


ABSTRACT
COVID-19 management practices devised for the medical intensive care unit (ICU) are centered on two main goals: ensuring caregiver safety and providing the highest quality patient care through adherence to evidence-based best practices. Rapid, sweeping changes for successful management are based on creating an educational platform to introduce and then further cement these concepts through a unified approach to clinical care. Creating a culture change in a short period of time requires overcoming a host of challenges; however, the result is a more unified and focused approach.
As the COVID-19 pandemic continues, it is essential for healthcare providers to follow updated literature and adapt these to individual institutions. In this review, we describe the COVID-19 management practices devised for the medical intensive care unit (ICU) in the Respiratory Institute at Cleveland Clinic.
The foundation of our ICU operations is centered on two main goals: ensuring caregiver safety, and providing the highest quality patient care through adherence to evidence-based best practices.
ENSURING CAREGIVER SAFETY
We need to preserve our workforce for the health of the community and the functioning of the institution. Identifying the appropriate situations for personal protection equipment (PPE) is essential, so we developed standards of care (Table 1) that outline when and how PPE should be used based on the risk of transmission when in contact with potential COVID-19-positive patients, either confirmed or under investigation for infection. Equipment includes a surgical mask, gown, protective eyewear, and gloves for all caregiver interactions. An N95 respirator or a powered air-purifying respirator (PAPR) is used for encounters with patients undergoing therapies at high risk for aerosolization (eg, high-flow nasal cannula [HFNC], noninvasive ventilation [NIV]) or procedures at high risk for disease transmission (eg, intubation, tracheostomy, endoscopy).
Recommendation for personal protective equipment for COVID-19
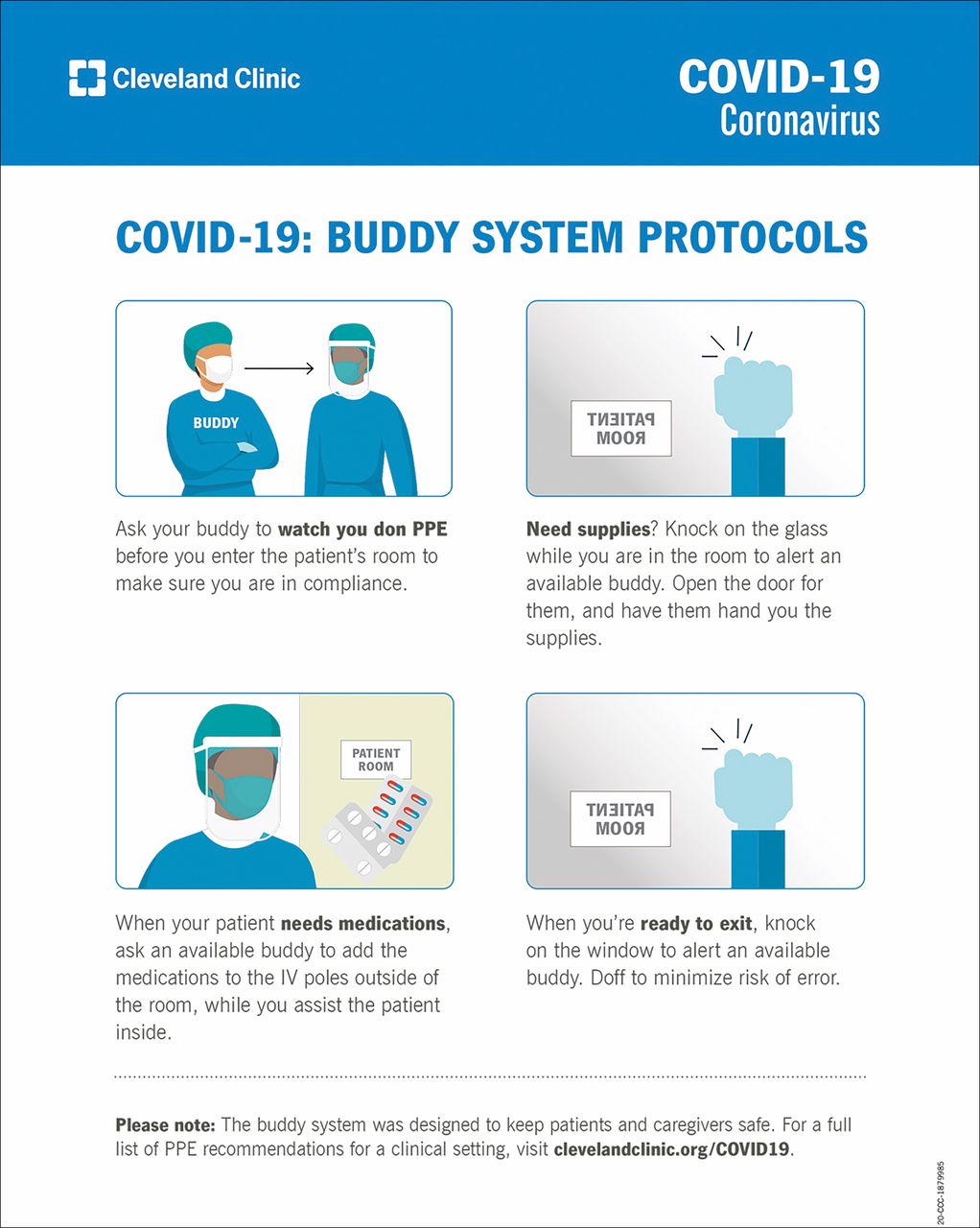
In addition, to reduce the high risk of transmission during the process of donning or doffing PPE, especially when doffing, we instituted a “buddy” system to create an additional layer of caregiver safety (Figure 1). This person provides direct observation and feedback during the process of donning and doffing PPE to ensure caregiver safety.

Cleveland Clinic buddy system protocol.
