


ABSTRACT
Bronchoscopy is an aerosol-generating procedure that creates unique challenges for healthcare providers to reduce the potential spread of the COVID-19 respiratory pathogen. As part of the initial response, Cleveland Clinic postponed elective surgeries including bronchoscopy. We established a 5-tier system for prioritizing the urgency of bronchoscopy procedures. When elective bronchoscopies were resumed, we established protocols to reduce aerosolization and potential virus transmission risks such as using an airborne infection-isolation room and changing to total intravenous anesthesia. Also, we established guidelines for periprocedural care and use of personal protective equipment including requirements for wearing N95 masks for all bronchoscopy procedures.
INTRODUCTION
Bronchoscopy is a challenging medical procedure in the context of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) because it is an aerosol-generating procedure.1,2 Infection control is intrinsic to the daily practice of bronchoscopy teams as they routinely manage respiratory pathogens including those requiring standard or contact precautions typical in hospital patients. For example, droplet isolation is commonly used during seasonal viral infections, and respiratory isolation is needed for pathogens such as tuberculosis. Existing guidelines about personal protective equipment (PPE), room and space considerations, and various levels of isolation are core competencies. Bronchoscopy is used to diagnose and treat many thoracic diseases including emergent procedures, so it is important to have procedures in place to manage patients with or suspicious for COVID-19, as well as those without COVID-19.
Since the COVID-19 pandemic has emerged, many published guidelines specific to bronchoscopy have been published.3⇓-5 While there are similarities and differences in each, the core principles are all based on relatively limited knowledge of COVID-19, requiring authors to use data from historical insights with other infections and extrapolate them into known constructs. As with any guidelines, they represent the best intentions and summaries of the collective knowledge of the expert authors and the various methodologies they used.
The most notable major change was for the use, reuse, and conservation of PPE. Before wide-spread shortages occurred related to COVID-19, most PPEs were used once, and accreditation and infection control policies were strict on this measure. Also, the processes of donning and doffing PPE amidst increased protective measures have changed accordingly.
PRIORITIZING BRONCHOSCOPY PROCEDURES
Early on in the COVID-19 pandemic, following guidance from the Ohio Department of Health,6 the Cleveland Clinic postponed elective (or nonessential) surgeries. Exceptions existed for surgeries that were life-saving, prevented permanent dysfunction, decreased the risk of metastasis, or decreased severe symptoms.
As bronchoscopy has a wide range of indications, we created a tier system that prioritizes the importance of bronchoscopy and related pleural procedures (Table 1), based on exceptions outlined by state health officials. Each procedure is evaluated to determine its priority tier. If it meets the criteria to be performed, we only proceed with all safety measures in place to protect patients and healthcare providers. A similar tier system was published by the Society of Advanced Bronchoscopy that stratified patients based on urgency.5
Cleveland Clinic recommended priority tiers for bronchoscopy and pleural procedures
The American Association of Bronchology and Interventional Pulmonology (AABIP) declared that bronchoscopy is “contraindicated” as a first-line diagnostic procedure for patients with potential COVID-19.7 Instead, they recommend obtaining samples from the upper airway via swab techniques for the diagnosis of COVID-19. However, bronchoscopy may still have a limited role in confirming the diagnosis of COVID-19 if the first-line testing is inconclusive and to rule out other pathologies. These considerations are relative to the prevalence of disease and available hospital resources.
At the time of this writing, local and state authorities have authorized the resumption of elective procedures, under the assurance that hospital capacity is available to accommodate patients if a surge is observed and that there are enough PPEs available. This is an evolving local assessment and is not uniform across the United States. Thus, many of the procedures that were postponed are now being performed.
PREPROCEDURE TESTING
Increased procedure availability is partly based on the ability to perform preprocedure COVID-19 testing as recommended by the American College of Chest Physicians guidelines.3 (A review of testing platforms is beyond the scope of this paper.) These guidelines have been changing. In addition, the Centers for Disease Control (CDC) has published caveats regarding the false-negative rates of tests and the possibility of conversion during the incubation period.8
Preprocedural COVID-19 testing helps inform perioperative care. If COVID-19 is diagnosed, we may postpone the procedure. Testing is also important for postoperative care planning, home care, and contact tracing. A few asymptomatic patients with positive tests had their procedures postponed. Others with negative tests but with high clinical suspicion of COVID-19 or other possible respiratory pathogens were placed into preprocedure quarantine pending bronchoscopy results.
