

A 44-year-old woman presented to the primary care clinic with diplopia and swelling of the right eyelid that had increased over the past 2 weeks. She denied fevers, chills, headache, cough, shortness of breath, or rashes.
Physical examination confirmed right eyelid edema, with unilateral ptosis and proptosis (Figure 1). There was no pain with eye movements. She was prescribed doxycycline for suspected preseptal (periorbital) cellulitis. However, the eyelid swelling increased, and she was referred to an ophthalmologist for examination and imaging of the orbits.

(A) A cellphone photo taken by the patient shows right eyelid swelling approximately 1 week after symptom onset. (B) Eyelid swelling increased, with associated ptosis and proptosis, approximately 2 weeks after symptom onset. (C) Exposure of the lacrimal gland mass during orbitotomy.
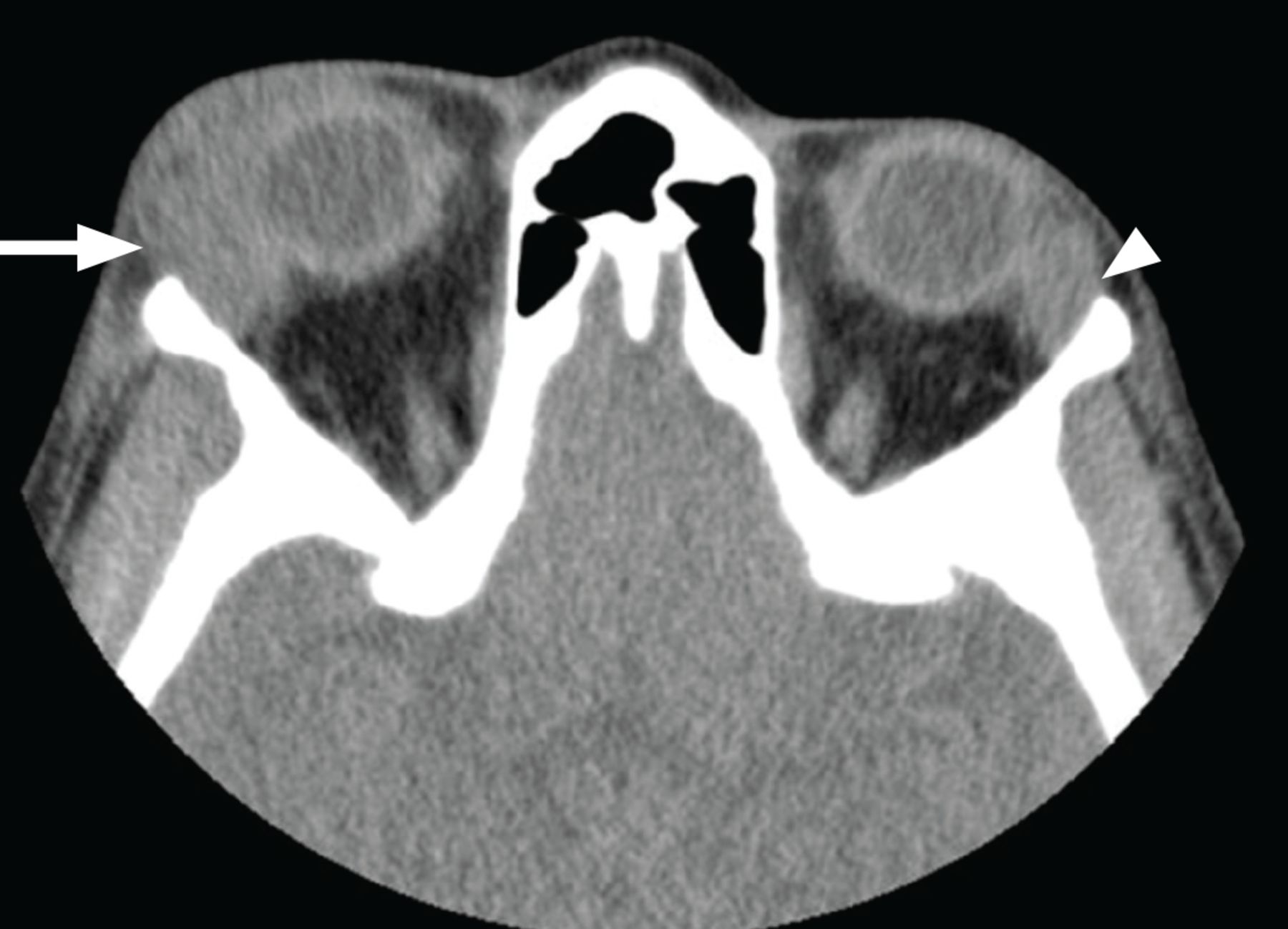
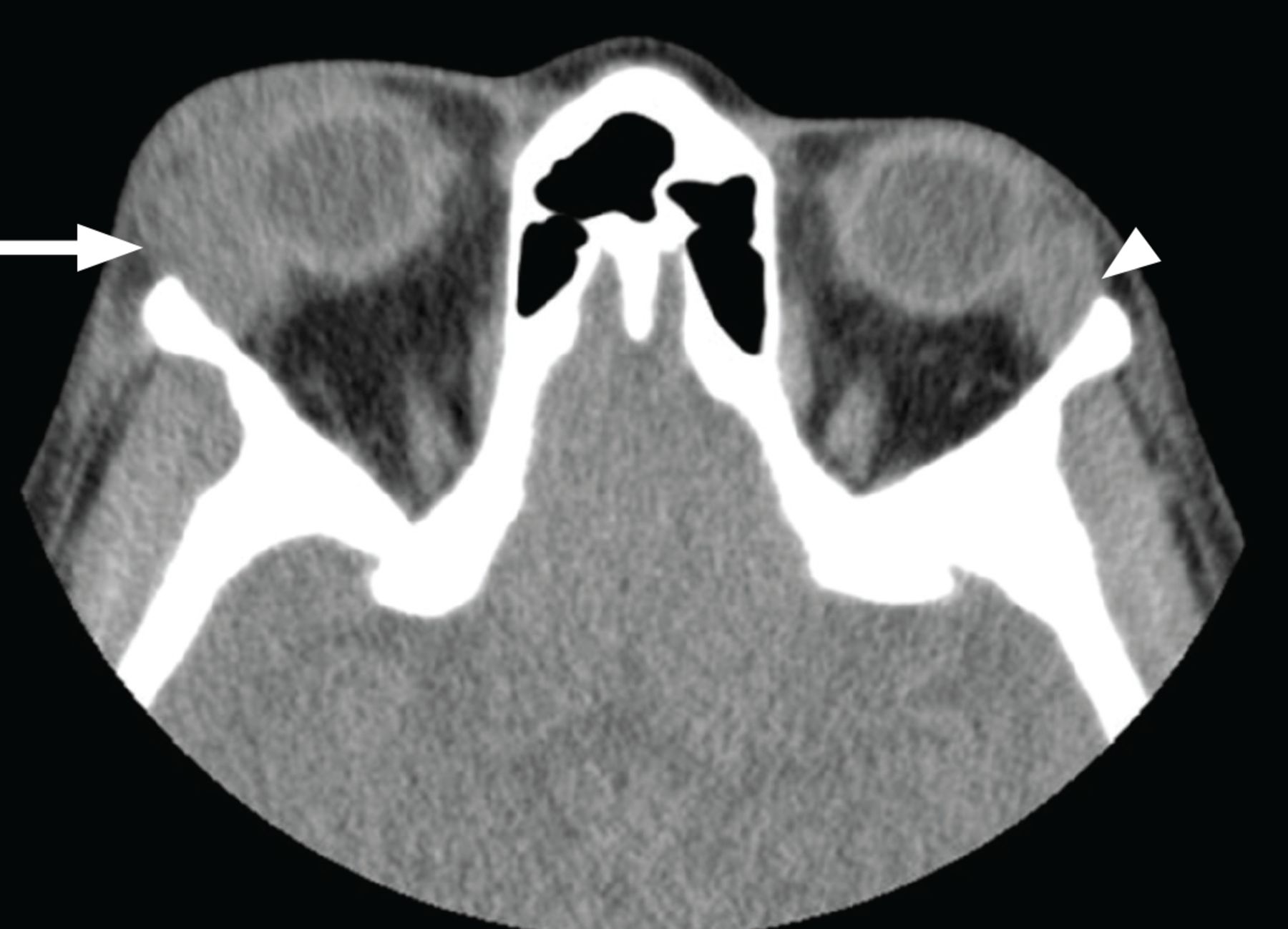
Computed tomography (Figure 2) revealed abnormal soft tissue masses in the lacrimal glands of both eyes, with a larger mass in the lacrimal gland of the right eye, causing ptosis and downward displacement of the right globe. The patient underwent right anterior orbitotomy with biopsy of the right lacrimal gland. Vision and physical appearance of the left eye were not significantly affected.