We also made adjustments to respiratory practices to enhance safety by minimizing aerosolization. For hospitalized patients with COVID-19 who develop hypoxemia, oxygen is supplemented with a target oxygen saturation (SpO2) range of 90% to 96%, and the patients are transferred to the ICU on escalating requirements for closer observation, as they can quickly deteriorate. In patients with increasing oxygen requirements, we prefer HFNC with a surgical mask placed on the patient, as tolerated, to minimize aerosolization. In patients with concomitant comorbid conditions that indicate the use of NIV with either continuous positive airway pressure (CPAP) or bilevel positive airway pressure (BiPAP), such as chronic obstructive pulmonary disease or congestive heart failure, we use expiratory-port high-energy particulate air (HEPA) filters.
We use objective criteria to identify patient deterioration while on noninvasive ventilation (Table 2). Although we do not advocate early intubation, these patients are evaluated often to avoid delaying intubation. In patients who are intubated, we use inline nebulizers. In those not on mechanical ventilation, we use metered-dose inhalers.
Failure criteria for noninvasive ventilation (NIV) and high-flow nasal cannula (HFNC)
Procedures for intubation, if required, have also been modified to ensure caregiver safety. Preoxygenation is achieved with delivery of 100% oxygen via a non-rebreather mask or HFNC; bag mask ventilation is not recommended. We have our most experienced operators use video laryngoscopy to perform intubation to minimize the duration of the procedure and to ensure maximum distance from the patient’s oropharynx. After successful intubation, we put patients directly on mechanical ventilators with continuous capnometer monitoring.
Chest radiography is performed at admission to ensure placement for necessary procedures such as nasogastric tube and central line. However, we avoid daily chest radiography unless clinically indicated, such as when changing location of the endotracheal tube or changing ventilation parameters (eg, increasing resistance, hypoxemia). We developed a process for performing portable radiologic studies from outside the room.
MAINTAIN BEST PATIENT CARE
It is challenging to maintain our standards of care when isolation practices increase. We created a cohort unit in which we place all patients under investigation for or with confirmed COVID-19 to ensure the safety of other patients and our caregivers.
We have 5 distinct medical ICUs. We dedicated 2 of these units (with plans to expand further based on patient volume) to the COVID-19 patient population, either suspected or confirmed. Each patient has his or her own room with four distinct walls.
Given that there is no curative therapy for COVID-19 and that therapeutic considerations have been extrapolated from limited experience, we developed multidisciplinary teams to help develop consistent clinical practice strategies. These teams include ICU providers, infectious disease specialists, and pharmacists.
