


ABSTRACT
Resuming procedural sedation services for elective procedures during the COVID-19 pandemic requires unique considerations to ensure safety for patients and providers. Guidelines for resuming these procedures, including timing, screening and testing, use of personal protective equipment, and case planning are discussed. Approaches to procedural sedation can be modified to reduce the risk of droplet or aerosol transmission by decreasing nasal cannula oxygen supplementation flows. Decreasing the need for oxygen supplement can be accomplished by opioid and sedative sparing strategies, including the use of multimodal analgesia and non-pharmacologic analgesic and anxiolytic interventions. Recommendations are made for patients who are COVID-19 positive and require procedural sedation.
INTRODUCTION
The US Government publication “Guidelines for Opening Up America Again” proposes a phased reopening approach based on downward trends of COVID-19 (caused by the novel severe acute respiratory syndrome corona virus 2 [SARS-CoV-2]) cases in the community.1 With the expansion of testing capability, personal protective equipment (PPE) inventory, and healthcare system capacity, facilities are resuming elective procedures, with adherence to Centers for Medicare and Medicaid Services (CMS) guidelines.2 Typically, these elective procedures, which include diagnostic, therapeutic, and minimally invasive procedures, are performed under moderate (conscious) sedation by non-anesthesiologist proceduralists, also referred to as procedural sedation. These procedures may require unique considerations and preparations to be safely and effectively performed.
The Society for Ambulatory Anesthesia (SAMBA) recently published two statements providing guidance on preoperative COVID-19 testing and resuming ambulatory care in outpatient facilities, ambulatory surgery centers, hospitals, and office-based practices.3,4 These statements are congruent with CMS recommendations and include details regarding when to restart elective surgeries, COVID-19 screening and testing, standards for PPE use, as well as case prioritization and scheduling. These principles are applicable to both ambulatory surgery and moderate sedation procedures.
WHEN TO RESUME ELECTIVE PROCEDURAL SEDATION
According to government and healthcare officials’ recommendations, before a facility resumes elective procedures, the community should have either a low incidence of COVID-19 cases or a sustained downward trajectory of COVID-19-like illnesses or positive tests within a 14-day period. Hospitals should have the capacity to treat all patients without crisis care protocols and have a robust testing program in place. Healthcare facilities should have sufficient resources including PPE, medications, supplies, surgical and anesthetic equipment, and workforce availability to provide care of non-COVID-19 patients without jeopardizing surge capacity (Table 1).2
Baseline criteria for restarting elective procedures
PRE-PROCEDURAL COVID-19 SCREENING AND TESTING
