


ABSTRACT
Point-of-care ultrasound has an important role in the management of patients with COVID-19 infection. Because the utility of each application varies by setting, individual institutions should consider how they can best use ultrasound within their specific environments. In general, procedural guidance and focused echocardiography are high yield. Lung ultrasound has the potential to aid the diagnosis and management of patients with COVID-19 infection. Lower extremity point-of-care ultrasound for deep vein thrombosis may help guide decision making regarding anticoagulation or undifferentiated shock. It is of the utmost priority that ultrasound not spread infection, so point-of-care ultrasound must be used only when clinically indicated. Institutions should have protocols for machine disinfection.
BACKGROUND
The highly infectious nature of the SARS-CoV-2 virus via respiratory droplets can lead to contamination of medical and radiologic devices during use. The concern for nosocomial spread of the virus among healthcare workers and other hospitalized patients has led many societies and medical centers to recommend appropriately limiting exposure and imaging.1,2
Point-of-care ultrasound is increasingly being used to diagnose, monitor, and manage patients in emergency departments and in those admitted to inpatient services. In patients with COVID-19 infection it is an excellent tool for comprehensive examination given that ultrasound is already commonly used in patient care, handheld ultrasound devices are easy to clean, and the nature of the virus is critical and dynamic.
In this Curbside Consult, we present typical lung ultrasound findings in patients with COVID-19 infection and discuss other uses of point-of-care ultrasound in their care. We also highlight key points about the disinfection of ultrasound machines and introduce a protocol that minimizes the time needed to assess infected patients for deep vein thrombosis as well as lung and cardiac abnormalities.
TYPICAL FINDINGS OF COVID-19
Description of findings
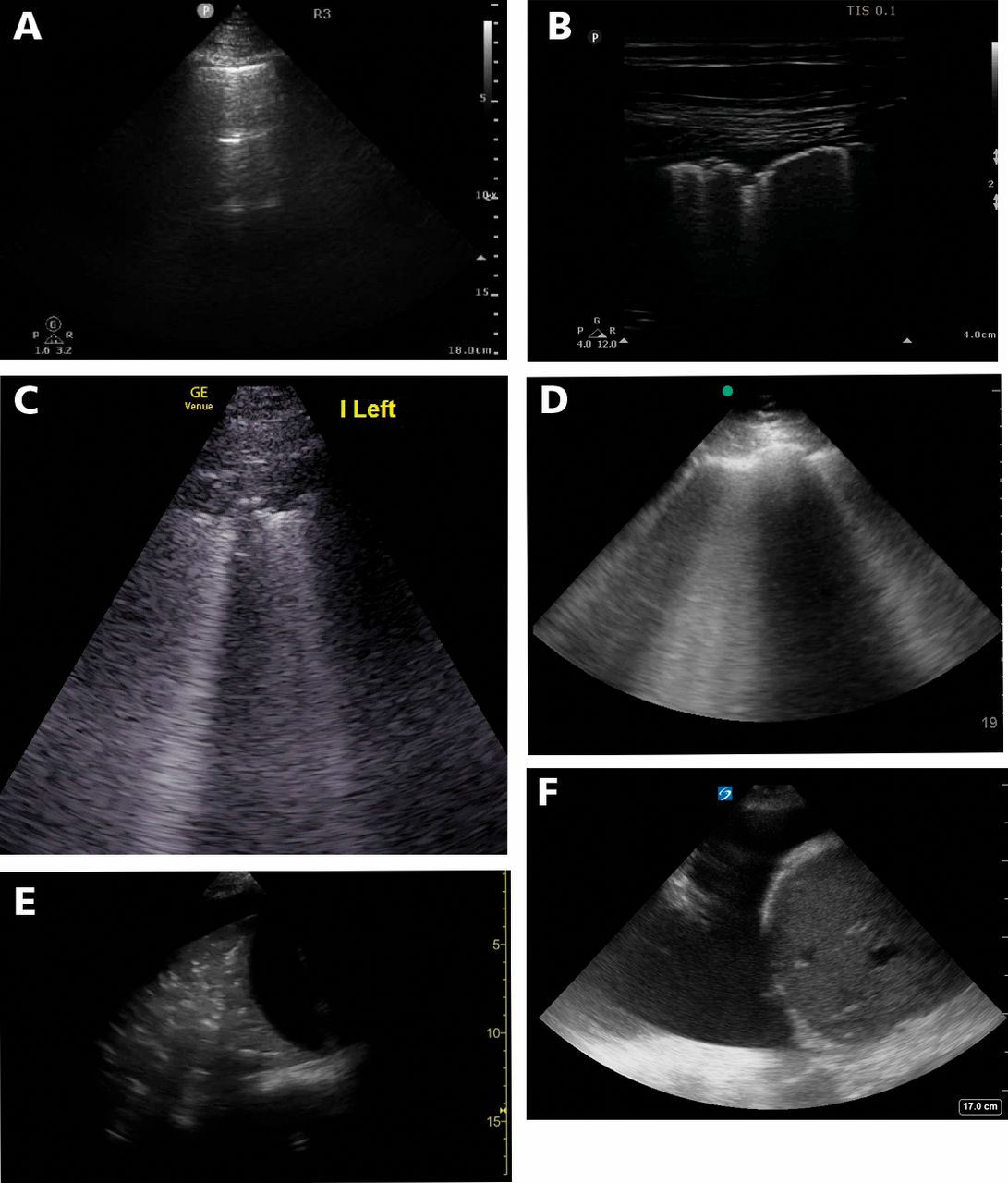
Typical lung patterns seen on ultrasonography in patients with COVID-19 infection include the following (Figure 1)3:
Pleural irregularity and thickening (early finding)
Subpleural consolidations
B lines may be seen, often derived from areas of irregular pleura; these become more confluent and diffuse as the disease progresses.
Spared areas (a pattern of normal lung interspersed between focal B lines) are usually present early in the disease
Nonlobar and translobar consolidation with air bronchograms
Small localized pleural effusions may be seen, but moderate or large basilar pleural effusions are rare.
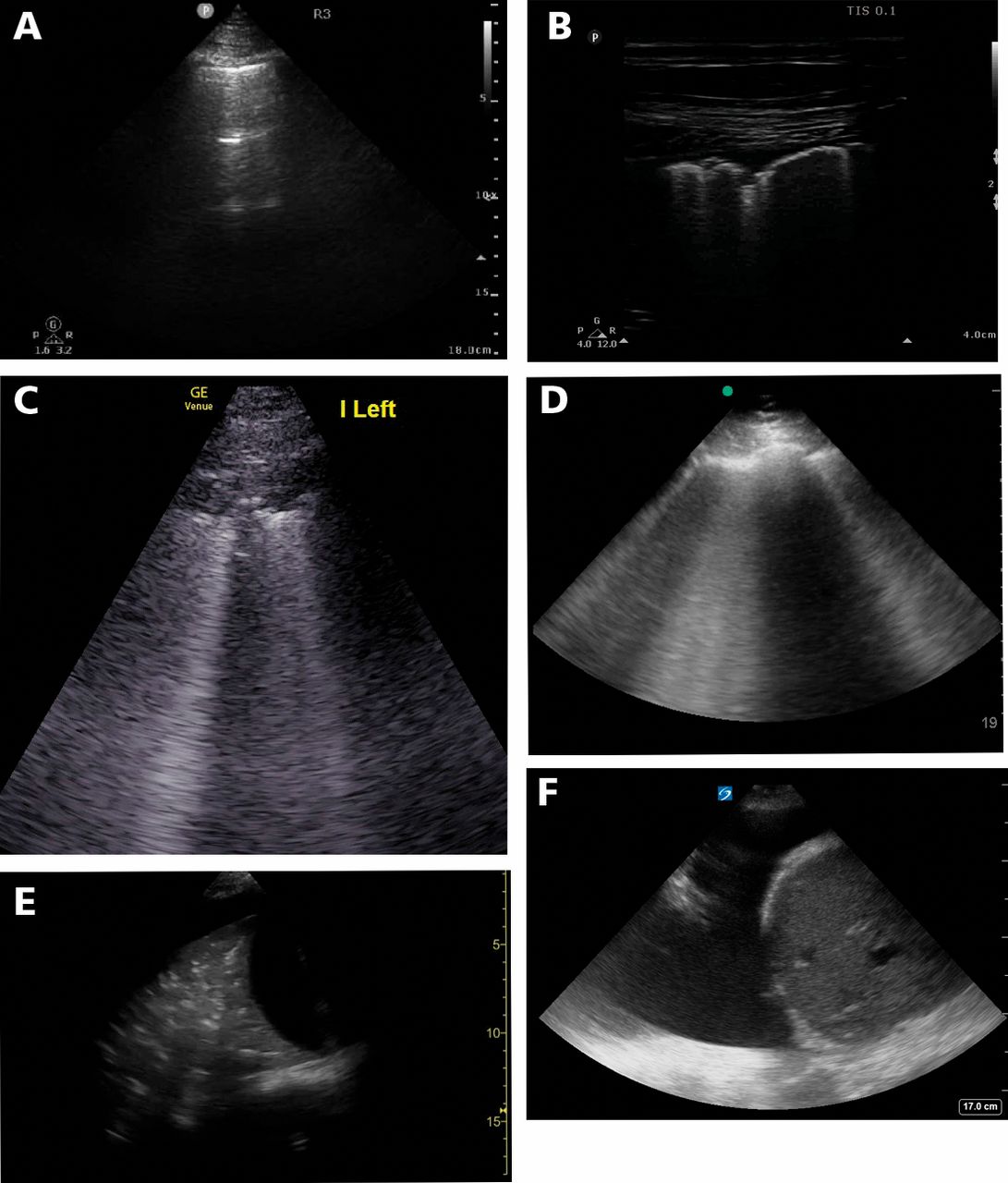
Relevant lung ultrasound findings in patients with COVID-19 infection. A: An “A pattern” as shown here may be present in multiple lung zones in patients with COVID-19; this may be referred to as a “spared area.” B: Pleural irregularity and B lines; in early COVID-19 infection, B lines appear from areas of pleural irregularity or subpleural consolidation. C: Subpleural consolidation, as characterized by an irregular, typically hypoechoic area just beneath the pleura, often with B lines deep or adjacent to it. D: B lines become progressively more frequent and confluent as the extent of interstitial edema progresses; this appearance is similar to that of acute respiratory distress syndrome of any cause. E: Large basilar consolidation, with air bronchograms, and a subpulmonic effusion. F: Large pleural effusion; this is not typical of COVID-19 infection in isolation.
Findings are nonspecific
These lung ultrasound findings are not specific to COVID-19 and are seen in other pneumonias (viral and bacterial) and inflammatory pneumonitis. Severe cases of COVID-19 are similar in appearance to acute respiratory distress syndrome from other etiologies. The findings differ from cardiogenic pulmonary edema, which is frequently characterized by bilateral lower-lobe-predominant B lines with smooth pleura. Alternatively, lack of lung ultrasound findings consistent with COVID-19 infection in acute respiratory failure may suggest an alternative etiology.
POTENTIAL APPLICATIONS OF LUNG ULTRASOUND
Increased diagnostic sensitivity
The importance of correctly identifying patients with COVID-19 is imperative for management and isolation because a false-negative COVID-19 test result may lead to a false sense of security and increase the risk of exposure. Chest computed tomography has been used in several settings as part of the rule-out process due to its high sensitivity (98%, vs 70% for reverse transcription polymerase chain reaction testing).4 However, this approach is associated with high resource use and risk of caregiver exposure.
One study reported a strong concordance between chest computed tomography and lung ultrasound performed simultaneously in patients presenting with flu-like symptoms.5 The authors of that study suggested using lung ultrasound as an alternative to chest computed tomography for early diagnosis of COVID-19 infection.
