


To the Editor: We read with great interest the Clinical Picture report by Rai et al on posterior reversible encephalopathy syndrome (PRES).1 We wish to highlight the lack of universal diagnostic criteria for this condition, especially regarding reversible clinical patterns.2
In the original report by Hinchey et al,3 the presenting neurologic deficit resolved within 2 weeks in all 15 patients, but follow-up imaging was available in only 8. Most of them showed the disappearance of lesions on computed tomography (CT) or magnetic resonance imaging (MRI). Over the years, investigators have proposed other PRES phenotypes, including malignant, hemorrhagic, and atypical variants that might define prognosis and predict recurrence.2
The following case of a young woman with PRES highlights the reversibility of different clinical, radiographic, and electroencephalographic parameters.
An 18-year woman presented with a history of subacute headache and seizures. Her past medical history was relevant for systemic lupus erythematosus, antiphospholipid syndrome, and hypertension. General examination was relevant for hypertension (blood pressure 160/90 mm Hg), and nerologic examination was unremarkable. Her laboratory work revealed normal kidney function (creatinine 0.91 mg/dL, reference range 0.6–1.2). Cerebrospinal fluid analysis revealed a normal opening pressure (12 mm H2O, reference range 5–20), normal glucose level (67 mg/dL, reference range 40–70), and increased proteins (169 mg/dL, reference range 15–45). Leukocytes and erythrocytes were absent.
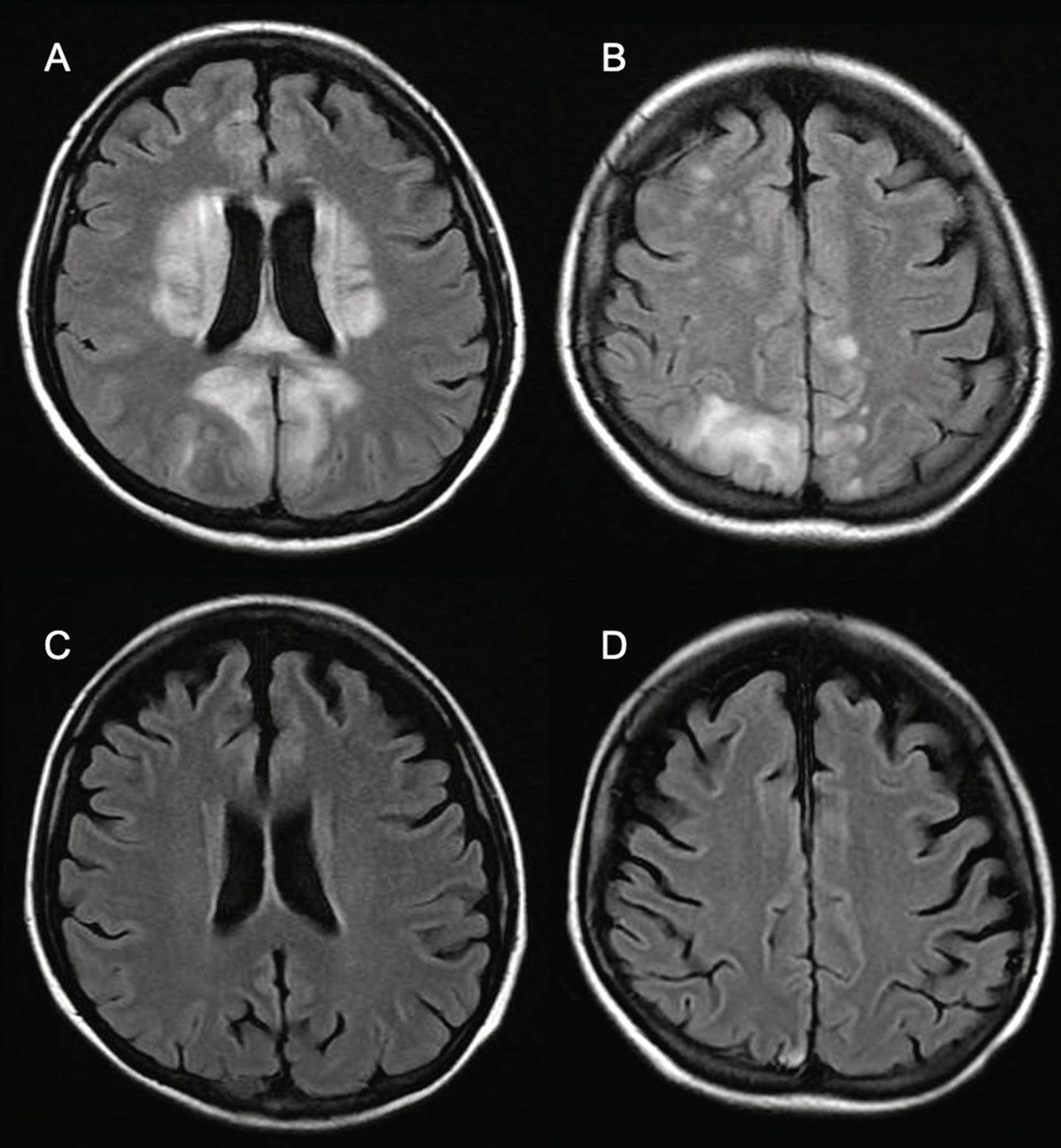
MRI of the brain showed high-signal lesions on the T2 fluid-attenuated inversion recovery (FLAIR) sequence within the cortex and subcortical paraventricular region of both parietal and occipital lobes, with gyral swelling but no associated restricted diffusion (Figure 1A, Figure 1B). No susceptibility artifact to indicate underlying hemorrhage or underlying mass lesions were identified.