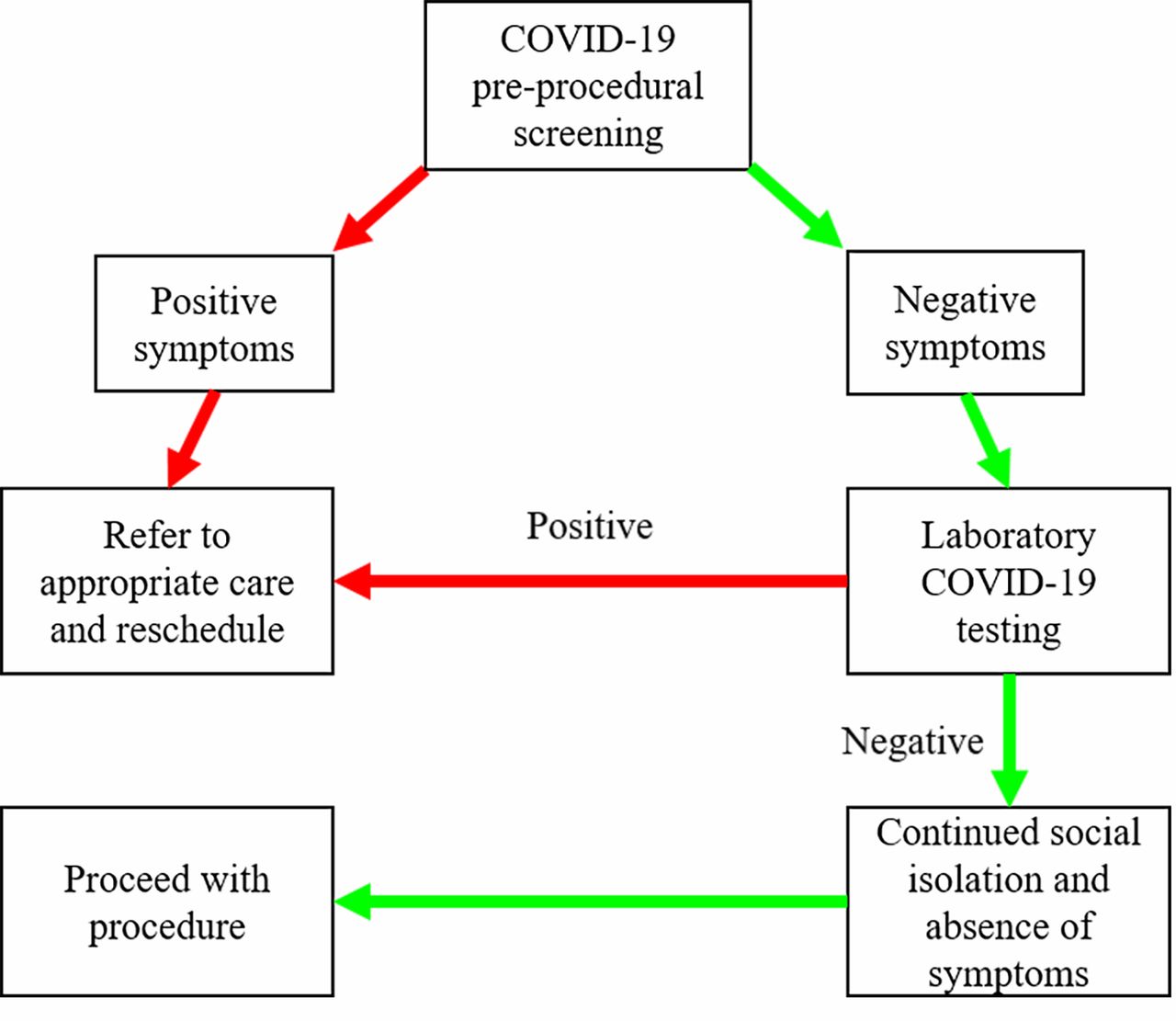
Pre-procedural screening and testing for COVID-19 are necessary before all non-emergency procedures to ensure the safety of patients and healthcare providers. Patients with COVID-19 symptoms (Table 2) should be referred for appropriate care and have their procedure rescheduled. Patients without symptoms should have a laboratory COVID-19 test 24 to 72 hours before their scheduled procedure. Once tested, patients should be encouraged to self-isolate until the procedure and report any change in symptoms. Figure 1 shows an algorithm for screening and testing patients.
CDC: Symptoms of COVID-195

Pre-procedural flowchart for pre-procedural screening and testing patients for COVID-19.
Pre-procedural COVID-19 testing is necessary as patients may become infected and have viral transmission up to 3 days before becoming symptomatic.6 Infected patients undergoing surgery who were asymptomatic have been found to have more significant disease progression, a higher incidence of ICU admission, and higher mortality.7
PERSONAL PROTECTIVE EQUIPMENT
Although COVID-19 testing will help identify patients who are infected, the reported sensitivity varies in different anatomical sites (eg, bronchoalveolar, nasopharyngeal, and sputum), leaving significant possibility for false-negative results.8 Additionally, patients may become infected between the test and the procedure. Due to these possibilities, even for COVID-19 negative patients, droplet precautions (eye protection, surgical mask, and gloves) should be used for non-aerosolizing procedures and airborne precautions (eye protection, N95 mask, gown, and gloves) should be used for aerosol-generating procedures (AGPs).2,3 These procedures involve mucous membranes such as those in the respiratory, naso-oropharyngeal, and gastrointestinal tracts. AGPs include intubation, extubation, bronchoscopy, upper and lower endoscopy, airway surgeries, and interventions such as using high-flow nasal cannula oxygen, positive-pressure mask ventilation, or continuous positive airway pressure (CPAP) ventilation.4,9–11
SCHEDULING A NON-EMERGENCY PROCEDURE FOR A PREVIOUSLY COVID-19 POSITIVE PATIENT
The decision to schedule a non-emergency procedure for a patient with previously confirmed COVID-19 should be based on whether they are asymptomatic or symptomatic. If symptomatic, then the severity of symptoms and the need for hospitalization and intensive care treatments should be evaluated. Based on the clinical course, state of recovery, and rehabilitation, the patient should undergo pre-procedural evaluation to determine their fitness for the procedural sedation. Once the decision is made to undergo the procedure, viral shedding should be considered, which is highest at symptom onset and can occur for up to 21 days.6 Due to the potential for prolonged viral shedding, the CDC guidelines for discontinuation of transmission-based precautions for previously COVID-19 positive patients can also be utilized for scheduling cases.