Lung ultrasound has been used in Italy during the COVID-19 outbreak to facilitate appropriate resource utilization, including testing.6 The broad application faces challenges including concern for false-negative test results, operator variability, clinician time to perform the ultrasound study, and risk of caregiver exposure.
Triage and prognostication
The use of lung ultrasound to triage patients to an appropriate level of care based on the observed abnormality has been suggested.6 Patients with COVID-19 infection who do not have any abnormalities on lung ultrasound and do not require supplemental oxygen can be observed at home. On the other hand, patients with gross lung ultrasound abnormalities or signs that these abnormalities are worsening may require a higher level of care in the intensive care unit as research suggests that there is an association between more prominent lung ultrasound abnormalities and clinical deterioration.7 Thus, lung ultrasound has a potential role to play in triage in some settings. However, it cannot be broadly recommended at this time due to a lack of data.
Characterization of disease
Lobar consolidations may raise suspicion for a superimposed bacterial process.6 Patients with well-aerated anterior lung may derive greater benefit from proning.8 Lung ultrasound can estimate lung recruitment with positive end-expiratory pressure in acute respiratory distress syndrome.9 However, use of lung ultrasound for ventilator titration cannot be broadly recommended in patients with COVID-19 infection due to limited added benefit and the need for frequent examinations, which increases the risk of exposure and disease spread.
Mild to moderate cases of COVID-19 infection have a similar pattern to nonlobar pneumonias (atypical, interstitial, or bronchopneumonia) (Table 1). Severe cases of COVID-19 have more dense or confluent B lines and have a pattern similar to acute respiratory distress syndrome. Cardiogenic pulmonary edema has a distinct pattern distinguished by smooth pleura, intact sliding, and the absence of subpleural consolidations and spared areas. Lobar pneumonia has a distinct pattern distinguished by large lobar consolidations with air bronchograms. Key distinguishing features are shown in bold.
Sonographic findings in pulmonary edema, COVID-19 viral pneumonia, and bacterial pneumonia
OTHER APPLICATIONS OF POINT-OF-CARE ULTRASOUND
Focused echocardiography
The mortality rate in critically ill patients with COVID-19 infection has been suggested to be > 20%, with a high incidence of shock.10,11 The shock syndrome in this group can be distributive, from sepsis or vasoplegia (eg, due to sedation).12 The presence of elevated troponin in the setting of pre-existing cardiovascular disease is associated with significant mortality (69.44%). In one study, the overall mortality in critically ill patients with elevated troponin levels was 59% compared with 8.8% in patients with no elevation.13 Acute cardiac injury may occur due to demand ischemia, acute fulminant myocarditis, worsening of pre-existing myocardial disease, acute coronary syndrome due to plaque rupture, or acute right ventricular failure (due to thromboembolism or pulmonary vasoconstriction from acute lung injury and high ventilator pressures).14
