


A 45-year-old man is brought to the emergency department with a self-inflicted forearm laceration. He is incarcerated and under the care of the Department of Corrections (DOC). The patient has a history of self-harm and iron deficiency anemia, and his baseline hemoglobin is 6 to 7 g/dL (reference range 13.0–17.0). On presentation to the emergency department, his vital signs are stable, he has no symptoms of blood loss, and his hemoglobin is 5.2 g/dL. A DOC representative presents a court order that authorizes a blood transfusion when the hemoglobin level is less than 6 g/dL, but the patient refuses the transfusion. As his caregiver, am I obligated to follow the court order against the patient’s wishes?
The caregiver’s obligation is to the patient. An incarcerated patient’s autonomy deserves the same respect as the autonomy of someone not incarcerated. Loss of decision-making autonomy in healthcare is not part of a prison sentence.1,2
As stated by former Associate Justice of the Supreme Court Benjamin Cardozo in Schloendorff v. Society of New York Hospital, “[e]very human being of adult years and sound mind has a right to determine what shall be done with his own body.”3 The real-world application of this principle is rarely straightforward, however.
PIVOTAL STEP: DETERMINE CAPACITY
The first step in any situation involving an incarcerated patient and a court order is to determine the patient’s capacity to make decisions about his or her own care. In this case, the decision is refusal or acceptance of the transfusion authorized by the court. Psychiatric consultation may be helpful when there is comorbid psychiatric disease, but any physician (and in some US states nurse practitioners and physician assistants) who is familiar with the patient is authorized to determine capacity.
Scenario 1
The patient has the capacity to make a decision regarding the treatment outlined in the court order—in this case, a blood transfusion.
A patient who has decision-making capacity has the same right as a nonincarcerated patient to refuse evaluation and treatment, but a court order can complicate the situation, as in the following examples:
A court order has no bearing on the patient’s capacity status. An order that authorizes medical treatment in specific scenarios is not a ruling on a patient’s capacity, nor does its existence imply that the patient does not have capacity.
A court order can be used to override a patient’s right to object to a course of treatment, but it does not mandate the treatment. That is, the presence of a court order does not require a caregiver to act if the caregiver considers the treatment to be inconsistent with the patient’s clearly stated preferences. Even in Washington v. Harper, a 1990 US Supreme
Court case that ultimately mandated antipsychotic treatment of a mentally ill incarcerated individual, the Court wrote that the interests of the incarcerated individual are “adequately protected, and perhaps better served, by allowing the decision to medicate to be made by medical professionals rather than a judge.”4 There are a few scenarios, though, in which a court’s decision may overrule that of the caregiver. (See sidebar, “Exceptions to the rule”).4–6
In our case, the patient’s refusal of a transfusion is unlikely to result in irreversible harm. However, respect for an autonomous patient’s preferences includes respect for their decision even if it is likely to result in death or other irreversible harm. As with nonincarcerated patients, all reasonable efforts should be made to ensure that the patient’s preference is informed, consistent, and congruent with their basic values.
EXCEPTIONS TO THE RULE
If the caregiver elects to go against the patient’s preferences, the court order authorizing the treatment gives the caregiver legal coverage. In general, however, if a patient has the capacity to make the medical decision, the caregiver should respect the patient’s autonomy and the decision. If the caregiver opts not to administer the court-authorized treatment, they should inform their organization’s legal team so they can be prepared should a dispute arise.5
In rare situations, the court has compelled treatment of a patient with decision-making capacity in order to maintain security in a prison setting or to protect the due process of law (Washington v. Harper4 or Saenz v. Wisconsin Department of Corrections6). These circumstances differ from the ones presented in this article, and caregivers outside of DOC facilities are unlikely to face such situations. Additionally, a court order that compels treatment of a specific patient does not compel a specific caregiver to administer that treatment.
Scenario 2
The patient lacks the capacity to refuse the treatment outlined in the court order.
