


ABSTRACT
A growing number of international postmortem studies identify acute and organizing diffuse alveolar damage (DAD) as the main pathologic feature of lung injury in patients with COVID-19. Other forms of acute lung injury, including organizing pneumonia, and acute fibrinous and organizing pneumonia are seen. Acute neutrophilic infiltrates have been observed, most frequently as the manifestation of a superimposed bacterial pneumonia. SARS-CoV-2 has been detected in type I and type II pneumocytes and bronchial epithelial cells using electron microscopy, immunohistochemistry, and in situ hybridization, and likewise, viral transcripts were localized with RNA probes in pneumocytes. However, the presence of true viral cytopathic effect seen with light microscopy remains to be defined. Interestingly, vascular changes are frequently observed in association with DAD, which include severe endothelial injury/endothelialitis, hemorrhage, and thrombotic and microangiopathic vasculopathy. Since similar vascular changes also occur in cases of DAD independent of the etiology, whether the vascular pathology in COVID lungs has unique features and represents a separate pathologic process is under investigation.
INTRODUCTION
Corona virus disease (COVID-19), caused by the novel coronavirus SARS-CoV-2, has spread globally since the initial outbreak in China in late 2019. On March 11, 2020, the infection was declared a pandemic by the World Health Organization. Patients infected with the virus may be asymptomatic or have symptoms with varying degrees of severity involving predominantly the respiratory tract. About 20% of patients develop severe disease and the mortality rate of patients with COVID-19 is .5% to 2%. Research on all aspects of the disease has been fast moving as understanding the epidemiology, pathogenesis, clinical, and pathologic characteristics of SARS-CoV-2 infection are crucial for the development of immunization and treatment strategies.
Studies of the histopathologic changes of COVID-19 are predominately conducted postmortem after clinically severe forms of the disease. The novelty and high infectivity of COVID-19 requires extra biosafety measures, including appropriate personal and environmental protective equipment. Because of this, many pathology laboratories have limited autopsies in these patients. Nonetheless, numerous published studies of the histopathology of COVID-19 have emerged and increased recently, resulting in a growing consensus about the main features of the pulmonary pathology of COVID-19.
HISTOPATHOLOGY
The predominant pathology in the lungs of deceased patients with COVID-19 is diffuse alveolar damage (DAD).1–14 This pattern of acute lung injury is the histologic finding observed in patients with acute respiratory distress syndrome regardless of the etiology. It results from epithelial and endothelial injury after an initial insult that leads to increased permeability of the alveolar-capillary barrier with consequent edema, release of proinflammatory and repair chemical mediators, impairment of the metabolism of surfactant, and abnormalities in the coagulation pathways. The interplay of these mechanisms varies depending on the causative agent, but the ultimate morphology of DAD has similar features. DAD is divided into 2 main phases, the acute phase and the organizing phase.15 Microscopically, the acute phase consists of vascular congestion with alveolar septal edema, fibrinoid exudates within the alveolar spaces and hyaline membranes. In the organizing phase of DAD, the alveolar interstitium is replaced by fibroblastic tissue, which can be prominent, and the alveolar septae are lined by reactive/reparative type II pneumocyte hyperplasia.