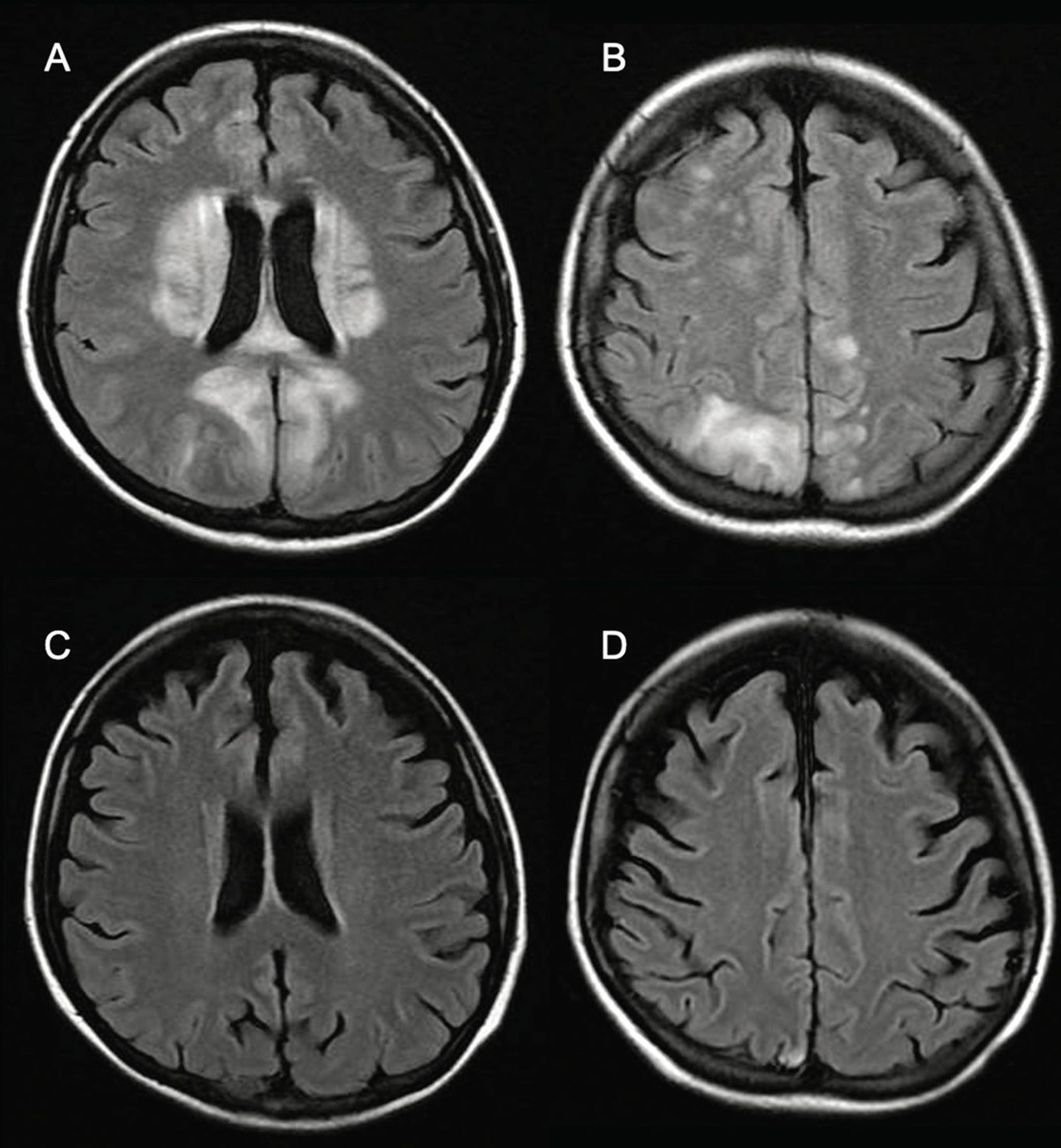
(A, B) Axial fluid-attenuated inversion recovery magnetic resonance imaging (MRI) of the brain showed bilateral cortical, subcortical, and, in the paraventricular region, hyperintense lesions of the parietal and occipital lobes with gyral swelling. (C, D) Follow-up MRI 4 months after presentation showed complete resolution of the lesions.
We initiated levetiracetam, and epileptic activity halted. Headache improved after intense blood pressure control. Electroencephalography (EEG) showed generalized theta-delta range activity with asynchronous activity in the right hemisphere. The patient underwent repeat EEG 4 months after the event, which showed normal alpha rhythm with no underlying background abnormalities. MRI was also repeated at this time, showing the complete reversibility of the described lesions (Figure 1C, Figure 1D).
This case illustrates the reversibility of findings based on imaging and other criteria, including neurologic manifestations and EEG. We suggest these patients may have a better prognosis if all clinical and paraclinical features are reversed and well-documented at short-term follow-up, emphasizing the R in PRES.
- Copyright © 2020 The Cleveland Clinic Foundation. All Rights Reserved.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.