This situation sets in motion a series of steps. The first is to identify the patient’s healthcare power of attorney. If one does not exist or cannot be found, there are other options:
A patient who lacks medical decision-making capacity may still have the capacity to designate a power of attorney. If the patient lacks the capacity to identify a surrogate, state-specific hierarchies of family members should be contacted,7 and incarceration does not change or exclude this hierarchy. If it is technically feasible and medically necessary, the surrogate decision-maker should be allowed access to the patient in order to make appropriate medical decisions even if such visitation would not normally be allowed.8
If no surrogate can be identified or contacted, caregivers must move forward with what they believe is in the patient’s best interest. Correctional officers do not become the surrogate decision-makers and do not have the authority to make medical decisions for people in their custody. This is true for patients in all healthcare settings, including healthcare facilities within correctional institutions. As with patients who are not incarcerated, the default assumption is that a patient would want to be evaluated and treated.
In this setting—ie, the patient lacks the capacity to make the decision and name a surrogate, there is no surrogate decision-maker, and a court order instructs treatment—the caregiver is still not obliged to order the treatment and may choose not to follow a court order that they feel is medically unnecessary. On the other hand, if the caregiver does feel that the treatment is in the patient’s best interest, the court order gives the caregiver legal protection to treat even when it is against the patient’s wishes.
Scenario 3
The patient lacks decision-making capacity and physically resists treatment the caregiver believes is necessary.
When a patient who lacks decision-making capacity physically resists treatment the caregiver believes is needed, the same process should be followed as for other patients, using necessary mechanisms to ensure safety.8 Sometimes this requires sedation, which is emotionally challenging even when it is used for a nonincarcerated patient. Given the additional complexities surrounding the care of incarcerated patients, forcing sedation may feel ethically questionable. Caregivers may opt to consult their legal teams or ethics committees for input in these cases. This is unnecessary, however, if the patient has been determined not to have capacity to make the decision.