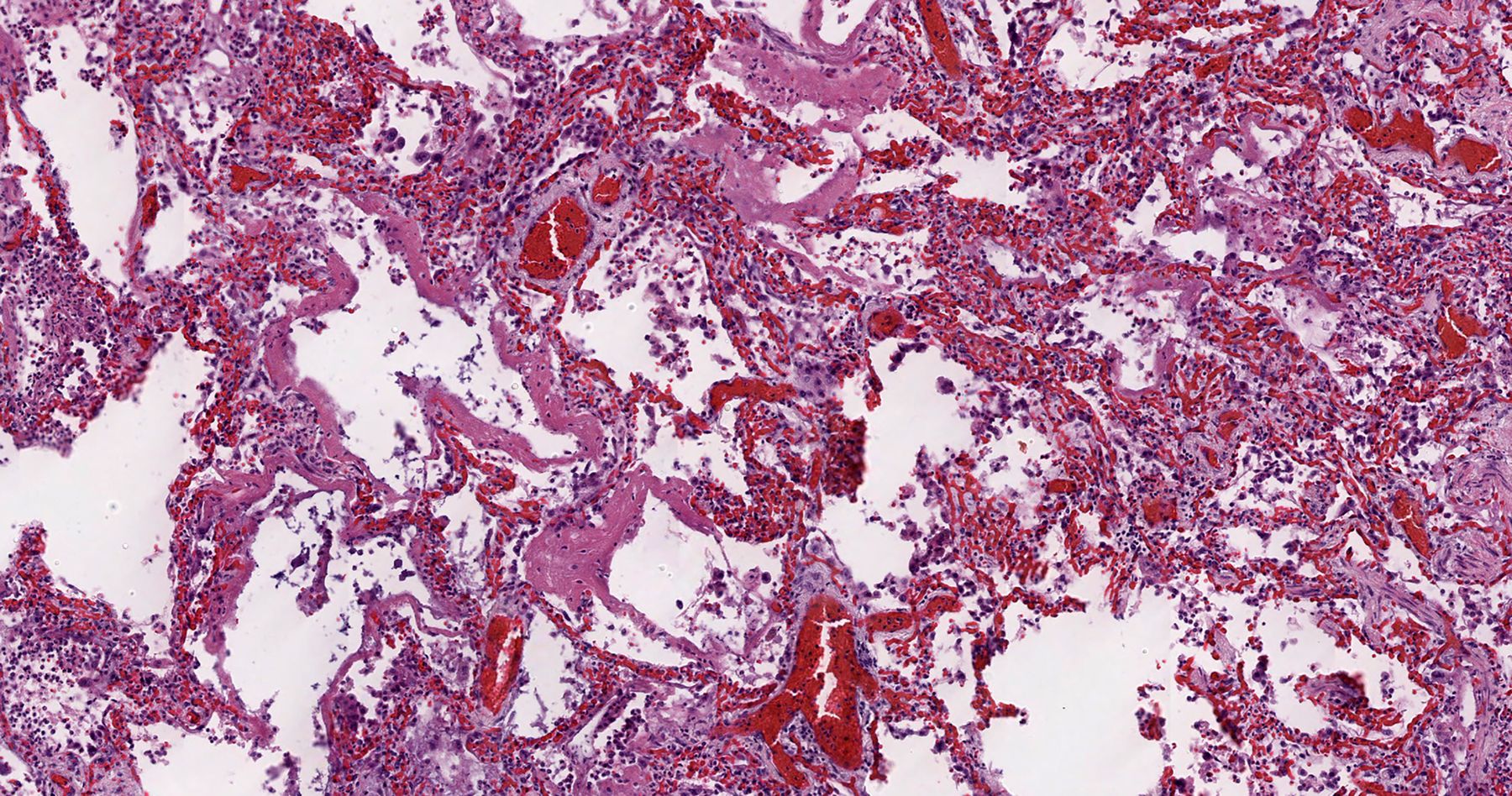
The pulmonary pathology findings of COVID-19 have been reported predominantly from autopsy cases of severely ill patients with acute respiratory distress syndrome, many of them with long hospital stays before expiration. Accordingly, DAD (Figure 1), in varying stages of evolution, is the predominant pathology pattern, though patterns of other forms of acute lung injury including acute fibrinous and organizing pneumonia,4,6,10 and organizing pneumonia2,6,9,13 may occur. Acute neutrophilic infiltrates have been observed in some cases, most frequently as the manifestation of a superimposed bacterial pneumonia. Large airway