For symptomatic patients with COVID-19, they should not be scheduled until cleared by either a symptom-based or test-based strategy, as follows:
Symptom-based strategy requires at least 3 days since recovery (resolution of fever without antipyretics and improvement in respiratory symptoms) and at least 10 days since symptom onset.
Test-based strategy requires resolution of fever without antipyretics, improvement in respiratory symptoms, and 2 consecutive negative COVID-19 tests more than 24 hours apart.
For asymptomatic patients with COVID-19 positive test, a time-based or test-based strategy should be used:
Time-based strategy requires 10 days to pass since the positive COVID-19 test without subsequent symptoms, although viral shedding could last longer.
Test-based strategy requires 2 consecutive negative tests at least 24 hours apart.
CDC: Discontinuation of transmission-based precautions for patients previously positive for COVID-1912
STEP-WISE APPROACH TO RESUMING TIME-SENSITIVE AND ELECTIVE PROCEDURES
During the initial phase of resuming elective procedures, it is important to prioritize those that are urgent and time-sensitive. In some areas, it may be ideal to begin with low to moderately complex procedures to reduce the number of patients requiring postoperative in-patient care.
REDUCING SARS-COV-2 TRANSMISSION
Appropriate sanitation protocols should be in place for common areas and procedural suites to reduce the risk of virus transmission. In addition to standard cleaning between cases, extra environmental cleaning (waiting areas, door handles, common surfaces, and elevator surfaces) should be implemented.2,3 For aerosol-generating procedures, allow adequate time between cases for appropriate room air exchange to reduce the risk of transmission from residual aerosolized particles.3 This time frame should be based on the time required for air exchange in individual procedural suites.
Social distancing should continue to be observed among patients and visitors in waiting areas and both pre- and post-procedure areas. This may require lower patient volumes. Visitors should only be allowed if their presence is necessary for patient care, and they should be screened for symptoms or COVID-19 exposure. Visitors accompanying patients may benefit from the option to leave and be contacted by phone to return to pick up the patient. Patients and visitors should wear cloth or surgical masks at all times unless not feasible during the procedure.2,3
For staff, establish distancing between workstations and limit interactions. Dividing the staff into dedicated teams per area may be helpful. Non-COVID-care zones can be established, if feasible, to further reduce the risk of transmission. Staff in this zone should not cross over into COVID-19 areas. All staff members should be routinely screened for COVID-19 symptoms and, if positive, appropriately quarantined and tested. Additionally, staff should wear surgical face masks at all times and consistently practice proper hand hygiene.
