain, diarrhea, and nausea or vomiting, but without any skin, respiratory, or circulatory complaints.
Alpha-gal syndrome mostly occurs in adults and was first identified in the early 2000s.2,3 Between 2010 and 2022, more than 100,000 cases of presumed alpha-gal syndrome were identified in the United States4; however, the exact prevalence of alpha-gal syndrome is unknown.
Many clinicians are not aware of alpha-gal syndrome. A nationwide survey of 1,500 healthcare professionals by the US Centers for Disease Control and Prevention showed that 42% were unaware of the condition, and 35% lacked confidence in diagnosing or treating patients with alpha-gal syndrome.5 Because cases continue to increase and symptoms overlap with other gastrointestinal illnesses and allergies, gastroenterologists and primary care clinicians must be aware of alpha-gal syndrome for timely diagnosis and intervention.
HOW TICK BITES CAN INDUCE A MEAT ALLERGY
Alpha-gal, the allergen identified in alpha-gal syndrome, is an oligosaccharide found in the cells and tissues of all nonprimate mammals. Sensitization to alpha-gal is thought to occur through parasitic infections, most commonly tick bites, when the immune system produces IgE antibodies directed against alpha-gal present in the parasite’s saliva.6,7 According to Commins et al,8 80% of patients with suspected alpha-gal syndrome report being bitten by ticks, and these individuals have higher alpha-gal IgE levels than those who have not been bitten.9
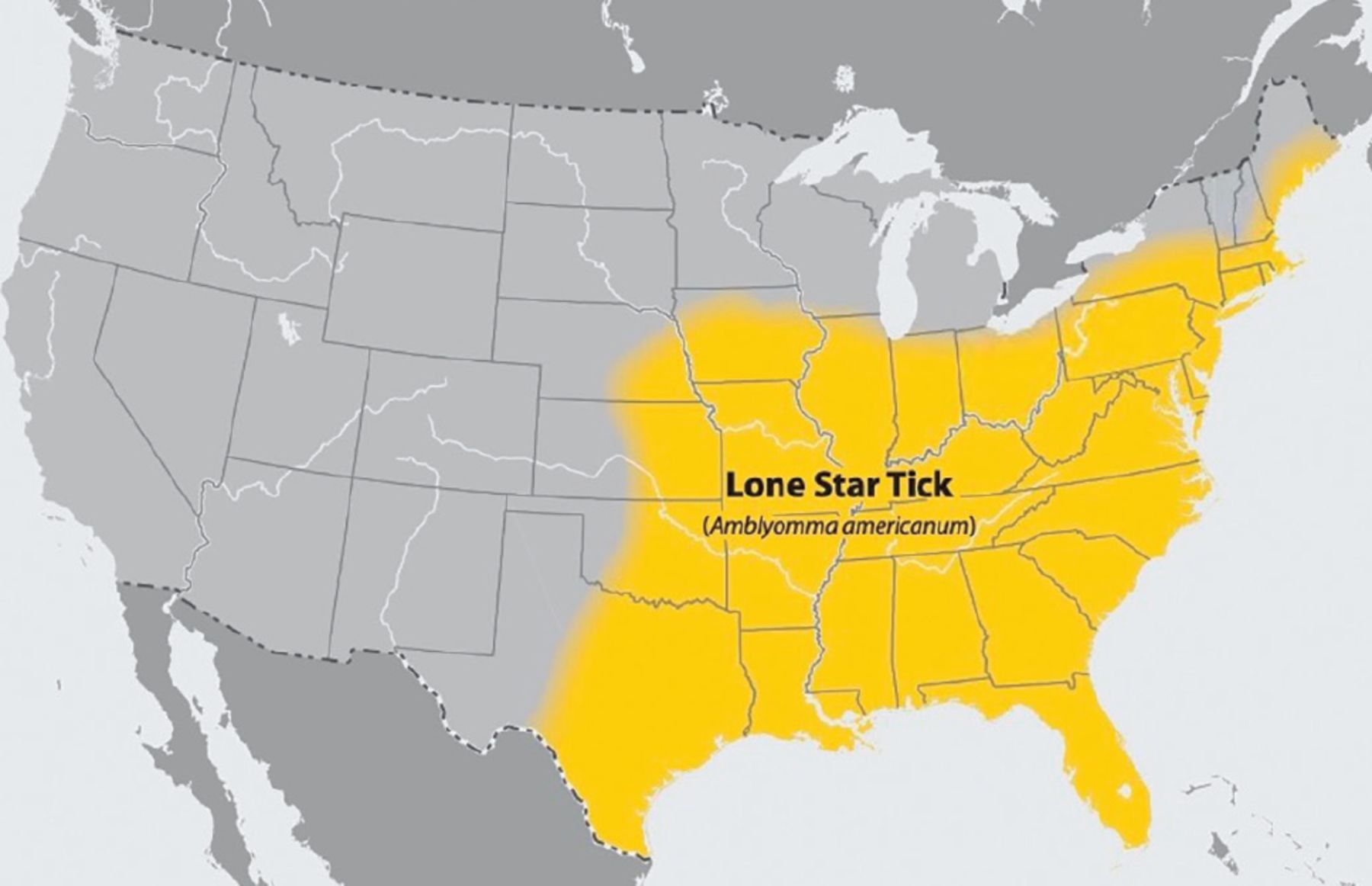
In the United States, the lone star tick (Amblyomma americanum; Figure 1), which primarily parasitizes deer and is responsible for 90% of all tick bites in the southern United States,3,10 has been identified as the vector responsible for alpha-gal syndrome.11 This tick is unique because it is the only tick that bites humans during its larval stage, positioning it as the primary source of alpha-gal sensitization in the United States.3 Other tick species that have been identified as carriers of alpha-gal in their saliva include the blacklegged tick (Ixodes scapularis), also known as the deer tick, in the United States; the Cayenne tick (Amblyomma cajennense) in Central America and Brazil; and the Asian long-horned tick (Haemaphysalis longicornis) in Asia.11–13