inflammatory changes include mucosal ulceration, acute and/or chronic inflammation. A recent study observed that 45% (17/38) of patients who were never intubated and 52% of patients with no associated bacterial or fungal pneumonia showed acute inflammation of the large airways. The authors did not find a significant relationship between overall large airway inflammation and intubation, or bacterial or fungal pneumonia.13
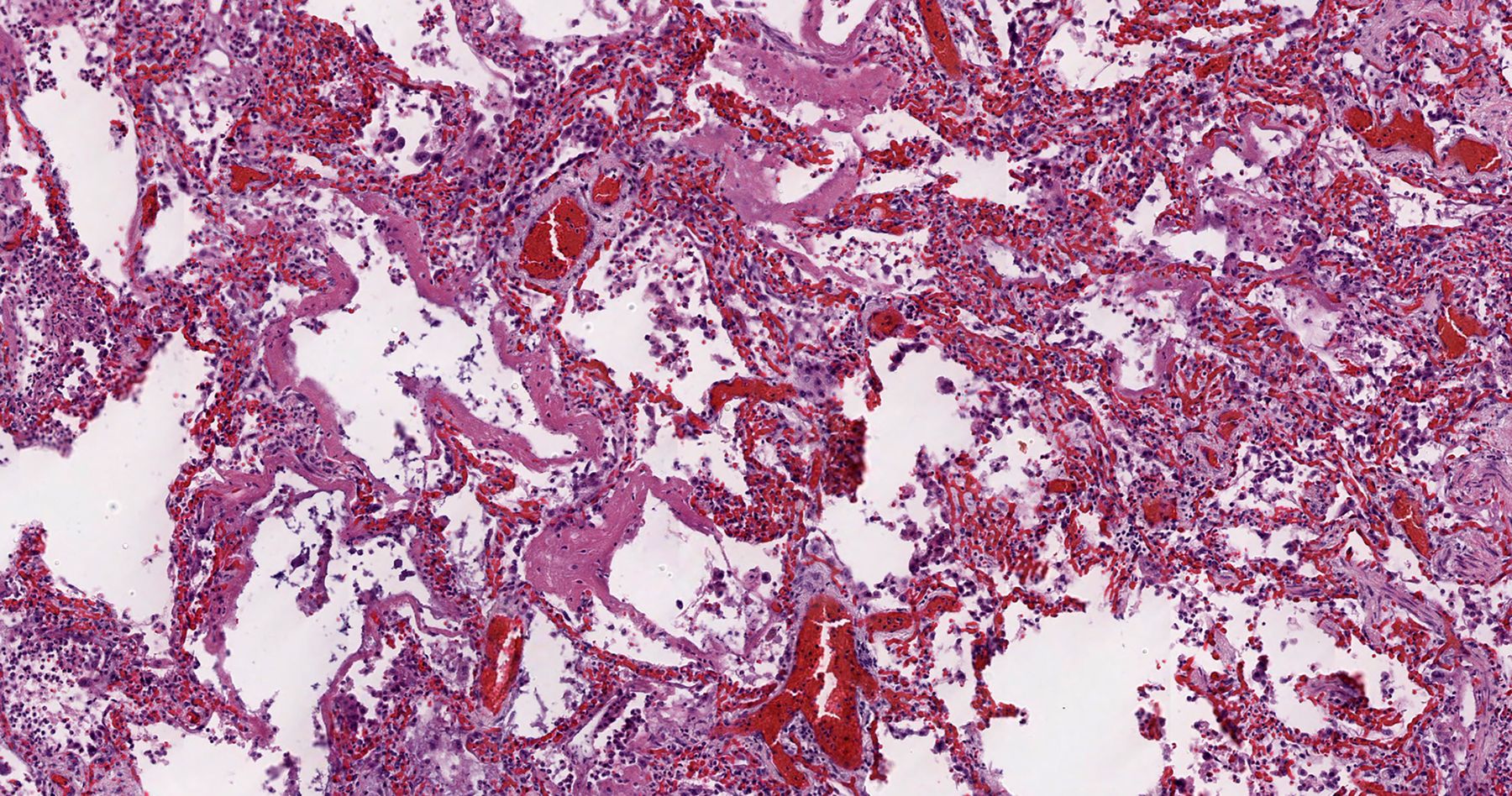
Acute diffuse alveolar damage: scattered hyaline membranes line the alveolar walls with vascular congestion and interstitial inflammation present within the interstitium (Hematoxylin and eosin; 200x).