COVID-19-RELATED CONSIDERATIONS IN PROCEDURAL SEDATION
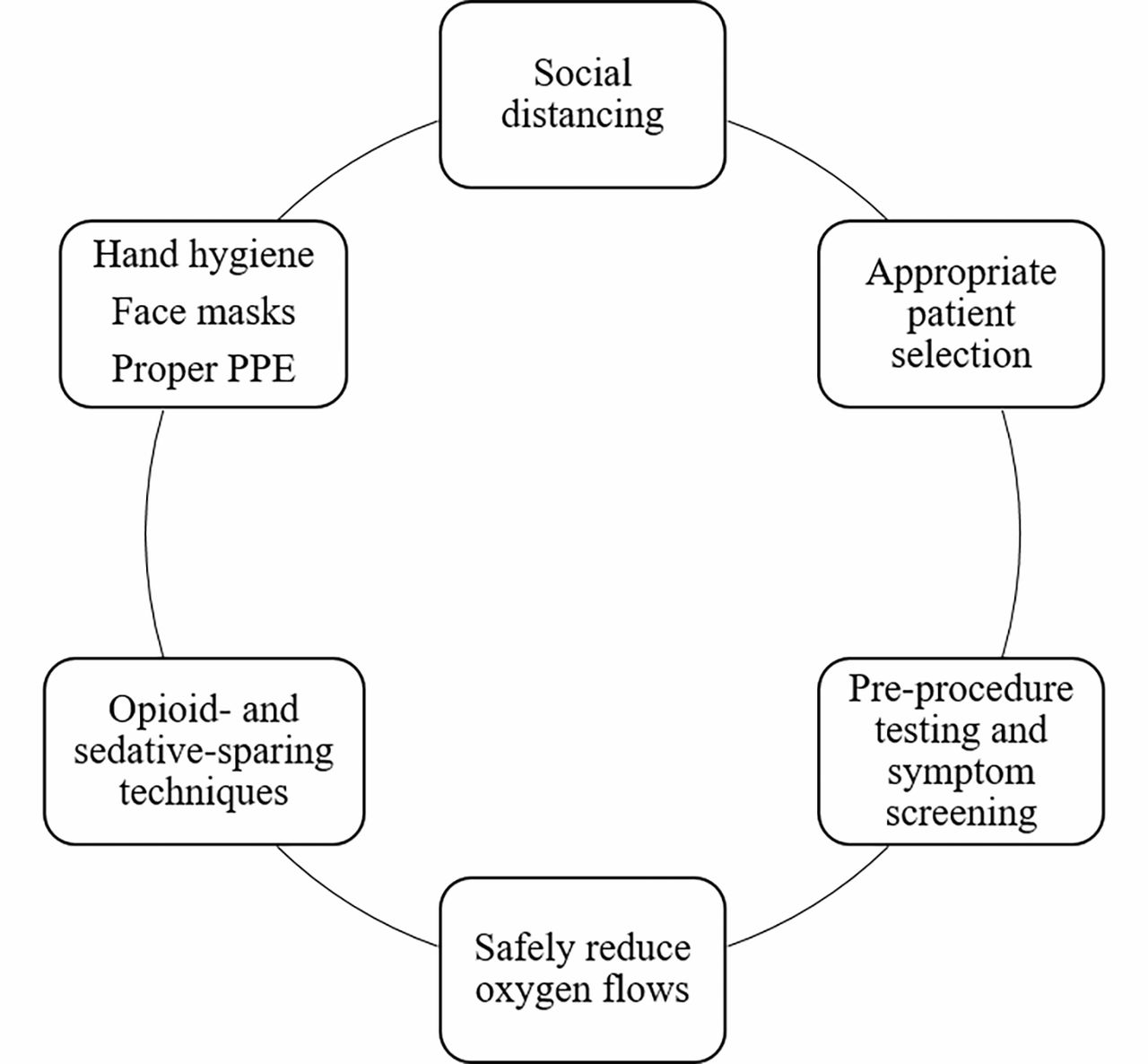
The risk of viral transmission during procedures can be significantly reduced with planning and implementing recommended interventions (Figure 2).3,4 However, procedural sedation may present unique challenges to risk reduction, such as the need to provide high-flow oxygen supplementation via nasal cannula or face mask, repetitive coughing, patient disinhibition, or unforeseen complications. The dis persion distance of exhaled air is a function of the oxygen flow rate through the nasal cannula and can reach up to 1 meter at flow rates of 5 L/min. Dispersion distance from a leaky noninvasive ventilation full face mask can be even further and is a function of the amount of positive pressure used to achieve adequate ventilation.13
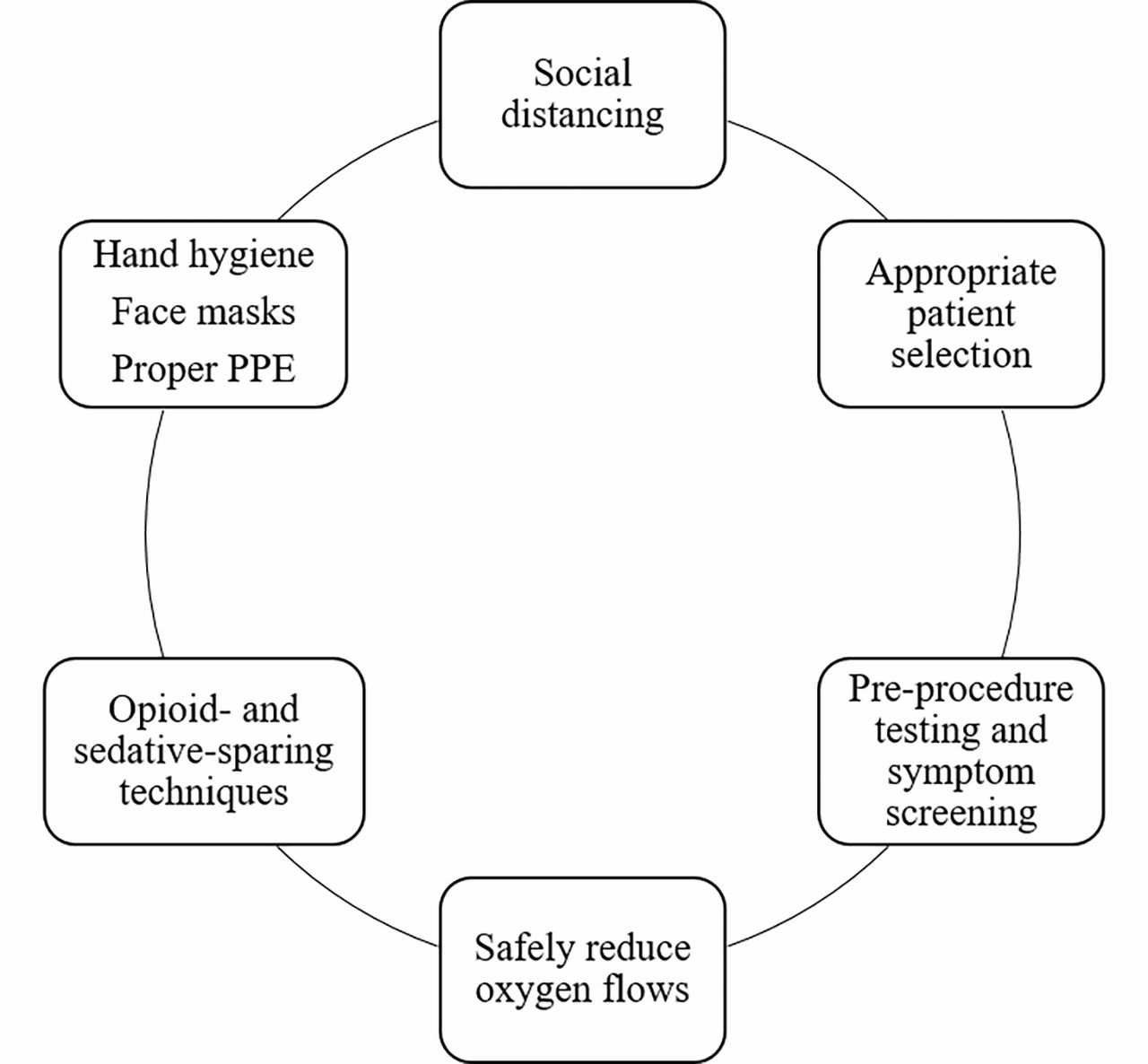
Intervention for safe procedural sedation during COVID-19 pandemic.
To minimize the need for supplemental oxygen and the risk of aerosolization, practitioners should evaluate patients for the opportunity to reduce the dose requirement of systemic sedatives (benzodiazepines) and opioid analgesics. This may be achieved with multimodal analgesia and opioid-sparing strategies, which have been used successfully in the perioperative setting.14
When clinically appropriate, patients should be given nonopioid analgesia pre- and post-procedure, including acetaminophen and nonsteroidal anti-inflammatory medications. Nonopioid analgesics have been shown to reduce postoperative opioid requirements in opioid-naive patients while providing acceptable pain control and high patient satisfaction.13 Local anesthetics such as lidocaine can be subcutaneously administered or applied topically to mucous membranes to provide analgesia to decrease the need for systemic opioid.