OTHER CHALLENGES
When providing care in correctional settings, caregivers must abide by rules set by DOC authorities. These rules may include limiting the amount of information provided to the patient or requiring that the patient be restrained. The need to abide by the rules of correctional authorities may be reasonable, but the rules can complicate the delivery of medically appropriate care. Caregivers have the right to challenge the rules, but under the current system, final decision-making power lies with correctional employees. Further challenges may occur if caregivers feel pressure from correctional officers to make specific decisions. In these instances, it is prudent to involve the legal team or ethics committee.
In the case of a life-threatening emergency, when there may not be time to clearly assess the patient’s capacity or preferences or when an appropriate surrogate cannot be found, the default position should be to avoid irreversible decisions and preserve the patient’s life until a more thorough assessment can be made. In the absence of sufficient information, it is reasonable to assume that most patients prefer life to death, so a decision to treat is still based on the best guess of the patient’s likely preference.
THE BOTTOM LINE
The United States incarcerates more people per capita than any other country.7 Caregivers in all specialties and all settings should be aware of their roles in caring for this large and vulnerable group, especially as the incarcerated population is aging rapidly and will require more medical care.9,10 Indeed, incarcerated individuals are among the few Americans who possess a constitutional right to healthcare.8
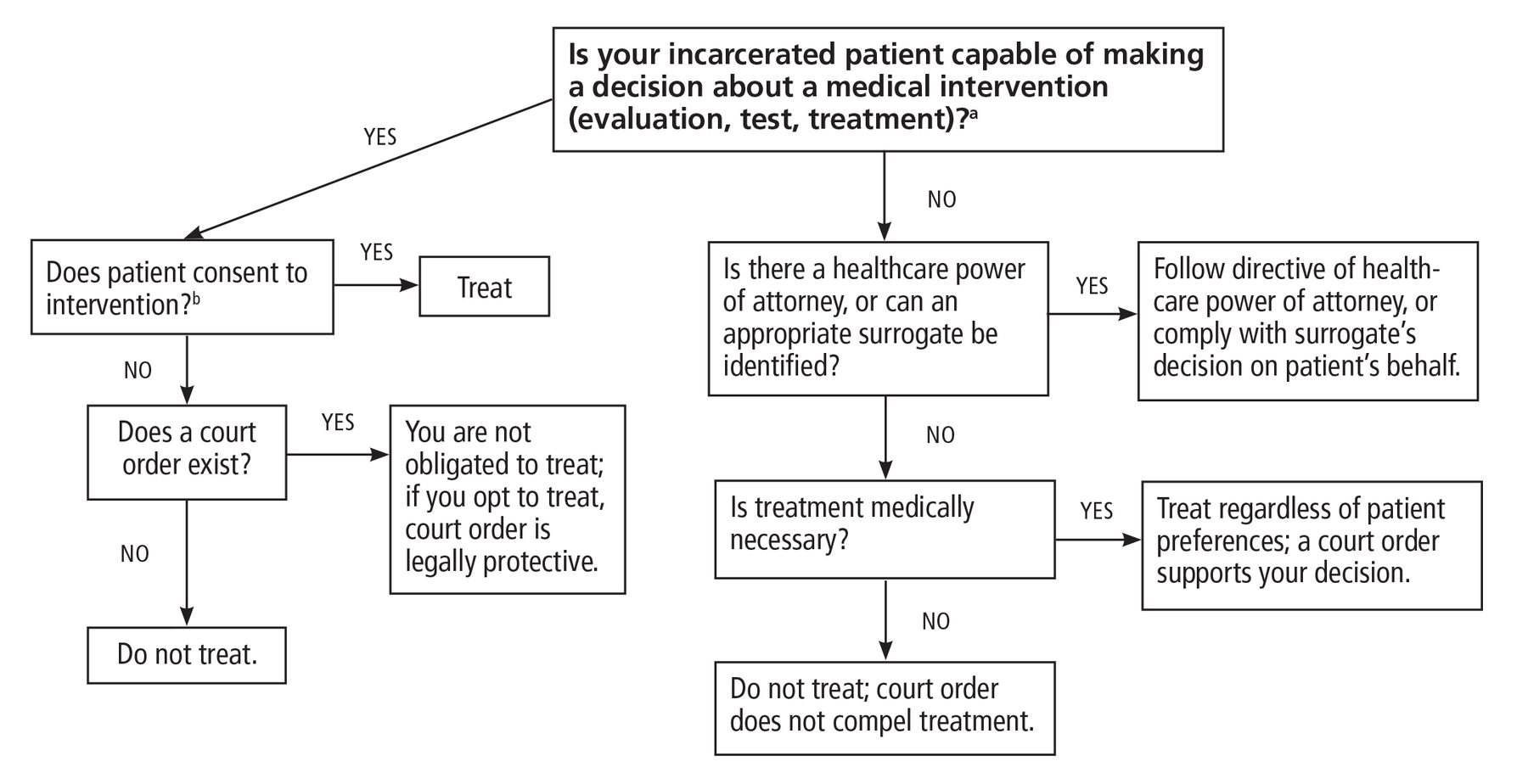
Caring for patients who are incarcerated can create complex, uncomfortable situations. These cases are easier to navigate with the use of a decision-making tool (Figure 1) and awareness that patients who are incarcerated have the same rights of self-determination as those who are not. A prison sentence, a jail sentence, or a court order does not abolish an individual’s entitlement to or refusal of healthcare.