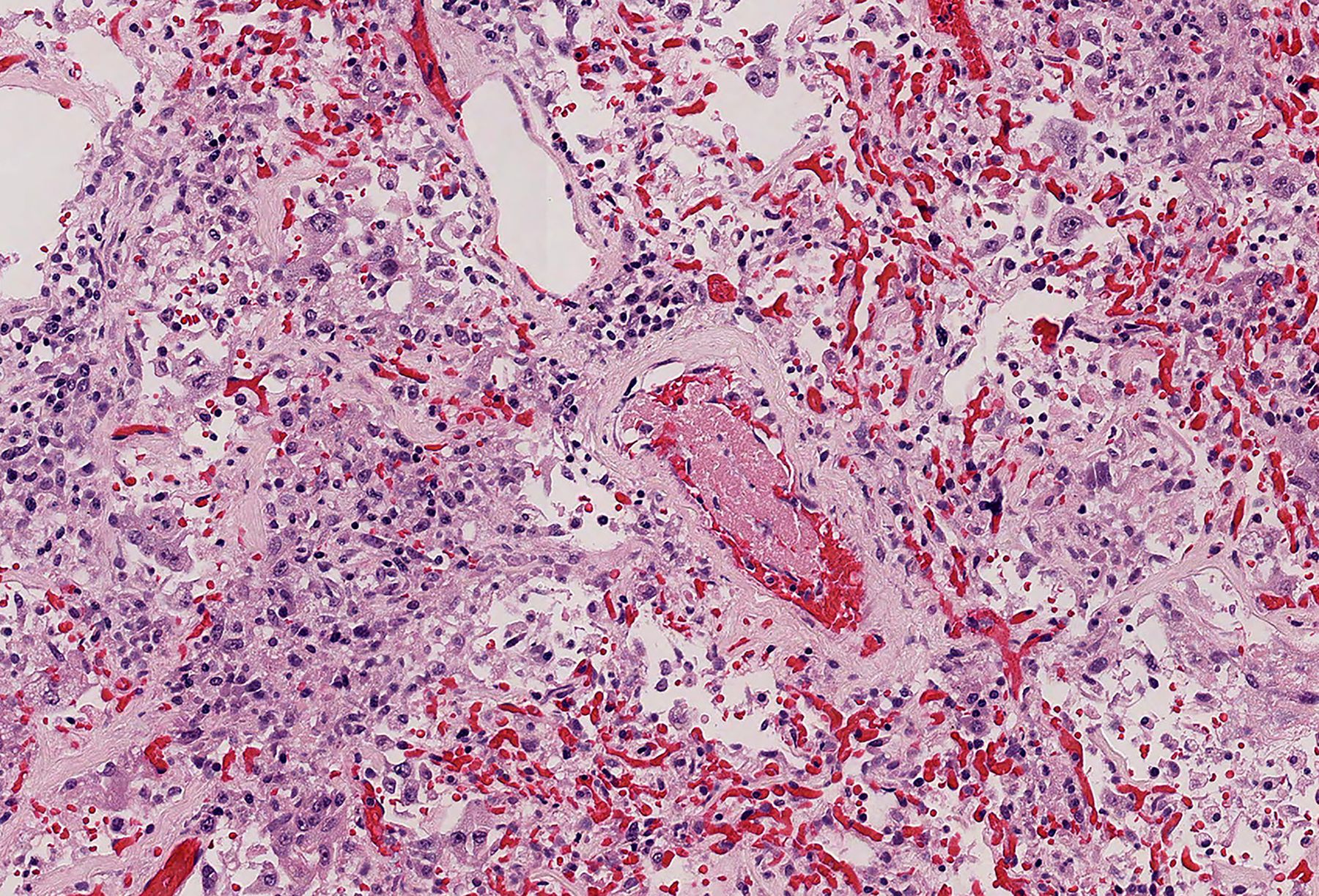
In addition to DAD, other findings described by pathologists include interstitial lymphocyte-predominant mononuclear cell infiltrates3,8,10,16,17 and vascular changes such as severe endothelial injury/endothelialitis,10,16,18,19 thrombotic and microangiopathic vasculopathy2,4–6,9,10,13,16,18–20 (Figure 2), and pulmonary hemorrhage.3–6,11 The microangiopathy and coagulopathy in patients with COVID-19 is thought to result from the endothelial cell activation and damage occurring secondary to the binding of the virus to the endothelial cells via angiotensin-converting enzyme 2 receptors, as well as activation of the coagulation through several procoagulant pathways induced by a dysregulated immune response or cytokine storm that occur in severe forms of the disease.18,21,22 However, these events can occur in DAD independent of the cause, thus the significance of their presence in COVID-19 lungs has yet to be elucidated. Furthermore, a recent postmortem histologic examination of DAD in the lungs of patients with COVID-19 compared with patients with DAD from other causes revealed that DAD is histologically indistinguishable in the 2 groups.4
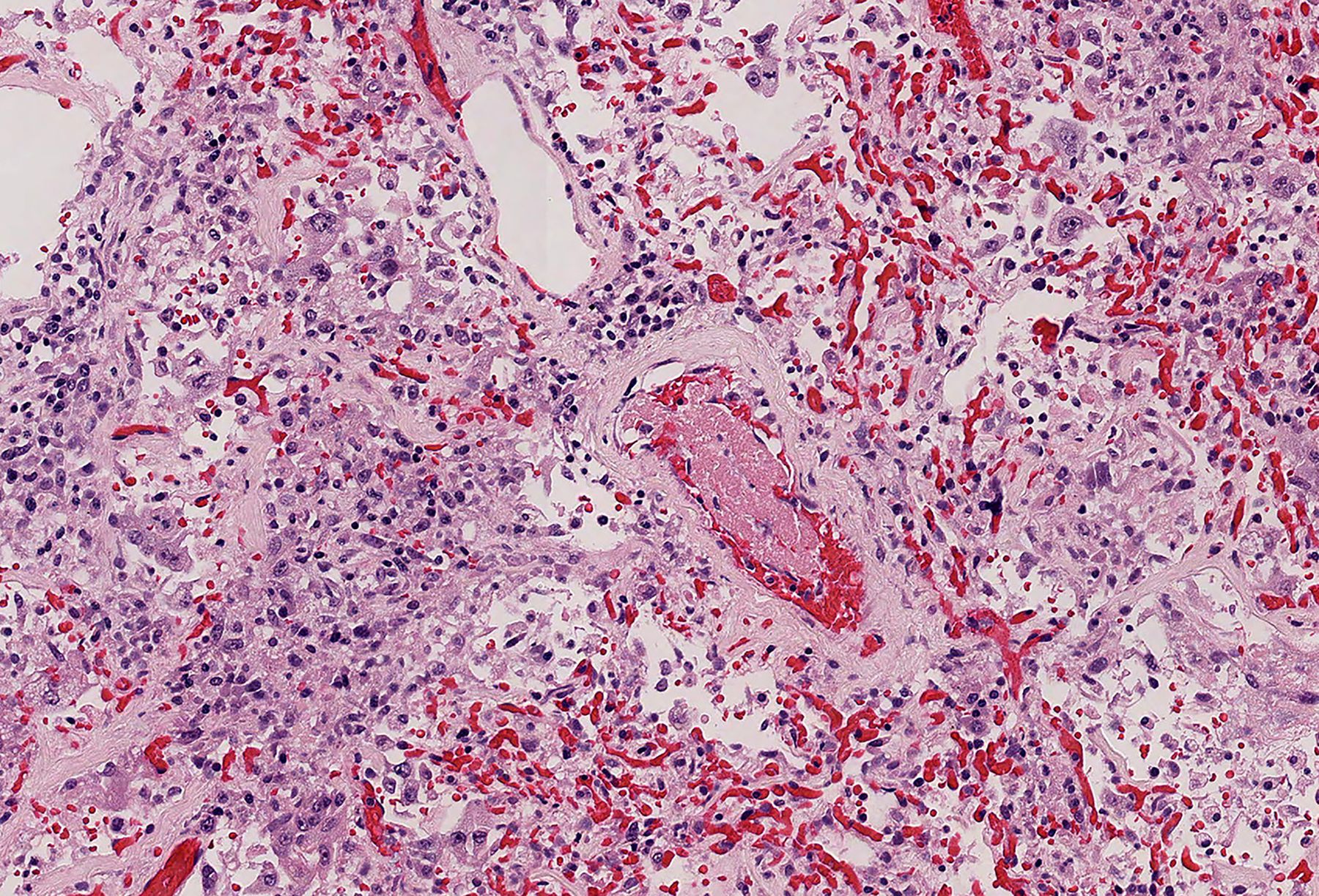
Organizing thrombus: an early organizing thrombus is present within a small artery. The surrounding lung reveals areas of vascular congestion (Hematoxylin and eosin; 200x)