The lone star tick (Amblyomma americanum).
Reprinted from US Centers for Disease Control and Prevention. Lone Star Tick Surveillance. www.cdc.gov/ticks/data-research/facts-stats/lone-star-tick-surveillance.html.
Glycolipid hypothesis
Although the exact pathogenesis of alpha-gal syndrome is unknown, it involves IgE-mediated activation of mast cells after mammalian meat is consumed.13 The current “glycolipid hypothesis” describes the mechanism for the delay in response to ingestion of meat products containing alpha-gal and subsequent development of symptoms.
After individuals sensitized to alpha-gal consume mammalian meat or its derivatives, lipid micelles are formed from glycolipids containing alpha-gal.14 Enzymes in the small intestine, mainly pancreatic lipase, break down triglycerides within the micelles into free fatty acids, monoglycerides, and diglycerides, which are absorbed by intestinal cells. The intestinal epithelium then converts the fatty acids and monoglycerides into triglycerides and bundles them into lipoprotein particles, or chylomicrons, that display alpha-gal molecules. The chylomicrons enter the lymphatic system via lacteals and reach the bloodstream about 4 hours after a meal,1 where the alpha-gal molecules bind to alpha-gal–specific IgE antibodies on the surface of basophils or mast cells.14 This triggers an allergic reaction or anaphylaxis as mast cells release a cascade of allergic mediators, which stimulate sensory nerves, inducing visceral pain through the contraction of intestinal smooth muscles, and activate excessive mucous secretion by the mucous glands.3
RANGE OF SYMPTOMS AND TRIGGERS
Alpha-gal syndrome can present with various symptoms, and the intensity of symptoms can vary over time. Symptoms usually occur 3 to 8 hours after exposure to alpha-gal, but can also happen immediately.15 Common symptoms include pruritus, erythema, hives, and angioedema, or severe systemic manifestations such as anaphylaxis with cough, wheezing, shortness of breath, and hypotension.