The varied causes of shock necessitate close monitoring of cardiovascular function.11 Focused echocardiography should be performed in patients who are in a state of shock to assess left ventricular systolic function and right ventricular size and function. It should also be used in these patients for basic assessment of cardiac valve function and regional wall-motion abnormalities. Noninvasive cardiac output estimation using left ventricular outflow tract velocity time integral may further guide the evaluation of shock. The need for conservative fluid management in patient with acute respiratory distress syndrome necessitates assessment of dynamic volume responsiveness and volume tolerance before fluid administration.15
Focused echocardiography may influence volume management, ventilator management (for right ventricle protection), assessment of the need for prone-position ventilation, and titration of inotropes and vasopressors.16–18 Point-of-care echocardiography performed by the bedside clinician may obviate the need for comprehensive echocardiography, reducing resource use and risk of infection spread.2
Deep vein thrombosis
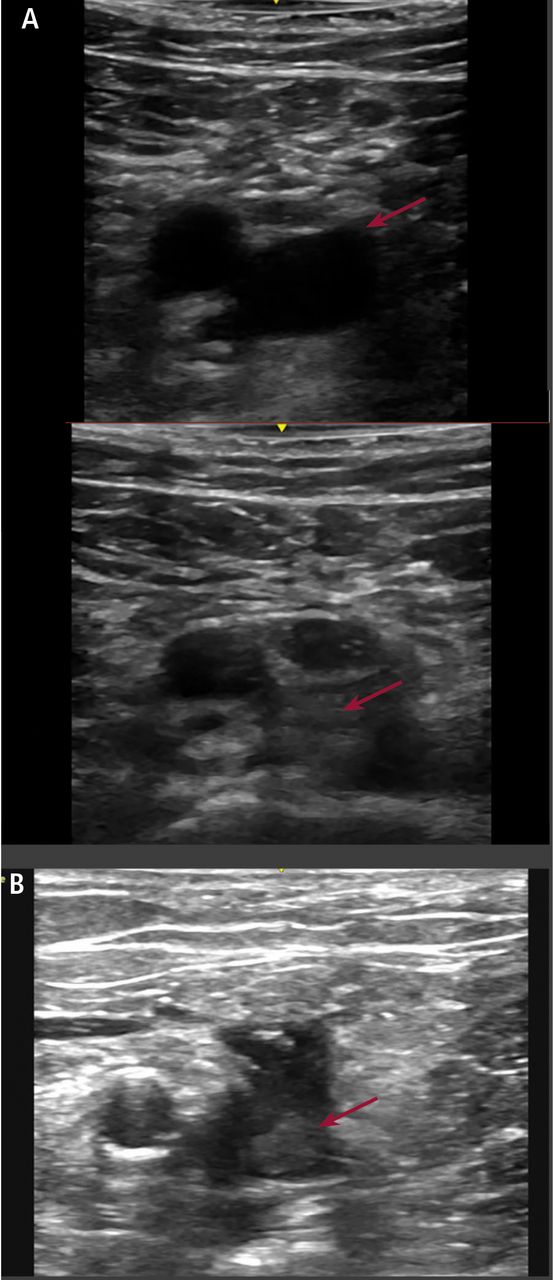
COVID-19 infection is associated with a hyperinflammatory state with a high incidence (20%) of deep vein thrombosis.19 In one study, anticoagulant therapy was associated with a better prognosis in severe COVID-19 infection.20 The sensitivity of limited bedside lower-extremity ultrasound for the diagnosis of deep vein thrombosis (Figure 2) ranges from 84% to 97% and has a specificity of > 95%.21,22

A: Venous compression study at the common femoral vein. The vein appears circular and anechoic in the upper image.
It collapses completely with compression in the lower image. This maneuver rules out clot at this site. The arrow indicates the common femoral vein. B: Intra-luminal echogenic material is seen in the vein at the femoral saphenous junction. The arrow indicates the echogenic clot in the vein. When an obvious thrombus is visible, compression should not be performed due to the theoretical risk of provoking clot embolization.
A “2-point DVT” scan using gray-scale imaging to evaluate vein compression at the common femoral and popliteal veins has been recommended for ease of use but may miss 5.5% of DVT cases.23 A “2-region” technique may be more appropriate and is recommended.24 This involves compression of an area of 1 cm to 2 cm proximal and distal to the greater saphenous vein junction with the common femoral vein extending to the confluence of the deep and superficial femoral vein, and of a second area behind the knee extending from the proximal popliteal vein to the confluence of the calf vein. In case the clinical suspicion for a DVT remains high despite a negative study result, a comprehensive ultrasound study performed by a vascular technician should be obtained.
