


Article Figures & Data
Figures
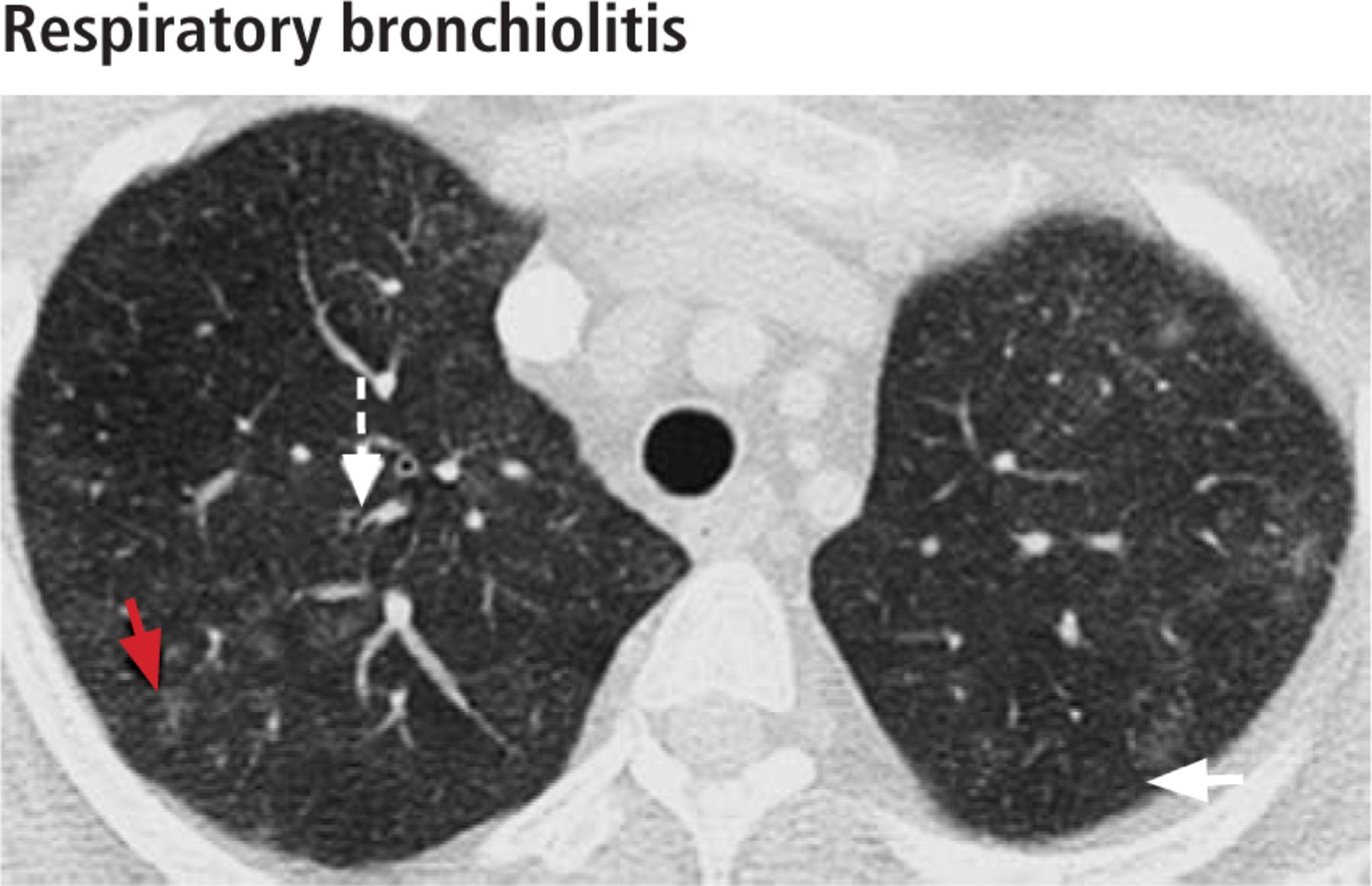
- FIGURE 1
In a 36-year-old woman with an 18-pack-year smoking history, high-resolution CT shows respiratory bronchiolitis in the upper lungs, with bilateral centrilobular ground-glass nodules (red arrow), patchy ground-glass opacities (white solid arrow) and bronchial wall thickening (white dashed arrow).