In some instances, patients can have localized gastrointestinal symptoms. A recent study showed that, among 91 individuals with alpha-gal allergy, 40.7% experienced gastrointestinal symptoms exclusively.16 The predominant symptoms reported in the gastrointestinal phenotype are abdominal pain, nausea, vomiting, diarrhea, and heartburn.16–18 These patients are frequently misdiagnosed with functional gastrointestinal disorders, commonly irritable bowel syndrome, owing to both the lack of awareness of alpha-gal syndrome and the lack of testing for IgE antibodies to alpha-gal.1,3
Notably, most sensitized individuals do not experience any symptoms after ingesting mammalian meat.3 In regions where ticks are prevalent, 15% to 35% of the population may be sensitized to alpha-gal, but clinical alpha-gal syndrome occurs in only 1% to 8%.15 It is crucial to recognize that, even if a person is allergic to alpha-gal, reactions may not always occur after they consume mammalian meat,3 and a sensitized individual who has tolerated meat previously is still prone to allergic reactions in the future.
The likelihood and intensity of these reactions can be exacerbated by multiple exogenous and endogenous factors. Alcohol, nonsteroidal anti-inflammatory drugs, and exercise can enhance intestinal food absorption, potentially raising the concentration of alpha-gal allergens in the body and lowering the threshold for allergic reactions.13 Additionally, consuming fatty cuts of meat can enhance an allergic reaction because they contain higher levels of glycolipids containing alpha-gal.19,20 When digested, these fats form the alpha-gal–coated chylomicrons that can trigger allergic reactions by activating mast cells, as discussed above.
Individuals who have a personal or family history of food or insect allergies are more likely to have alpha-gal syndrome and experience more severe symptoms due to cross-reactivity between oligosaccharides. Those with blood type A or O are also at higher risk of developing alpha-gal syndrome.21
MEDICAL PRODUCTS THAT CONTAIN ALPHA-GAL CAN TRIGGER ALLERGIC REACTIONS
Medications and medical products containing alpha-gal may trigger reactions more frequently in patients with alpha-gal antibodies.22 Chung et al23 observed that antibodies to alpha-gal were present in patients with severe hypersensitivity to cetuximab, a therapeutic monoclonal antibody containing alpha-gal in the fragment antigen-binding portion of the heavy chain. (This led to the first observation of alpha-gal syndrome and its association with higher prevalence in regions where the lone star tick is located; see next section.)
The risk of reaction to other medical products that contain alpha-gal such as vaccines with gelatin (especially the live attenuated zoster vaccine), porcine-derived heparin or pancreatic enzymes, equine-derived antivenins, and bioprosthetic heart valves is not known, but cases of such reactions have been reported.24–28 Heparin products are well tolerated in 98.3% of patients with a documented alpha-gal allergy.26 On the other hand, positive skin prick tests to both antivenins and cetuximab have been seen in patients sensitized to alpha-gal, suggesting a potentially high risk of anaphylaxis with therapeutic doses of antivenin.29
Additionally, medical devices derived from animal materials, such as bioprosthetic cardiac valves, pose risks to those with alpha-gal sensitivity.27 Despite anecdotal evidence of hives and anaphylaxis after porcine or bovine valve replacement, conclusive research on valve failures due to alpha-gal reactions is lacking.25
The probability of a clinically significant reaction is relatively low and may be influenced by the animal source, processing methods, purity level, and administered dose, as well as the patient’s serum alpha-gal antibody titers.24,26,27,29
WHEN TO CONSIDER ALPHA-GAL SYNDROME
Patients should be tested for alpha-gal IgE antibodies if they are experiencing unexplained gastrointestinal symptoms that awaken them at night, as this reflects the characteristic delay from ingestion to reaction observed in individuals sensitized to alpha-gal.2 These patients may also report a history of tick bites and frequent engagement in outdoor activities. However, clinicians should be cautious about testing patients exhibiting “red flag” symptoms like anemia, gastrointestinal bleeding, or significant weight loss because these are not typically caused by alpha-gal syndrome.3 The presence of skin symptoms, including urticaria and angioedema, may also vary among patients.