Procedural
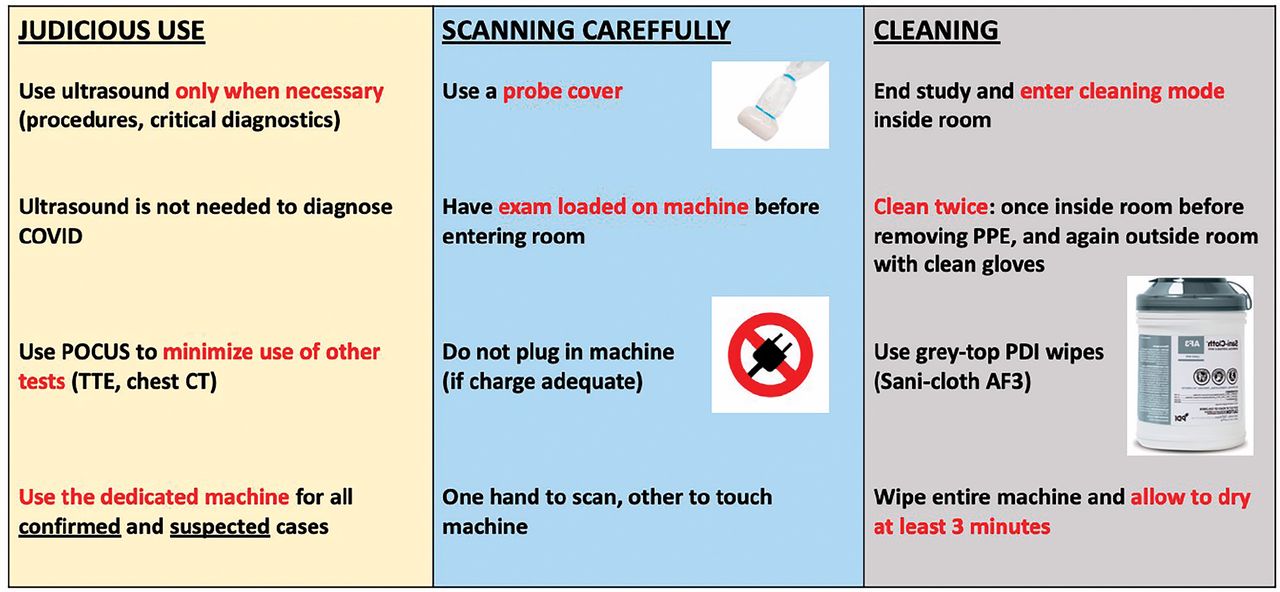
Multiple professional society guidelines recommend using ultrasound for central venous catheter and arterial catheter placement to improve the safety and success rate of the procedure.25 Use of point-of-care ultrasound for procedural guidance is strongly recommended, even in facilities that do not use it diagnostically in patients with COVID-19 infection. Figure 3 provides guidance on the use of ultrasound machines for patients with confirmed or suspected cases of COVID-19 infection.
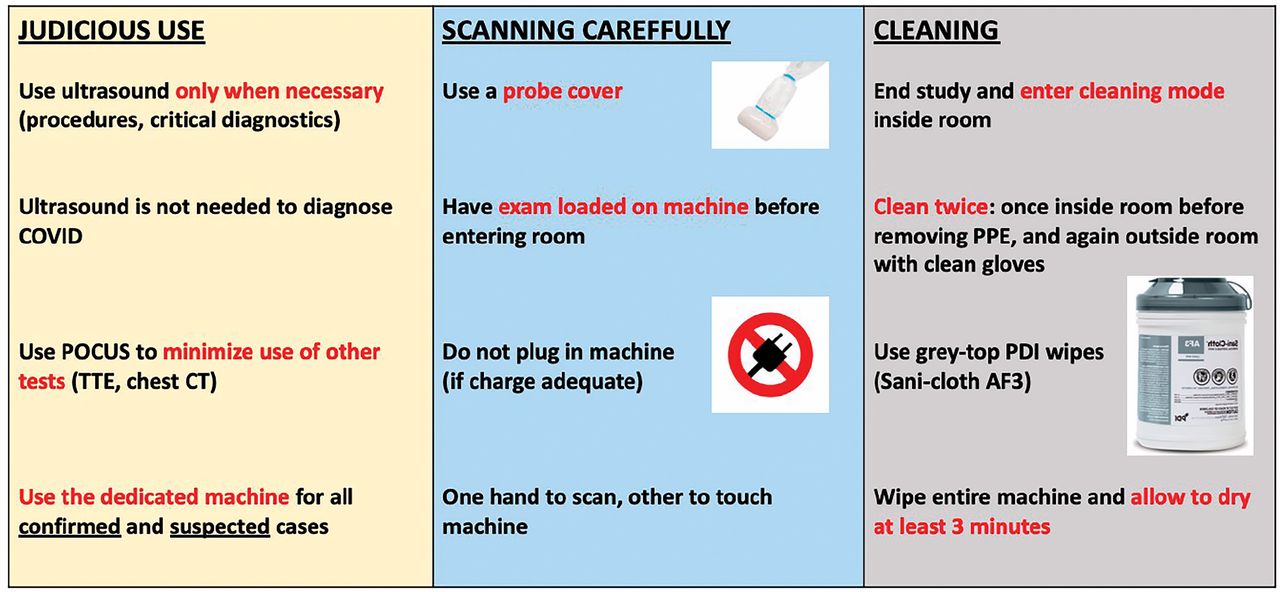
Guidance for use of ultrasound machines for patients with confirmed or suspected COVID-19.