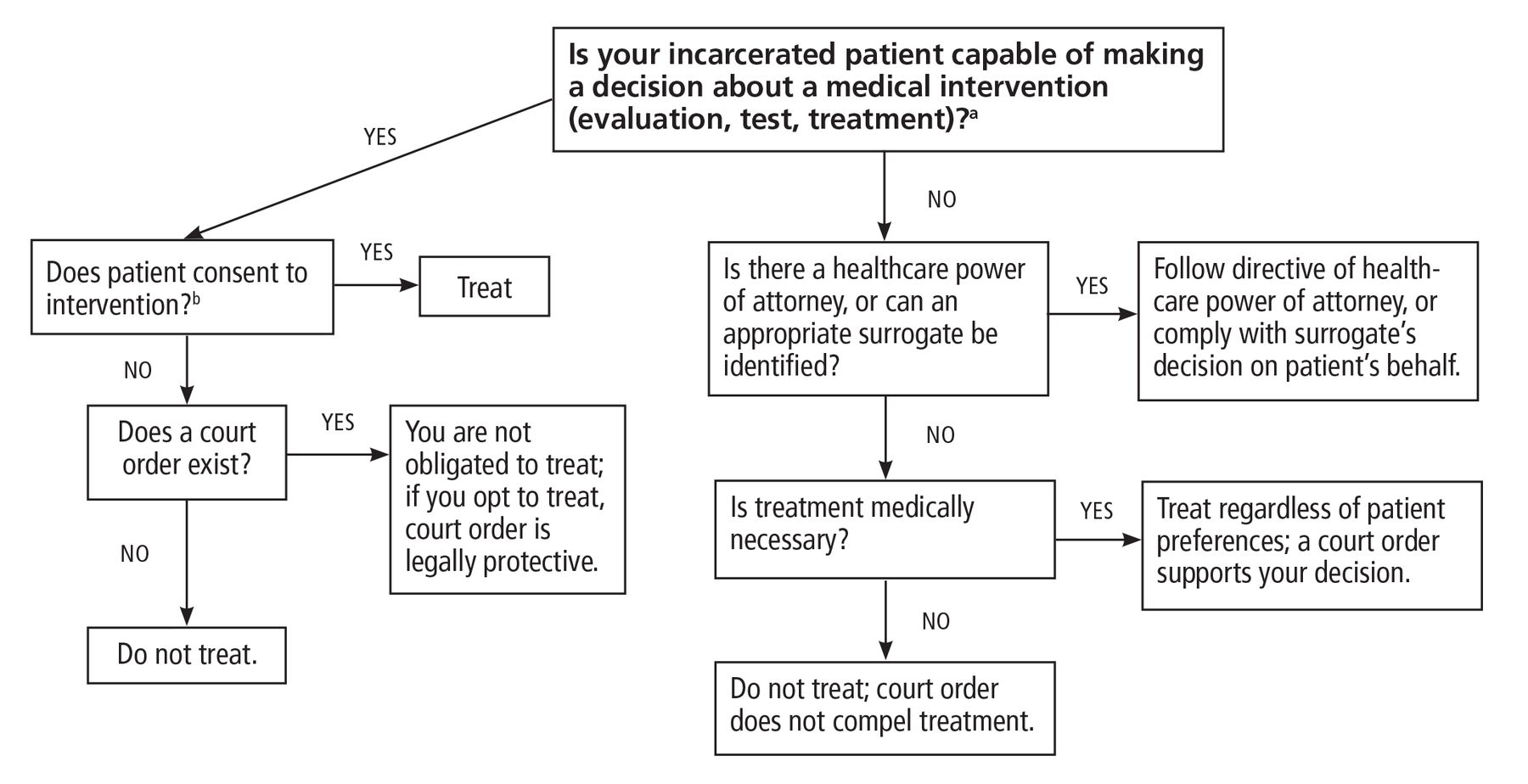
Navigating healthcare of an incarcerated patient.
aAny physician, and in some US states nurse practitioners and physician assistants, can determine capacity.
bThis applies for medical evaluations, diagnostic tests, and treatments.
RETURNING TO THE INITIAL CASE
This incarcerated 45-year-old patient consistently refused transfusion despite conversations with multiple caregivers. Although his hemoglobin was lower than the court-noted threshold, it was not greatly reduced from his baseline, and he was asymptomatic. The patient’s stability allowed time for a thorough capacity evaluation, which was done with psychiatric assistance due to his history of self-harm.
The patient was able to state his reasons for refusal: “I don’t want someone else’s blood inside of me … [and] there is a shortage of blood in the world; my blood can regenerate, it has before.” He denied suicidal ideation and was deemed to have the capacity to refuse transfusion. Ultimately, the transfusion was deferred despite the court order.
DISCLOSURES
The authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
Acknowledgments
The authors would like to acknowledge Joe Hanes, JD, Corporate Counsel at UW Health, Tricia Kvitrud, JD, Senior University Legal Council, University of Wisconsin-Madison, and Shannon Ross, Executive Director of The Community (thecommunitynow.us) for their review of and comments on this manuscript.
- Copyright © 2023 The Cleveland Clinic Foundation. All Rights Reserved.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.