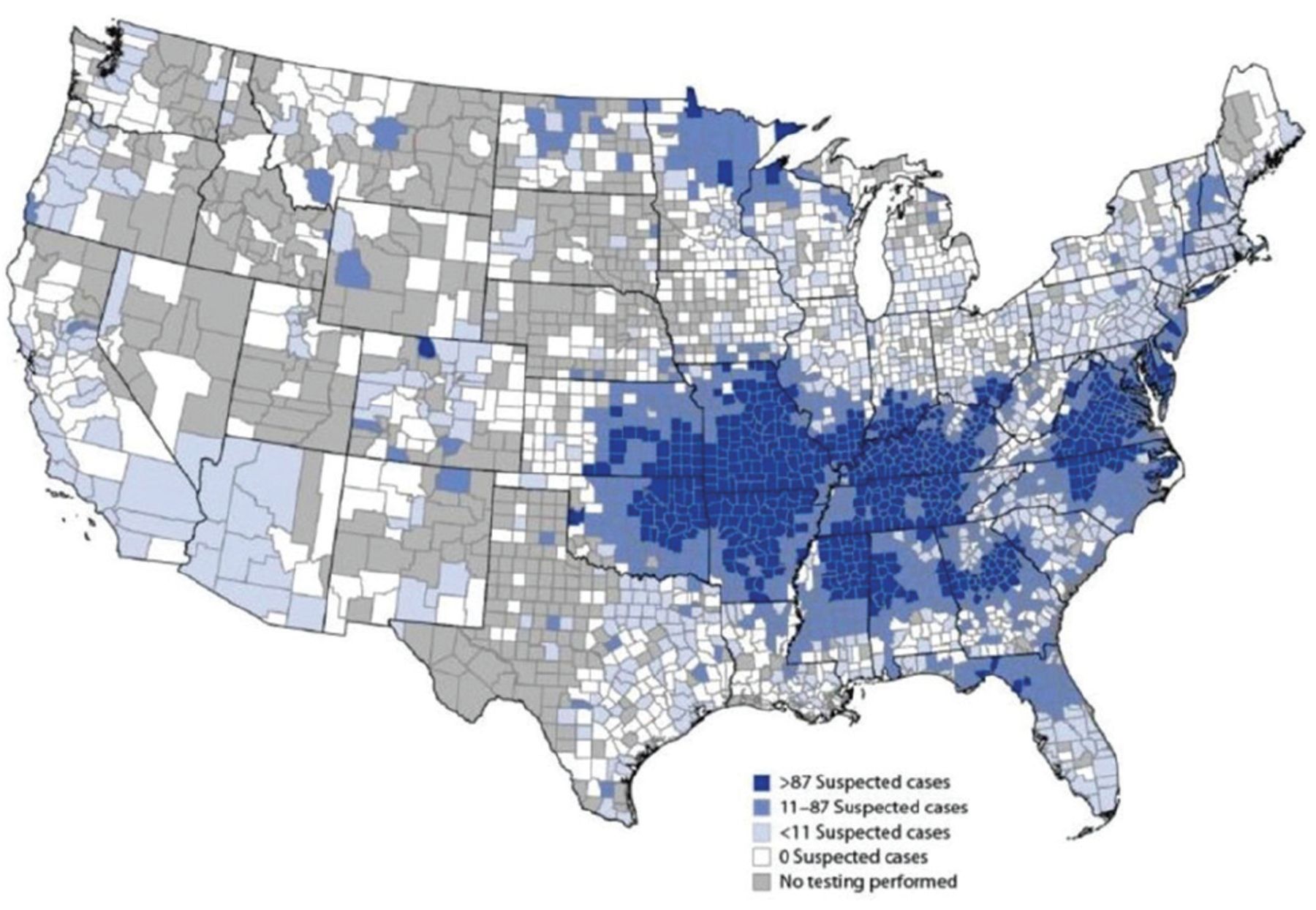
Clinicians should consider alpha-gal syndrome as a potential diagnosis if patients with unexplained gastrointestinal symptoms live or have lived in regions where alpha-gal syndrome is common (Figure 2).4 These regions are also where the lone star tick is found, and include the southern, midwestern, and mid-Atlantic United States—particularly parts of Oklahoma, Kansas, Arkansas, Missouri, Mississippi, Tennessee, Kentucky, Illinois, Indiana, North Carolina, Virginia, Maryland, and Delaware, and Suffolk County in New York (Figure 3).