DISINFECTION PROTOCOL
It is of the utmost priority that ultrasound not spread COVID-19 infection. Several guidelines have been developed for disinfection of ultrasound machines.26,27
A few key points are described here:
Each institution should have a cleaning protocol for machines prior to use on COVID-19 patients.
Point-of-care ultrasound examinations should only be performed when necessary and should be consolidated during a single visit as much as possible.
An ultrasound machine should be dedicated to patients with suspected or confirmed COVID-19 infection as much as possible. Handheld machines may be easier to clean and their use should be promoted. A probe cover should be used. No extra supplies should be on the machine. The power cord should be removed from the machine if possible.
The machine should be cleaned twice between patients: once with personal protective equipment on, and once with clean gloves after doffing the protective equipment. The cleaning wipe should be a type approved for emerging pathogens by the US Environmental Protection Agency.
Even in patients without particular concern for COVID-19, point-of-care ultrasound should be used judiciously during a pandemic to limit patient contact and fomite transmission from patients with undiscovered viral shedding. Educational scanning should be limited. Extra attention should be paid to rigorous cleaning of ultrasound machines between patients.
DOING THIS IN PRACTICE: THE DLETE PROTOCOL
A major challenge, particularly amidst increasing staffing demands, is the time required to perform the point-of-care ultrasound exam. A protocol (Figure 4) called DLETE (DVT, lung, echo ten-minute exam) has been developed that shows caregivers how to asses COVID-19–positive patients for deep vein thrombosis as well as for lung and heart abnormalities in 10 minutes. The protocol may be utilized on admission to the intensive care unit and combined with physical exam. The full study or individual components may be repeated later in the event of hemodynamic decompensation.

The DLETE COVID-19 point-of-care ultrasound protocol. The examination for deep vein thrombosis is performed with the linear probe, and lung and cardiac exams are performed with the phased array probe.
SUMMARY
Point-of-care ultrasound has an important role in the management of patients with COVID-19 infection. Because the utility of each application varies by setting, individual institutions should consider how they can best use ultrasound within their specific environments. In general, procedural guidance and focused echocardiography are high yield. Lung ultrasound has the potential to aid the diagnosis and management of patients with COVID-19 infection. Lower extremity point-of-care ultrasound for deep vein thrombosis may help guide decision making regarding anticoagulation or undifferentiated shock. It is of the utmost priority that ultrasound not spread infection, so point-of-care ultrasound must be used only when clinically indicated. Institutions should have protocols for machine disinfection.
APPENDIX RESOURCES FOR FURTHER LEARNING
Learning Modules
Cleveland Clinic MyLearning
Ultrasound Leadership Academy
ultrasoundleadershipacademy.com/academy/#/bt_section5e78dfc6d9af6
Footnotes
The statements and opinions expressed in COVID-19 Curbside Consults are based on experience and the available literature as of the date posted. While we try to regularly update this content, any offered recommendations cannot be substituted for the clinical judgment of clinicians caring for individual patients.
- Copyright © 2020 The Cleveland Clinic Foundation. All Rights Reserved.




{kind=link}
{kind=link}
{kind=link}
{kind=link}