


A 36-year-old man presented to the emergency department with severe pain in the left upper quadrant. This was preceded by 10 days of nonproductive cough, sore throat, and fever. His female partner had experienced similar symptoms starting 2 days prior to his symptom onset.
Physical examination was significant for erythematous swollen tonsils with white exudates, bilateral tender cervical lymphadenopathy, and left upper quadrant tenderness. The tonsils were touching (ie, “kissing”) (Figure 1). There was no stridor or wheezing, but the patient had difficulty swallowing and tolerating oral secretions.

Image captured at bedside upon arrival to the emergency department showing “kissing tonsils.”
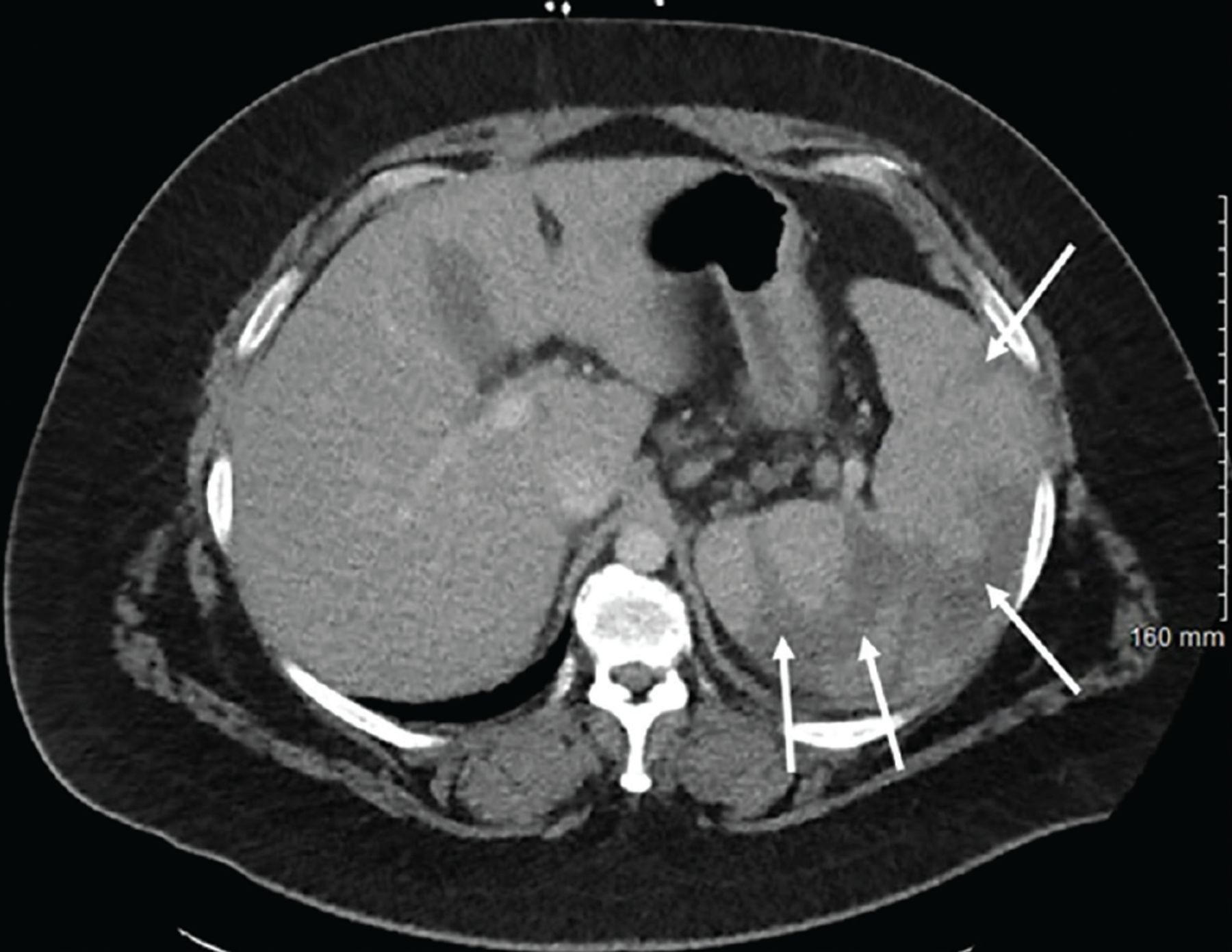
Laboratory studies showed a leukocytosis of 26 × 109/L (reference range 4.0–11.0), with 56% lymphocytes and 11% atypical lymphocytes. Aminotransferases were elevated, with an aspartate aminotransferase 71 U/L (7–30), alanine aminotransferase 92 U/L (11–30), and alkaline phosphatase 119 U/L (16–100). Computed tomography (CT) of the abdomen showed splenomegaly with multiple splenic infarcts (Figure 2).