BRONCHOSCOPY ENVIRONMENT OF CARE
Patients with known, suspected, or unknown COVID-19 status are managed as if they are positive. This follows well-established protocols used for typical respiratory pathogens. We made these changes because the level of community spread and individual risk is unknown and the accuracy of testing is not sufficient to ignore the high-risk nature of bronchoscopy. Bronchoscopy typically is performed in an airborne infection-isolation room, formerly referred to as a negative-pressure room, based on accreditation standards.
Anesthesia considerations
Bronchoscopy is performed with sedation (by the pulmonologist performing the bronchoscopy) or anesthesia (by an anesthesiologist) depending on the complexity of the procedure. Most of our procedural sedation bronchoscopies were for routine surveillance in lung transplant patients, and these were mostly elective and initially postponed. To reduce the risks of virus aerosolization, procedural sedation for bronchoscopy is now performed under general anesthesia administered intravenously. In addition, we stopped using nebulized or atomized lidocaine; aggressively manage cough throughout the procedure; perform bronchoscopy through an established airway, either a supraglottic airway or an endotracheal tube; and avoid the use of high-flow oxygen supplementation, all to minimize aerosols. Table 2 compares the virus aerosolization risks between procedural sedation and general anesthesia for bronchoscopy.
Comparison of virus aerosolization risks between procedural sedation and general anesthesia for bronchoscopy
Anesthesiologists also have made changes to minimize aerosolization. They replaced standard induction of anesthesia with rapid-sequence induction and prefer an endotracheal tube over a supraglottic airway. Higher consideration is given for the use of intraoperative muscle relaxants to avoid coughing, use of fentanyl as an antitussive, and management of postoperative nausea and vomiting to avoid retching and its potential for aerosolization. They avoid jet ventilation, and high-flow nasal cannula oxygenation and ventilation, the so-called THRIVE technique (transnasal humidified rapid insufflation of oxygen and ventilatory exchange). For more details, see Procedural sedation in the COVID-19 era.
After the procedure, the environment is cleaned and sanitized with an EPA-registered cleaner effective against most pathogens, including SARS-CoV-2.9 The CDC refers to a terminal clean, yet there is no clear understanding of the time required for SARS-COV-2 to be cleared. Typically, the time needed to “clear the air” after each case is based on the air handling system and how many air exchanges per hour occur. A typical airborne infection isolation room has 12 air exchanges per hour and, thus, would require 35 minutes to have 99.9% removal efficiency.10
Personal protective equipment
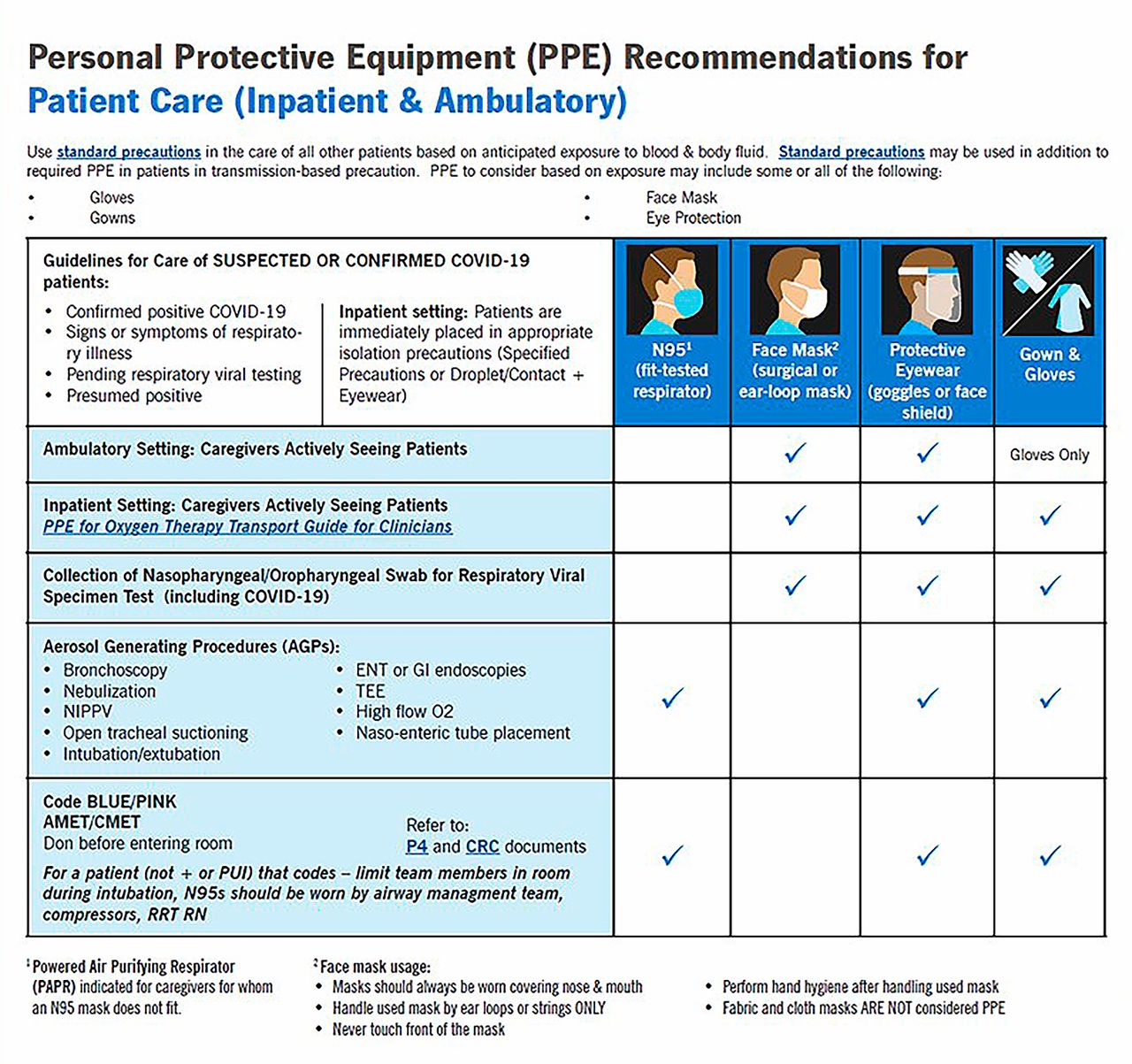