{kind=link}
{kind=link}
Axial computed tomography of the orbits showed homogeneously confluent, enlarged lacrimal glands, right (arrow) greater than left (arrowhead).
FURTHER EVALUATION PROVIDES DIAGNOSTIC CLUES
The differential diagnosis for the patient’s symptoms and presentation included infection, malignancy, and inflammatory disorders such as immunoglobulin G4-related disease and sarcoidosis. Biopsy of the right lacrimal gland demonstrated nonnecrotizing granulomatous inflammation, with well-formed granulomas. Histochemical staining for acid-fast bacilli and fungi was negative. There were no features concerning for malignancy. Testing for systemic inflammatory disease—computed tomography of the chest, C-reactive protein, and sedimentation rate—was nondiagnostic.
The diagnosis of sarcoidosis is based on 3 major criteria designated by the American Thoracic Society: a clinical presentation compatible with sarcoidosis (eg, lacrimal gland swelling, as in this patient), nonnecrotizing granulomatous inflammation in a tissue sample, and exclusion of other etiologies of granulomatous disease.1 As other causes of granulomatous inflammation were felt to be less likely, sarcoidosis was favored as the cause of the patient’s lacrimal enlargement. Given the absence of systemic symptoms and normal results on chest computed tomography, disease involvement was initially considered to be isolated to extra ocular tissue, and the patient was diagnosed with extraocular sarcoidosis using International Workshop on Ocular Sarcoidosis criteria.2
ISOLATED LACRIMAL GLAND INVOLVEMENT IN SARCOIDOSIS
Sarcoidosis may affect any organ, but the lungs are usually involved. Patients frequently present with ocular involvement, which is more common in female and African American patients.3,4
The American Thoracic Society recommends a baseline eye examination for all patients diagnosed with systemic sarcoidosis.1 Sarcoidosis may affect any part of the eye and its adnexa, presenting most commonly with uveitis, dry eyes, and conjunctival nodules.3 The lacrimal gland is also often affected.5 Significant enlargement of the lacrimal gland leads to the effects observed in our patient, ie, eyelid swelling, ptosis, and globe displacement.
Isolated lacrimal involvement is unusual. Collison et al,6 in a small case series, concluded that although most patients with extraocular orbital sarcoidosis eventually develop systemic sarcoidosis, there are rare cases in which there is no evidence of systemic disease at the time of biopsy.6
Our patient eventually developed systemic sarcoidosis with biopsy-proven cutaneous lesions 10 months after the onset of extraocular symptoms.
MANAGEMENT OF OCULAR SARCOIDOSIS
Management of ocular sarcoidosis centers on initial systemic corticosteroid and immunosuppressive therapy, with or without excision.2 Our patient’s symptoms progressed on prednisone at a high dose of 80 mg and hydroxychloroquine. She has been maintained on oral methotrexate monotherapy at a weekly dose of 10 mg with folic acid supplementation.
DISCLOSURES
The authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
- Copyright © 2022 The Cleveland Clinic Foundation. All Rights Reserved.