Axial computed tomography of the abdomen with intravenous contrast shows splenomegaly with multiple acute-appearing splenic infarcts visualized as large, wedge-shaped peripheral areas of non-enhancement (arrows).
A heterophile antibody (“monospot”) test was positive, consistent with acute Epstein-Barr virus mononucleosis. Throat culture later grew beta-hemolytic group C streptococci, which was thought to represent colonization. Given the approximation of the tonsils and difficulty swallowing and tolerating secretions, steroids were initiated, and he was transferred to the intensive care unit for monitoring. He was discharged on hospital day 6 with 5 days of dexamethasone, and 8 weeks later his symptoms had resolved.
DIFFERENTIAL DIAGNOSIS OF TONSILLAR ENLARGEMENT
The differential diagnosis in cases of bilateral tonsillar enlargement in adults includes infection with groups A, C, and G streptococci, Fusobacterium necrophorum, Neisseria gonorrhoeae, Corynebacterium diphtheriae, Toxoplasma gondii, and viral pathogens including Epstein-Barr virus, cytomegalovirus, adenovirus, herpes simplex virus type 1, human herpesvirus type 5, measles, rubella, human immunodeficiency virus, and hepatitis A virus.1,2 Other causes of tonsillar enlargement include malignancy, notably squamous cell carcinoma or lymphoma, although these are less likely to present in the acute setting and are usually unilateral.3 Peritonsillar abscess should be considered, but it is also less likely to have bilateral involvement.4
ASSESSMENT OF TONSILLAR ENLARGEMENT IN INFECTIOUS MONONUCLEOSIS
The typical features of infectious mononucleosis include fever, pharyngitis, lymphadenopathy, and atypical lymphocytosis. Pharyngitis is a relatively common symptom of infectious mononucleosis and is present in an estimated 85% of cases.5,6 Pharyngeal inflammation is often accompanied by tonsillar exudates, which usually appear white or gray.
In rare cases, airway compromise secondary to tonsillar edema may occur, and thus it is important to focus on the patient’s ability to swallow. If the patient is not tolerating oral secretions, emergent consultation with an otolaryngologist should be considered.5
Despite controversy regarding the use of corticosteroids in infectious mononucleosis, corticosteroids are still widely recommended in patients with evidence of significant upper airway obstruction.7 Additionally, intensive airway monitoring should remain a priority in cases of pharyngitis with impending airway obstruction that manifests with tonsillar enlargement, dyspnea, and difficulty tolerating secretions.
SPLENIC INFARCTION IN INFECTIOUS MONONUCLEOSIS
Although splenomegaly may be present in approximately 50% of patients with infectious mononucleosis, splenic infarction is a rare complication, although the exact incidence is not known.8 Splenic infarction may present with a wide range of clinical presentations, ranging from asymptomatic to fatal hemorrhage. Most patients present with left upper quadrant pain on presentation, though in 1 case series, 30% of patients with splenic infarction were asymptomatic.9
Contrast-enhanced CT remains the imaging modality of choice for diagnosis of splenic infarction. It should be noted that abdominal ultrasonography has low sensitivity for acute infarction.9
The pathogenesis of splenic infarction in infectious mononucleosis remains poorly understood, but it is likely multifactorial, resulting from splenic enlargement, alterations in splenic vascular circulation, and a transient prothrombotic state associated with acute infection.10 Splenic infarction is typically managed with supportive care, and patients should be monitored closely to avoid splenic rupture, a rare but serious complication that is estimated to be present in less than 0.5% of infectious mononucleosis cases.11,12 Patients should be advised to avoid contact sports for a minimum of 21 days to avoid this complication.12
DISCLOSURES
The authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
- Copyright © 2023 The Cleveland Clinic Foundation. All Rights Reserved.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.