


No. The early repolarization pattern on electrocardiography (ECG) in asymptomatic patients is nearly always a benign incidental finding. However, in a patient with a history of idiopathic ventricular fibrillation or a family history of sudden cardiac death, the finding warrants further evaluation.
DEFINING EARLY REPOLARIZATION
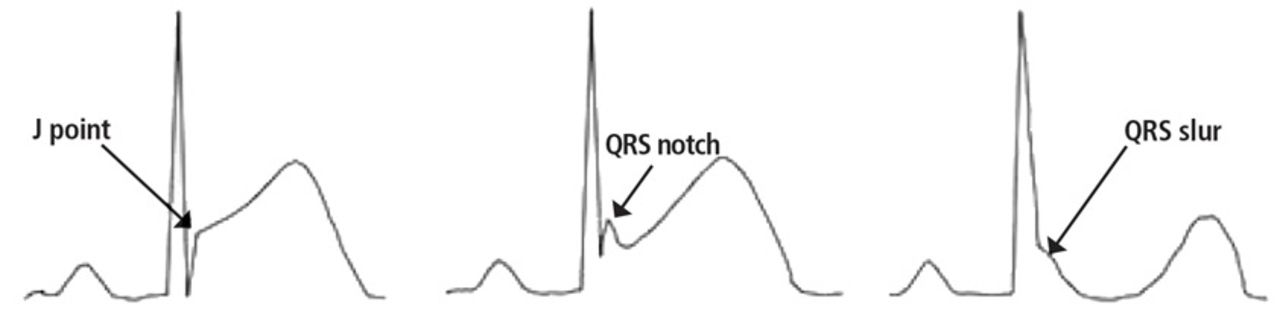
Published studies differ in their definitions of the early repolarization pattern. In 2016, Pat-ton et al described it as ST-segment elevation in the absence of chest pain, with terminal QRS slur or terminal QRS notch.1 However, Mcfarlane et al2 described it as a J-point elevation of at least 0.1 mV in 2 or more contiguous leads on 12-lead ECG, excluding leads V1 to V3, with the presence of terminal QRS notch or slur and QRS duration less than 120 msec. They defined the J point as either the peak of QRS notch or the beginning of QRS slur (Figure 1).2 J-point elevation and QRS notch or slur are most commonly seen in left lateral leads and less often in inferior leads.

Early repolarization with and without QRS notch or slur.
The early repolarization pattern may mimic patterns seen in myocardial infarction, pericarditis, ventricular aneurysm, hyperkalemia, and hypothermia,1,3 and misinterpreting the pattern can lead to unnecessary laboratory testing, imaging, medication use, and hospital admissions. On the other hand, misinterpreting it as benign in the presence of certain features of the history or clinical presentation can delay the diagnosis and treatment of a potentially critical condition.
PREVALENCE AND MECHANISMS
The prevalence of the early repolarization pattern in the general population ranges from 5% to 15%; the wide range reflects differences in the definition, as well as variability in the pattern of early repolarization over time.4
The early repolarization pattern is more commonly seen in African American men and in young, physically active individuals.3 In one study, it was observed in 15% of cases of idiopathic ventricular fibrillation and sudden cardiac death, especially in people ages 35 to 45.4 While there is evidence of a heritable basis in the general population, a family history of early repolarization is not known to increase the risk of sudden cardiac death.
A proposed mechanism for the early repolarization pattern is an imbalance in the ion channel system, resulting in variable refractoriness of multiple myocardial regions and varying excitability in the myocardium. This can produce a voltage gradient between myocardial regions, which is believed to cause the major hallmarks of the early repolarization pattern, ie, ST-segment elevation and QRS notching or slurring.3
Early repolarization: High-risk features
Although the mechanistic basis of ventricular arrhythmia in patients with early re-polarization is still incompletely understood, certain associations may help define the ECG phenotype that suggests increased risk of sudden cardiac death (Table 1).
MANAGEMENT
The early repolarization pattern is nearly always a benign incidental finding on ECG, with no specific signs or symptoms attributed to it. High-risk features on ECG are associated with a modest increase in absolute risk of sudden cardiac death and warrant clinical correlation.
In the absence of syncope or family history of sudden cardiac death, early repolarization does not merit further workup.2
In patients with a history of unexplained syncope and a family history of sudden cardiac death, early repolarization should be considered in overall risk stratification.1 Early repolarization in a patient with previous idiopathic ventricular fibrillation warrants referral for electrophysiologic study and, if indicated, insertion of an implantable cardiac defibrillator for secondary prevention.5
- Copyright © 2019 The Cleveland Clinic Foundation. All Rights Reserved.




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.