For hypoxic respiratory failure, our mechanical ventilation strategy includes low tidal-volume-ventilation with a goal end-inspiratory plateau pressure of 30 cm H2O or below and allows for permissive hypercarbia (pH ≥ 7.15). We titrate the fraction of inspired oxygen and positive end-expiratory pressure (FiO/PEEP) according to established protocols.1 It is often easier to use existing evidence-based protocols2 in a pandemic when unfamiliar teams may be caring for these patients. Early proning and neuromuscular blockade are recommended as adjuvant therapy in patients. For patients who are refractory to conventional mechanical ventilation, trials of salvage therapy with inhaled vasodilator and extra-corporeal life support can be considered. After initial volume resuscitation, as patients often come with evidence of volume depletion, we are vigilant in preventing and decreasing volume overload. In patients with acute lung injury, diuresis with the Fluid and Catheter Treatment Trial (FACTT) lite protocol should be implemented.2
Bacterial coinfections have been reported in patients with COVID-19.3 As a preventative measure, we start coverage with antibiotics in critically ill patients presenting with severe respiratory distress, basing it on their risk factors for community versus drug-resistant organisms (eg, MRSA, pseudomonas). Procalcitonin is ordered on admission and followed to help with de-escalation of antibiotic therapy.
Critically ill patients with COVID-19 experience a sequelae of manifestations from activation of the innate inflammatory cascade, which increases the incidence of cardiomyopathy/heart failure, disseminated intravascular coagulation, venous thromboembolism (VTE), and the cytokine-release syndrome. Although there are currently no accepted standardized therapies for the prevention or treatment of these phenomena, we perform screening modalities that include ECG, troponin levels, ferritin, and select serology tests on admission with follow-up based on the patient’s clinical course (Table 3). In patients at high risk for VTE (D-dimer > 3,000 ng/mL FEU), we perform point-of-care ultrasound to assess the presence of thromboembolism over extremities. Therapeutic anticoagulation is indicated for patients with conclusive evidence for VTE.
Cleveland Clinic MICU COVID-19 workup checklist (updated 4/15/2020)
As with any new disease that has unproven therapies, our approach is to develop the best evidence-based guidelines for our teams to follow and to engage in clinical trials to form better guidance.
Bundle care. We also have developed practices to preserve PPEs while maintain our standards of care. We bundle all care (eg, medications at same times, labs, and procedures) and limit traffic into the room to only what is essential. Our nursing and respiratory therapy teams have placed medication administration pumps and ventilator screen outside of patient rooms, which has decreased our PPE use by about 50% to 60%. This placement also allows for more efficient titration of medications and ventilator settings resulting in decreased sedative use and easier adjustment of ventilator support.
To further limit room traffic, we delegate one caregiver to perform a daily comprehensive physical examination with a dedicated single-use stethoscope that remains in the room. The results are documented and shared with all other care and consulting teams to limit entrance. They are repeated based on changes in patient’s clinical condition.
Neurological assessment and skin examination are performed by beside nurses every 2 to 4 hours with other bundled care. All other practices including daily routine lab draws and ancillary support such as physical therapy continue on an essential-only basis.
Family visitation is limited as an infection-control method, but the team has placed special emphasis on maintaining communication with patients and their supporting members. Updates are amended in various fashions based on the provider and patient’s preference to be done outside of the rooms. This involved phone calls, videoconferencing, and in some instances communicating by writing on the glass ICU doors.
Be aware of information overload. Not a minute goes by without a new post, tweet, email, or letter from caregivers at the frontlines with new disease manifestations or unproven therapies. At times, this generates an overwhelming amount of anxiety. We have created an educational team that is responsible for reviewing all available literature and developing an educational platform that serves our teams. This is done through an easily accessible, shared toolkit that allows our caregivers to rapidly find protocols and up-to-date educational resources (eg, webinars, simulations, checklists) especially with rapidly updated guideline. This resource becomes the source of truth for the institution, aligns caregivers, and decreases anxiety from misinformation.
SUMMARY
To deal with COVD-19, we have developed best practices for the ICU to maintain the highest quality patient care while ensuring the safety of all caregivers. This requires rapid, sweeping changes to the system. Success is based on creating an educational platform to introduce and then further cement these concepts through a unified approach to clinical care. Creating a culture change in a short period of time requires overcoming a host of challenges; however, the result is a more unified and focused approach.
Footnotes
The statements and opinions expressed in COVID-19 Curbside Consults are based on experience and the available literature as of the date posted. While we try to regularly update this content, any offered recommendations cannot be substituted for the clinical judgment of clinicians caring for individual patients.
- Copyright © 2020 The Cleveland Clinic Foundation. All Rights Reserved.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.