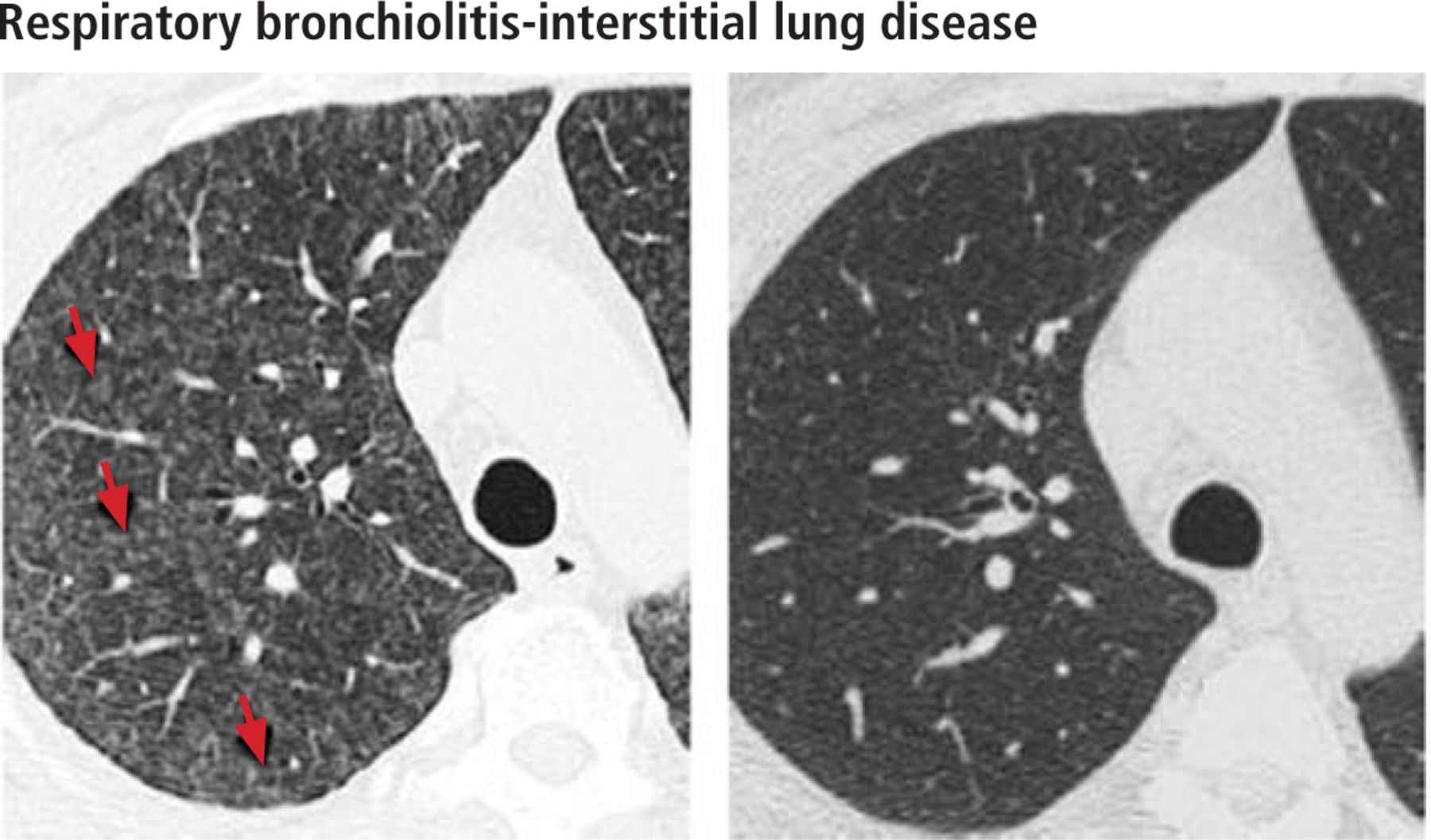
- FIGURE 2
In a 40-year-old woman with a 15-pack-year smoking history with respiratory bronchiolitis-interstitial lung disease, high-resolution CT obtained through the upper lungs at initial diagnosis (left) shows diffuse faint centrilobular ground-glass nodules (red arrows). High-resolution CT 1 year after smoking cessation (right) shows complete resolution of the centrilobular nodules.