US Centers for Disease Control and Prevention data on the geographic distribution of suspected cases of allergy to galactose-alpha-1,3-galac-tose (alpha-gal syndrome) per 1 million population per year in the United States (2017–2022).
Reprinted from reference 4.

Distribution map of the lone star tick (Amblyomma americanum) in the United States.
Reprinted from US Centers for Disease Control and Prevention. Lone Star Tick (Amblyomma americanum). stacks.cdc.gov/view/cdc/25414.
DIAGNOSIS IS A CHALLENGE
Alpha-gal syndrome is difficult to diagnose: the presenting symptoms can be vague, and reactions in sensitized individuals are delayed—typically happening late in the evening or in the middle of the night—or may not always occur, unlike other food allergies. Therefore, alpha-gal syndrome, especially gastrointestinal alpha-gal syndrome, may be underdiagnosed.
Alpha-gal syndrome is primarily identified through clinical evaluation and supported by laboratory testing. A history of tick bites, including larval tick bites (such as seed ticks) or “chigger” bites, and frequent engagement in outdoor activities can support a diagnosis of alpha-gal syndrome; however, tick bites are often painless, and around half of patients who develop a tick-borne illness don’t remember being bitten.15
Serum IgE testing
An alpha-gal IgE level of 0.1 kU/L or greater confirms the diagnosis of alpha-gal syndrome, as it has a reported specificity of 92.3% and a sensitivity of 100%.15 Laboratory testing for IgE antibodies against alpha-gal should be considered when clinical evaluation and patient history confirm 2 or more of the following:
Timing: nighttime symptoms, starting with itching
Ticks: history of tick bites, history of avid outdoor activities in tick-prevalent areas, prolonged irritation at the site of the tick bite
Diet: consumes mammalian meats and high-fat dairy.
Diagnosis can be particularly difficult in patients who have reactions to mammalian products but test negative for alpha-gal IgE, which occurs in approximately 2% of patients referred for evaluation of alpha-gal syndrome.15 Because patients with alpha-gal syndrome are also found to have elevated IgE antibodies against beef, pork, and lamb, serum IgE testing for these alternative markers can help establish the diagnosis.8
Skin testing
Skin prick tests with mammalian meat extracts are unreliable because of false negatives and should not be used to establish an alpha-gal syndrome diagnosis.15 The presence of IgE antibodies to beef can indicate a primary beef allergy, and IgE antibodies to pork (porcine and cat albumin) may signify pork-cat syndrome. Occasionally, skin testing for reaction to alpha-gal–containing drugs like cetuximab and basophil activation testing can be performed in those who test negative for alpha-gal IgE antibodies.
Oral food challenge
Although food allergies are generally diagnosed through food challenges, the delayed reaction characteristic of alpha-gal syndrome renders such challenges cumbersome and infeasible for routine clinical practice. However, if the initial serologic testing does not lead to a clear diagnosis, an oral food challenge may help.15
Given the unpredictable nature of alpha-gal food challenges, discussing the risks and benefits with patients is essential. According to Commins,15 15% to 20% of patients with alpha-gal syndrome undergoing food challenges required epinephrine, emergency medical transport, or both. As a result, alpha-gal food challenges should only be conducted by clinicians skilled in identifying and managing anaphylaxis, and should always be done in a controlled clinical environment where lifesaving treatments, such as epinephrine, are readily available.