Efforts should be made to alleviate fears and anxiety during the preoperative visit, through discussion and reassurance. Other non-pharmacologic sedative-sparing interventions prior to procedures could be beneficial for anxiety relief, including music therapy, aromatherapy, massage, or other relaxation techniques.15,16
ALTERNATIVE APPROACHES TO PROCEDURAL SEDATION
Certain circumstances may warrant careful consideration of whether procedural sedation is the best approach due to risk of droplet or aerosol contamination. Patients who are already on home oxygen therapy or those who require preoperative oxygen may require above average oxygen flows via nasal cannula or face mask during their procedural sedation. Some procedures (eg, repetitive, painful, or complex) may require sedation levels that will necessitate above-minimal supplemental oxygen (2-3 L/min). Certain patient factors may require increased oxygen flow or airway manipulation, such as significant comorbidities, a physical exam that suggests a difficult airway, or a history of high-sedation requirements or failed sedation procedures. In such cases, consultation with an anesthesiologist and scheduling the procedure under general anesthesia could be a reasonable alternative.
PROCEDURAL SEDATION FOR COVID-19 POSITIVE PATIENTS
For time-sensitive or urgent procedures in patients who are COVID-19 positive or for patients who do not meet CDC criteria for discontinuation of transmission-based precautions, their procedures should be performed without delay. There are recommendations for reducing the transmission risk.2–4 Patients with COVID-19 should wear a mask at all times and be isolated from other patients, visitors, and non-COVID care zones. To reduce the risk of cross-contamination, have designated COVID-only care areas and healthcare teams, if feasible.2 Personal protective equipment, including gowns, eye protection, and fitted N95 masks or powered air-purifier respirator, should be used by all team members.
The procedure area should be prepared in advance by limiting exposure of supplies and equipment. This can be achieved by placing only the necessary supplies, equipment, and medications in the room and by keeping all storage cabinets and doors closed during the procedure. Use plastic sheets to cover items that cannot be stored away and dispose them after the case. After the procedure, the room should be thoroughly (ie, terminally) cleaned and equipment disinfected. Allow adequate time between cases for droplets and aerosols to settle or be eliminated by air turnover.
Considerations should be given to the most appropriate healthcare setting for performing procedures in COVID-19 positive patients. Specifically, for patients at risk of sudden clinical deterioration requiring escalation of care or emergency intervention, including intubation and mechanical ventilation, appropriate support and inpatient resources should be immediately available.
CONCLUSION
As the United States progresses through the reopening phases, guidelines and statements provide essential navigation for healthcare systems. For moderate sedation procedures, recommendations from medical societies provide further support for the safety of patients, healthcare providers, and the community from the risks of COVID-19.
Footnotes
The statements and opinions expressed in COVID-19 Curbside Consults are based on experience and the available literature as of the date posted. While we try to regularly update this content, any offered recommendations cannot be substituted for the clinical judgment of clinicians caring for individual patients.
- Copyright © 2020 The Cleveland Clinic Foundation. All Rights Reserved.
In this issue




{kind=link}
{kind=link}
Jump to section
- Article
- ABSTRACT
- INTRODUCTION
- WHEN TO RESUME ELECTIVE PROCEDURAL SEDATION
- PRE-PROCEDURAL COVID-19 SCREENING AND TESTING
- PERSONAL PROTECTIVE EQUIPMENT
- SCHEDULING A NON-EMERGENCY PROCEDURE FOR A PREVIOUSLY COVID-19 POSITIVE PATIENT
- STEP-WISE APPROACH TO RESUMING TIME-SENSITIVE AND ELECTIVE PROCEDURES
- REDUCING SARS-COV-2 TRANSMISSION
- COVID-19-RELATED CONSIDERATIONS IN PROCEDURAL SEDATION
- ALTERNATIVE APPROACHES TO PROCEDURAL SEDATION
- PROCEDURAL SEDATION FOR COVID-19 POSITIVE PATIENTS
- CONCLUSION
- Footnotes
- REFERENCES
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- No citing articles found.