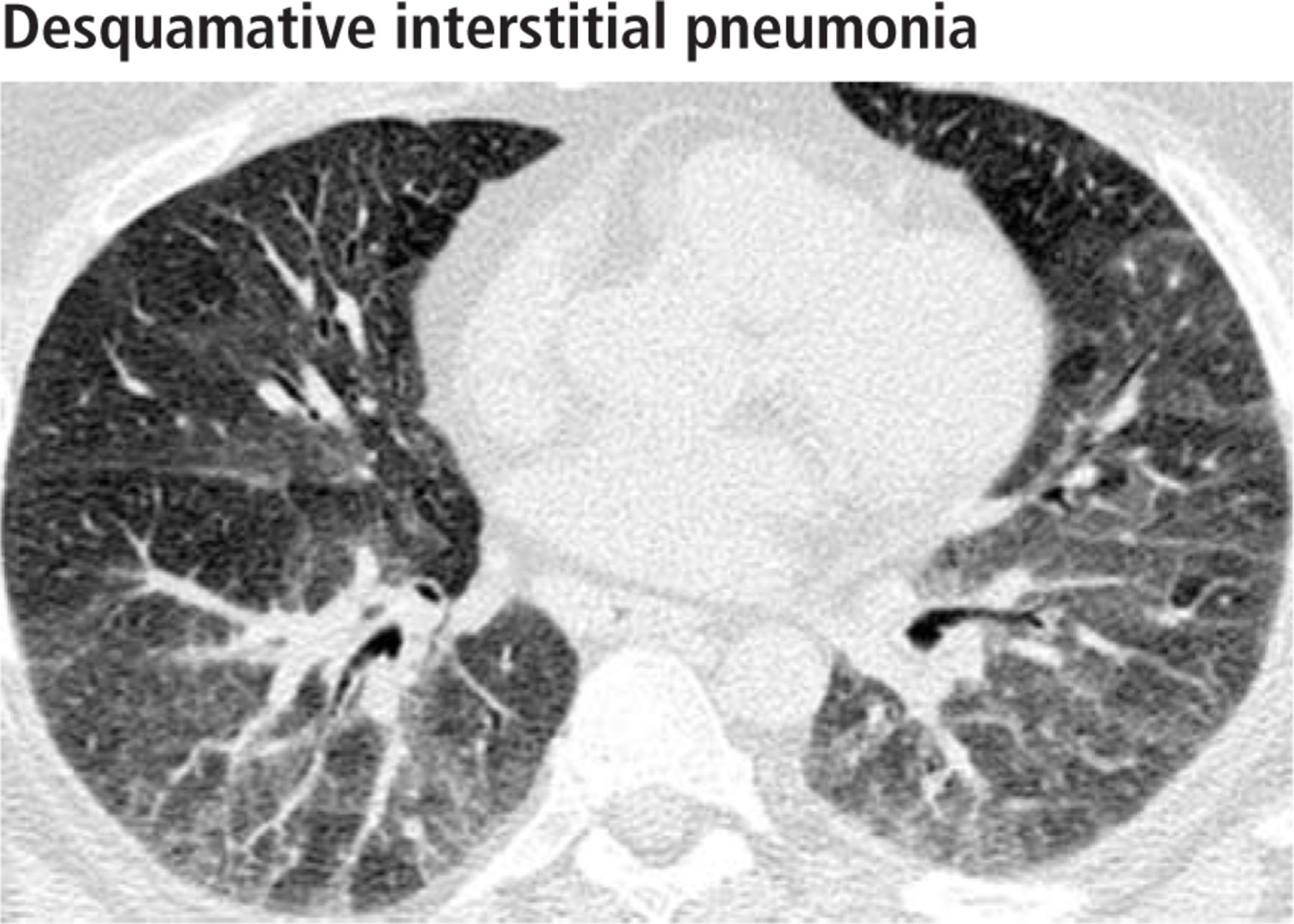
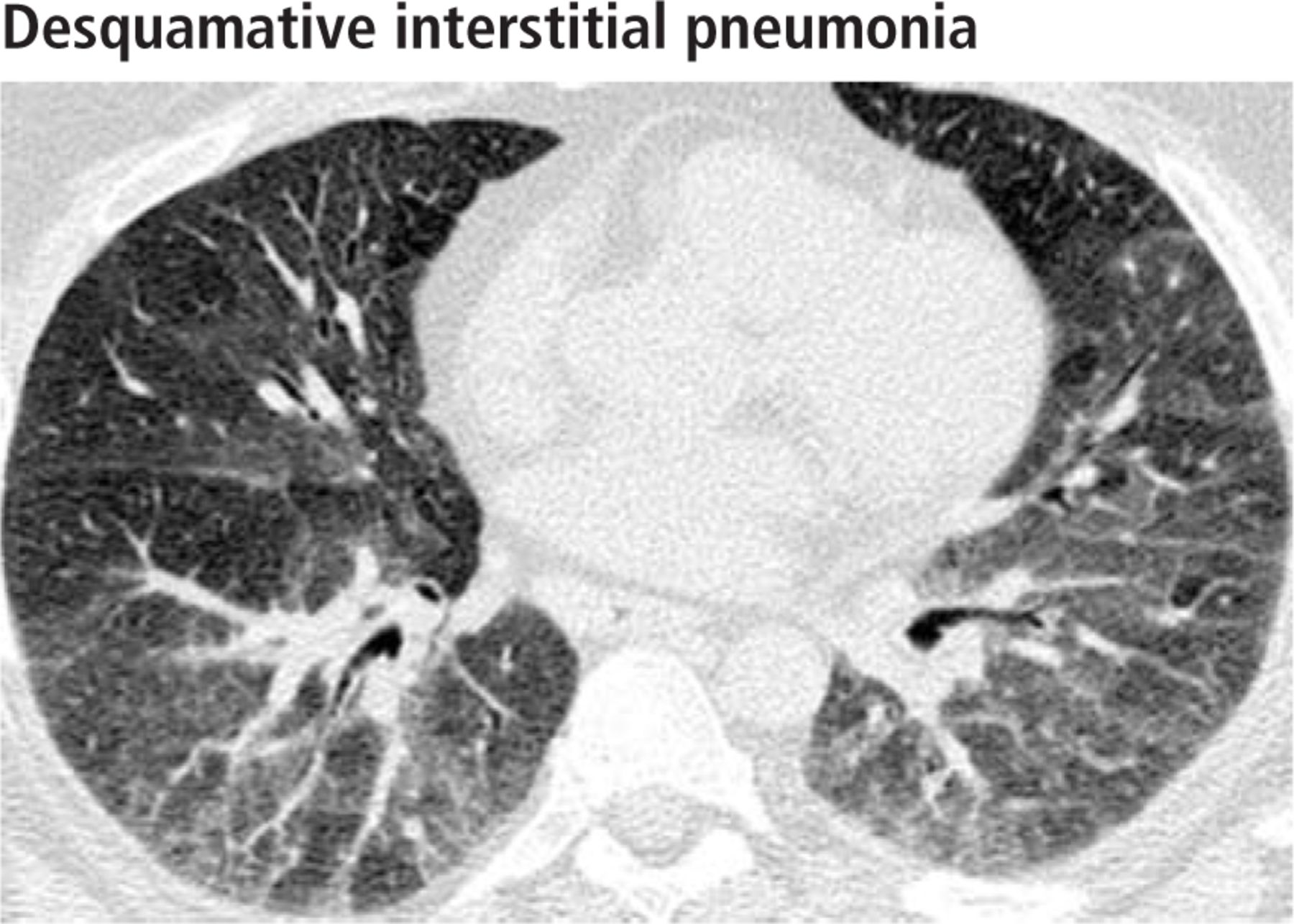
- FIGURE 3
In a 49-year-old woman with a 23-pack-year history of smoking, high-resolution CT obtained through the lower lungs shows features of desquamative interstitial pneumonia: diffuse ground-glass opacities predominantly in the mid-lower lung. No traction bronchiectasis or architectural distortion is seen.