These challenges should be performed when clinically appropriate in certain specific cases15:
Unclear cause of an allergic episode and patient tests positive for alpha-gal IgE (≥ 0.1 kU/L) but continues to consume mammalian meat without any symptoms
History of tick bites or significant exposure and patient tests positive for alpha-gal IgE and has been advised to avoid mammalian meat based solely on test results, despite not having symptoms
Alpha-gal IgE level less than 2.0 kU/L in a patient who can tolerate high-fat ice cream made from cow’s milk and a small amount of pepperoni (about 12 g) without any reactions and has no history of tick bites for 1 year
History of alpha-gal syndrome in patient who tests negative for alpha-gal IgE (< 0.1 kU/L) and has been followed over time
Symptoms suggest alpha-gal syndrome but patient tests negative for alpha-gal IgE and additional diagnostic tests have been inconclusive.
An oral mammalian meat challenge may be performed with 2 pork sausage patties (70 g) or 3 patties in patients weighing greater than 70 kg.15 Pork is used for oral challenges due to its fatty composition, which increases the likelihood of allergic reactions.19 After an oral challenge, these patients must be monitored for up to 6 hours due to the risk of delayed reactions.
MANAGEMENT OF ALPHA-GAL SYNDROME
Currently, there is no cure for alpha-gal syndrome. The primary management strategy is eliminating foods and products that contain alpha-gal for a minimum of 30 days.3 Promising data show that extended avoidance of alpha-gal can lead to symptom resolution in many patients. According to a 2021 study of 16 patients with alpha-gal IgE antibodies, three-quarters reported significant improvement or resolution of symptoms after following a strict alpha-gal–free diet over a median follow-up of 13 months.30
Avoiding dairy products is not part of our standard recommendation because 80% to 90% of patients with alpha-gal syndrome do not have reactions to cow’s milk or cheese.15 That said, published research and expert advice suggest that patients still symptomatic despite avoiding mammalian meat might benefit from eliminating dairy.24 Poultry, fish, and seafood, however, are safe for consumption because they do not contain alpha-gal.
Foods and products to avoid
Mammalian-derived products should be avoided. Gelatin, which is made from collagen in pig or cow bones, is present in foods such as marshmallows, gummy bears, and gelatin-based desserts, which should be avoided if previous allergic reaction episodes have occurred after exposure. Similarly, lanolin, collagen, and glycerin in personal care products are derived from mammals and should be avoided in instances of previous reactions. Because reactions have been reported with exposure to the monoclonal antibody cetuximab, it is reasonable to avoid it or to consult an allergist before starting this medication. Carrageenan, an additive made from seaweed and used to thicken and stabilize yogurt, nut milks, and processed meat products, also contains alpha-gal and may provoke an allergic reation.15
A summary of foods and products that do and do not contain alpha-gal is provided in Table 1.15,24
Food and product safety for patients with alpha-gal syndrome
Medical therapies
Medical therapy can be considered for patients with continued symptoms or with a high exposure risk (Table 2).3,15,31–33 Options include using long-lasting oral antihistamines such as fexofenadine or levocetirizine, which are effective for 22 to 28 hours after intake.32 An oral cromolyn solution may also be prescribed to stabilize mast cells, particularly to address gastrointestinal symptoms.13 Moreover, for refractory cases, the anti-IgE monoclonal antibody omalizumab may be helpful.34 In cases of severe allergic symptoms and anaphylaxis, patients must have access to self-injectable epinephrine for emergencies.
Recommended medications
Alternative therapies to treat alpha-gal syndrome, such as acupuncture, currently have no scientific evidence to support their use.
Referral to an allergist
Managing alpha-gal syndrome extends beyond simple dietary restrictions and involves a multidisciplinary approach with gastroenterologists, dietitians, and allergists to ensure comprehensive patient care. An allergist referral should be placed when patients have symptoms such as facial or throat swelling, voice changes, breathing difficulties, hives, or fainting after eating. These symptoms suggest a high risk of anaphylaxis and the need for epinephrine autoinjectors. Allergists can also assist with oral food challenges, especially when there is a potential risk of anaphylaxis.