Other histologic features reported in lungs infected with SARS-CoV-2 include intra-alveolar hemorrhage with both hemosiderin and intra-alveolar fibrin present. The etiology of this hemorrhage is not clear, though microvascular fragility due to complement activation has been speculated. Also, many studies report the presence of atypical large pneumocytes or atypical multinucleated giant cells and have suggested that the changes are due to viral cytopathic effect. In this regard, the virus has been detected in type I and type II pneumocytes using electron microscopy, immunohistochemistry and in situ hybridization, and RNA probes have localized viral transcripts in pneumocytes.1,6,9,12–14,23–27 However, specific morphologic features of a viral cytopathic effect in the lungs of patients with COVID-19 using light microscopy remain to be defined.
The discrepancies in the reported pulmonary pathology of COVID-19 are often based on the determination of DAD or other causes. The pathological definition of DAD can vary among authors. Since DAD can have lymphocytic infiltrates early in the disease with congested capillaries, especially when a virus is the etiology, the reports of a separate capillaritis-like pathology may arise from cases of a very early DAD where this pattern can be seen. Similarly, as stated, thrombosis that is seen throughout these lungs, is also a feature of DAD. However, the controversy arises from the extent of the thrombi seen in COVID-19, that is, the number of thrombi in COVID-19 lungs beyond what would manifest in DAD due to other causes. Most recently, studies that have quantitated the amount of thrombi present, suggest that the number present is beyond what would be seen in a non-COVID-19 DAD and most likely represent a thrombosis that is a separate pathologic process from DAD.14,16
FINAL COMMENTS
A growing number of international postmortem studies identify acute DAD as the main pathologic feature of lung injury in patients with COVID-19. Other forms of acute lung injury, including acute fibrinous and organizing pneumonia, and organizing DAD are seen, as are numerous thrombi and areas of pulmonary hemorrhage. Though multinucleated giant cells and enlarge pneumocytes with cleared chromatin are found, whether these represent true viral cytopathic effects remains to be defined.
Footnotes
The statements and opinions expressed in COVID-19 Curbside Consults are based on experience and the available literature as of the date posted. While we try to regularly update this content, any offered recommendations cannot be substituted for the clinical judgment of clinicians caring for individual patients.
- Copyright © 2020 The Cleveland Clinic Foundation. All Rights Reserved.




{kind=link}
{kind=link}