Cleveland Clinic has issued PPE recommendations for inpatient and ambulatory care of patients with suspected or confirmed COVID-19 (Figure 1). Standard precautions for all healthcare workers in the bronchoscopy room are to wear gowns, gloves, and eye protection along with a fitted National Institute for Occupational Safety and Health (NIOSH)-certified N95 mask or powered air-purifying respirator (PAPR). Previously, only a surgical mask was required for most bronchoscopy procedures. It was common to use N95 masks or PAPRs to care for patients with respiratory pathogens. Now, it is recommended to wear an N95 mask during all bronchoscopy procedures regardless of the patient’s SARS-CoV-2 test result. The AABIP guidelines note that N95 is at least similar to PAPR, based on expert consensus.3

Cleveland Clinic personal protective equipment recommendations for COVID-19.
We instituted PPE preservation in several ways. First, we reduced the total number or people in the procedure room. To achieve this, we eliminated nearly all observers and industry representatives. We also limited the number of trainees who can participate in the procedure, then we limited the number of personnel changes during the procedures. Furthermore, we implemented the extended use and reuse of PPE as recommended by CDC under crisis management plans.11 On this regard, we have 2 work flows. In cases of known or suspected COVID-19, PPEs are discarded after each use. In all others, the N95 masks and face shields (after being wiped) are reused during subsequent procedures until the end of the day. Lastly, we collect used N95 masks and face shields at the end of day and send them for decontamination reprocessing.
POSTBRONCHOSCOPY AND RECOVERY
Postprocedure droplet generating coughing is universal. After the procedure, if tolerated, patients wear a surgical mask as source control and during transfer to the recovery area. The patient is placed in a bed with at least 6 feet of space from other patients with curtains drawn and droplet precautions instituted (Table 3). Healthcare providers wear surgical masks, face shields, and standard PPE (gloves and, gowns) when in close contact with recovering patients. In patients with suspected or proven COVID-19, we fully recover them in the airborne infection isolation environment of the procedure rooms. This was applied as an extra cautionary measure until the patient is ready to go home or is moved to a COVID-19 unit to limit the area that needs to be sanitized, to reduce the number of caregivers directly in contact with the patient, and to conserve PPE.
COVID-19 infection control guidance for health-care professionals from the CDC8
Footnotes
The statements and opinions expressed in COVID-19 Curbside Consults are based on experience and the available literature as of the date posted. While we try to regularly update this content, any offered recommendations cannot be substituted for the clinical judgment of clinicians caring for individual patients.
- Copyright © 2020 The Cleveland Clinic Foundation. All Rights Reserved.
In this issue







{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.