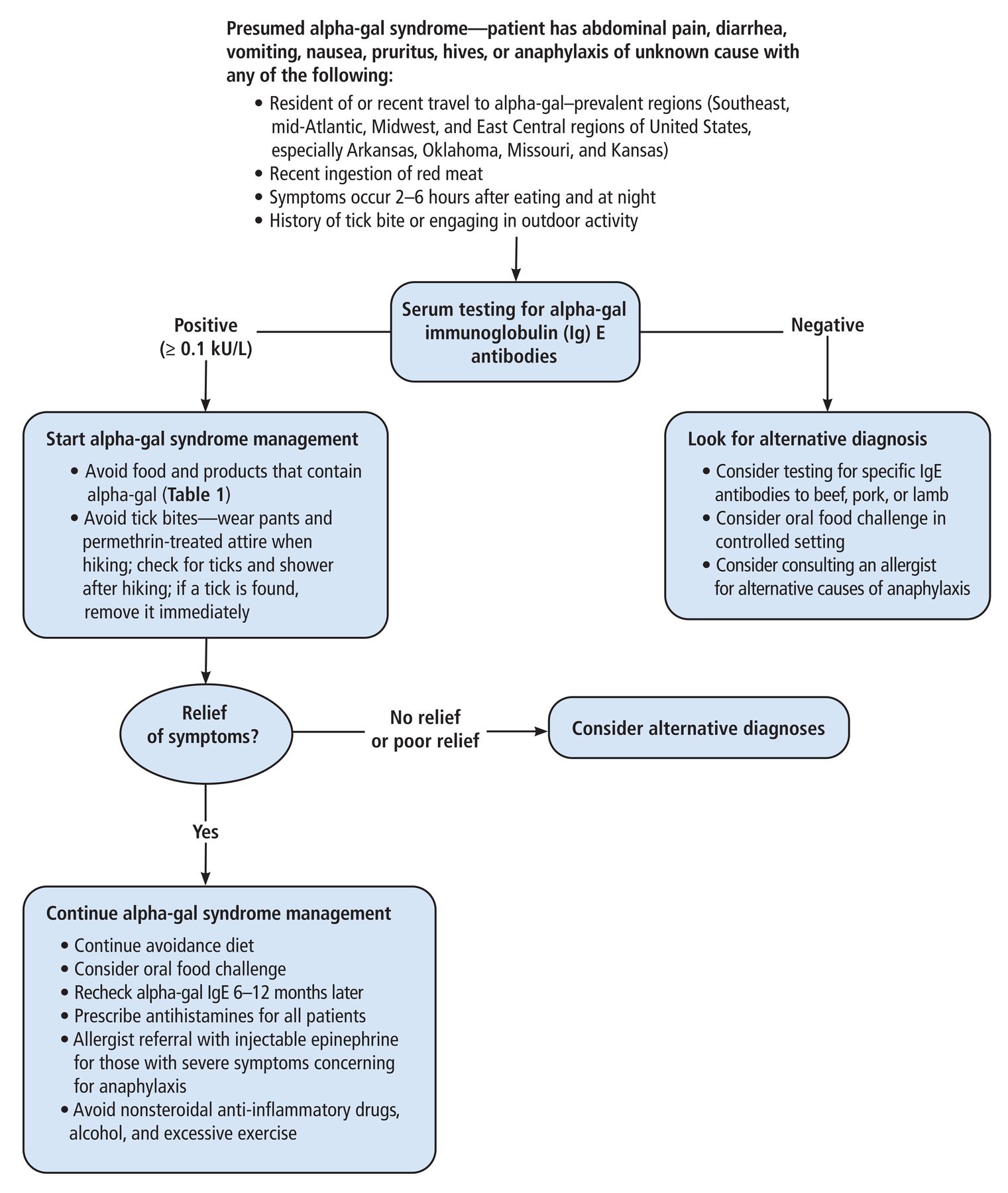
Figure 4 is our algorithmic approach to the diagnosis and management of presumed alpha-gal syndrome.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Algorithm for the diagnosis and management of presumed allergy to galactose-alpha-1,3-galactose (alpha-gal syndrome).
PREVENTING TICK BITES
Primary prevention for alpha-gal syndrome involves avoiding tick bites and taking appropriate action if a tick is detected. Areas where ticks are common, such as tall grass, bushes, shrubs, and leaf litter, should be avoided. Moreover, ankles and legs should be covered while hiking, ideally with clothes and boots treated with permethrin to deter ticks, and N,N-diethyl-meta-toluamide should be applied to the skin.3,35
Tick checks should be conducted after outdoor activities in wooded areas. The lone star tick is considerably larger than the blacklegged tick, which is the vector for Lyme disease, making it much more visible. If a tick is found, it should be removed immediately with the help of tweezers, grasping the tick near its head or mouth to ensure complete removal without crushing. An antiseptic can then be applied to the area.
ADVICE FOR PATIENTS WITH ALPHA-GAL SYNDROME
Patients with alpha-gal syndrome should be cautioned to prevent future tick bites, as repeated bites can sustain or increase alpha-gal IgE levels, which could exacerbate their allergy and symptoms.6,11 Most patients (89%) who avoid tick bites tend to see a decline in their alpha-gal IgE levels.36 While the rate of decrease varies, and it is uncertain what level of reduction is necessary to restore tolerance, Commins15 found that nearly 12% of patients tracked for more than 5 years had negative alpha-gal IgE titers (< 0.1 kU/L) and were able to reintroduce mammalian meat into their diets.
In addition, if patients with alpha-gal syndrome are still consuming red meat, they should be advised to use alcohol and nonsteroidal anti-inflammatory drugs with caution and to limit their consumption of fatty meats. It is also crucial to educate these patients about the potential risk of accidental exposure to alpha-gal through processed foods, restaurant meals, and inhalation of aerosolized alpha-gal from cooking bacon or beef products.
RESEARCH GAPS AND FUTURE IMPLICATIONS
There is a lack of research on alpha-gal syndrome, and comprehensive studies are needed. Research should focus on evaluating the symptoms and immune responses in patients sensitized to alpha-gal through blinded food challenges with both alpha-gal–free and conventional mammalian meat, which would deepen our understanding of the clinical spectrum of gastrointestinal alpha-gal syndrome. Additionally, exploring the timeline to symptom resolution while following an alpha-gal–free diet and identifying factors that might further improve symptoms would be valuable. Investigating sensitized individuals who do not have symptoms, the mechanisms responsible for the spectrum of symptoms among patients with alpha-gal syndrome, and whether alpha-gal syndrome can cause chronic systemic inflammation and contribute to coronary artery disease could provide valuable insights into potential health consequences.
Moreover, further geographic studies on the regions where alpha-gal syndrome is prevalent should be conducted to identify individuals at a higher risk who might benefit from stricter preventive measures. Clear guidelines for risk stratification and desensitization protocols in patients with alpha-gal syndrome are also needed.
TAKE-HOME POINTS
Alpha-gal syndrome has emerged as a significant and increasing contributor to anaphylaxis and severe allergic responses to mammalian meat.1
Gastroenterologists need to be aware of alpha-gal syndrome, particularly because some patients exhibit gastrointestinal symptoms without skin or anaphylactic reactions.3
An alpha-gal syndrome diagnosis is presumed when a symptomatic patient is from a region where lone star ticks are prevalent and has a history of a recent tick bite and mammalian meat consumption.15
Definitive diagnosis requires laboratory testing that reveals increased serum alpha-gal IgE antibodies in patients with gastrointestinal distress who then show improvement on a diet that avoids alpha-gal.15
The primary management strategy is eliminating alpha-gal exposure and preventing future tick bites to mitigate the risk of escalating IgE titers and worsening allergy symptoms.3,6
Referral to an allergist is recommended for patients experiencing severe reactions.
DISCLOSURES
The authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
- Copyright © 2025 The Cleveland Clinic Foundation. All Rights Reserved.