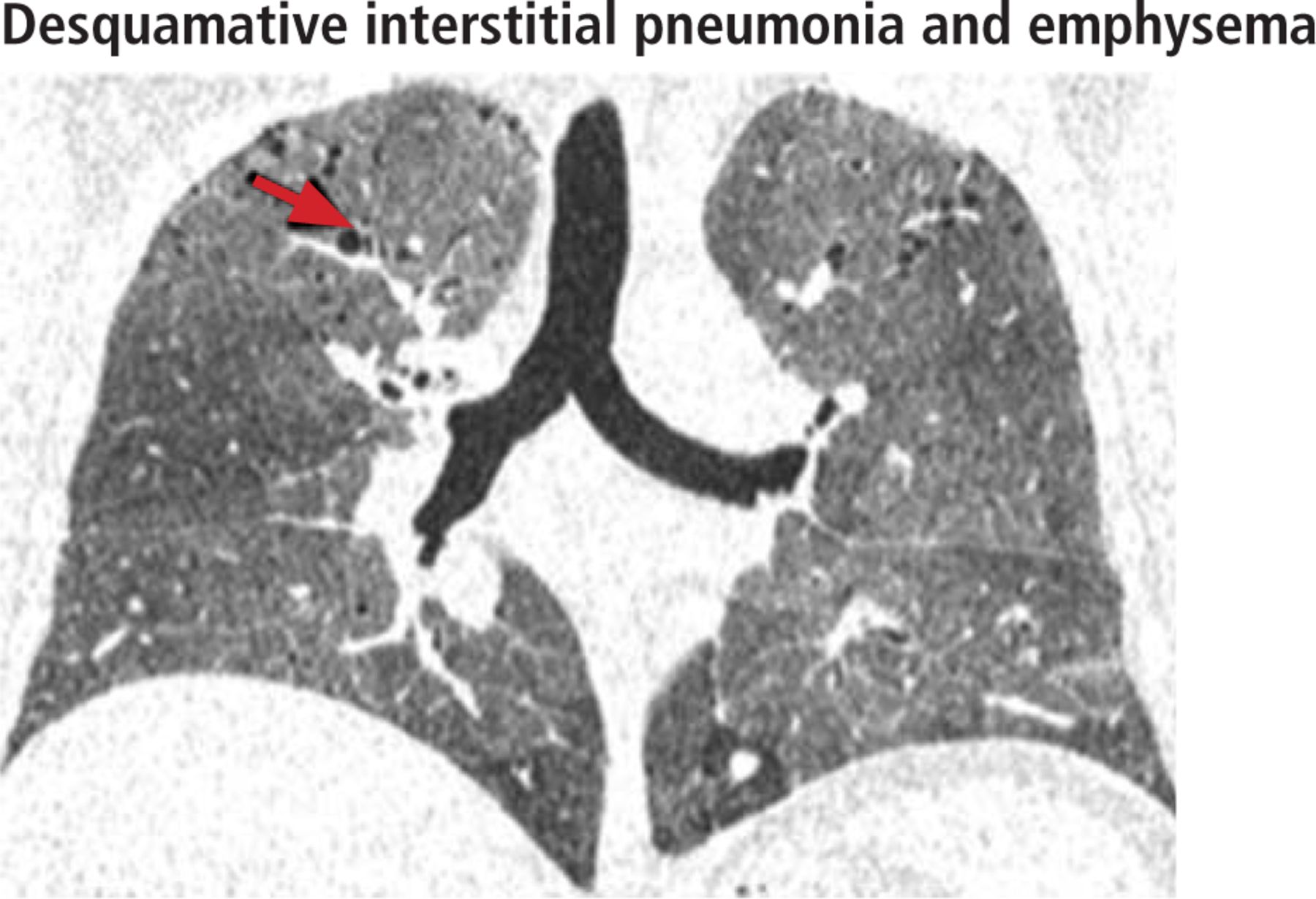
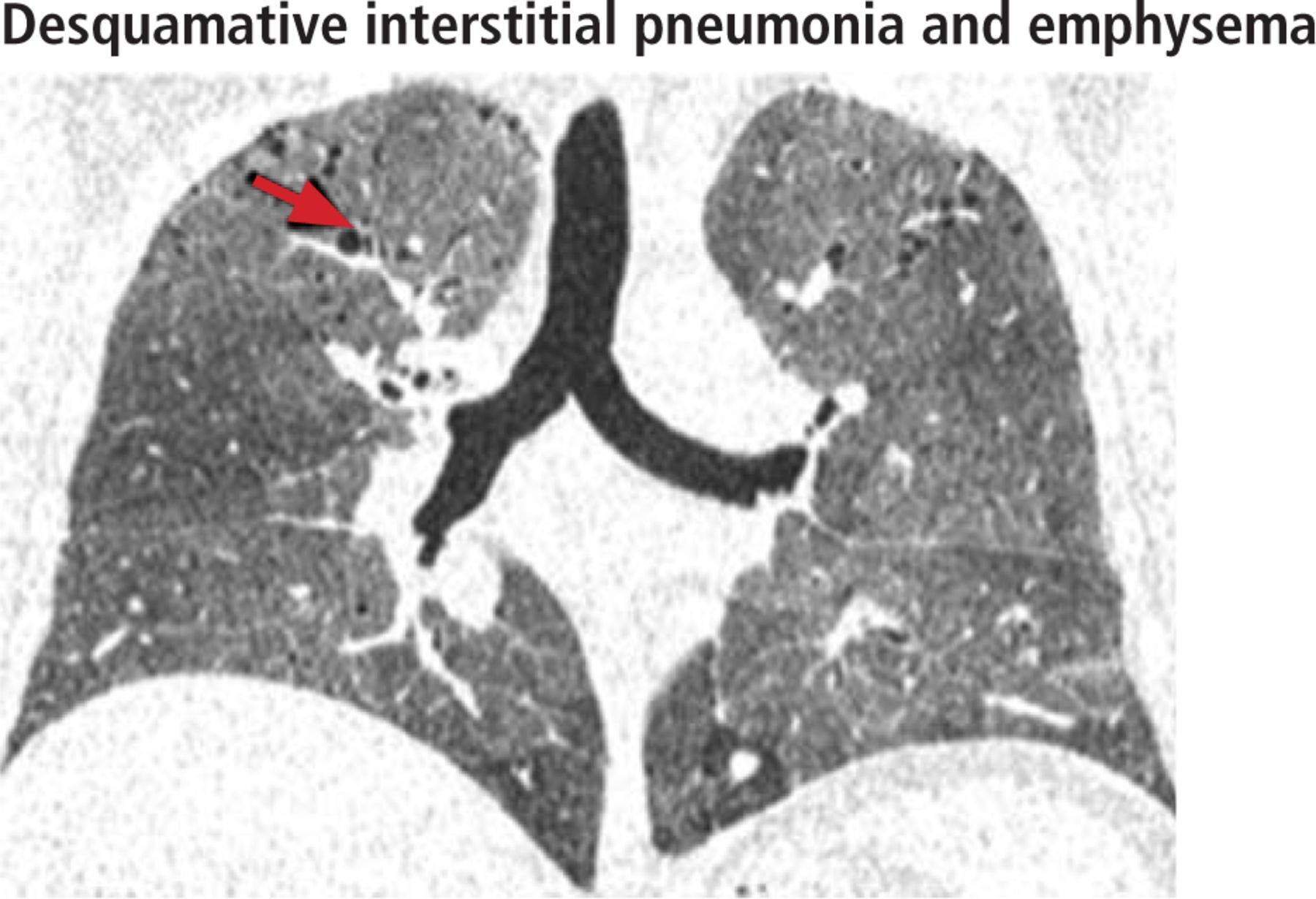
- FIGURE 4
In a 38-year-old man with a 20-pack-year history of smoking, coronal image reformatting shows features of desquamative interstitial pneumonia and emphysema, ie, diffuse distribution of ground-glass opacities with cystic airspaces representing emphysema (red arrow).
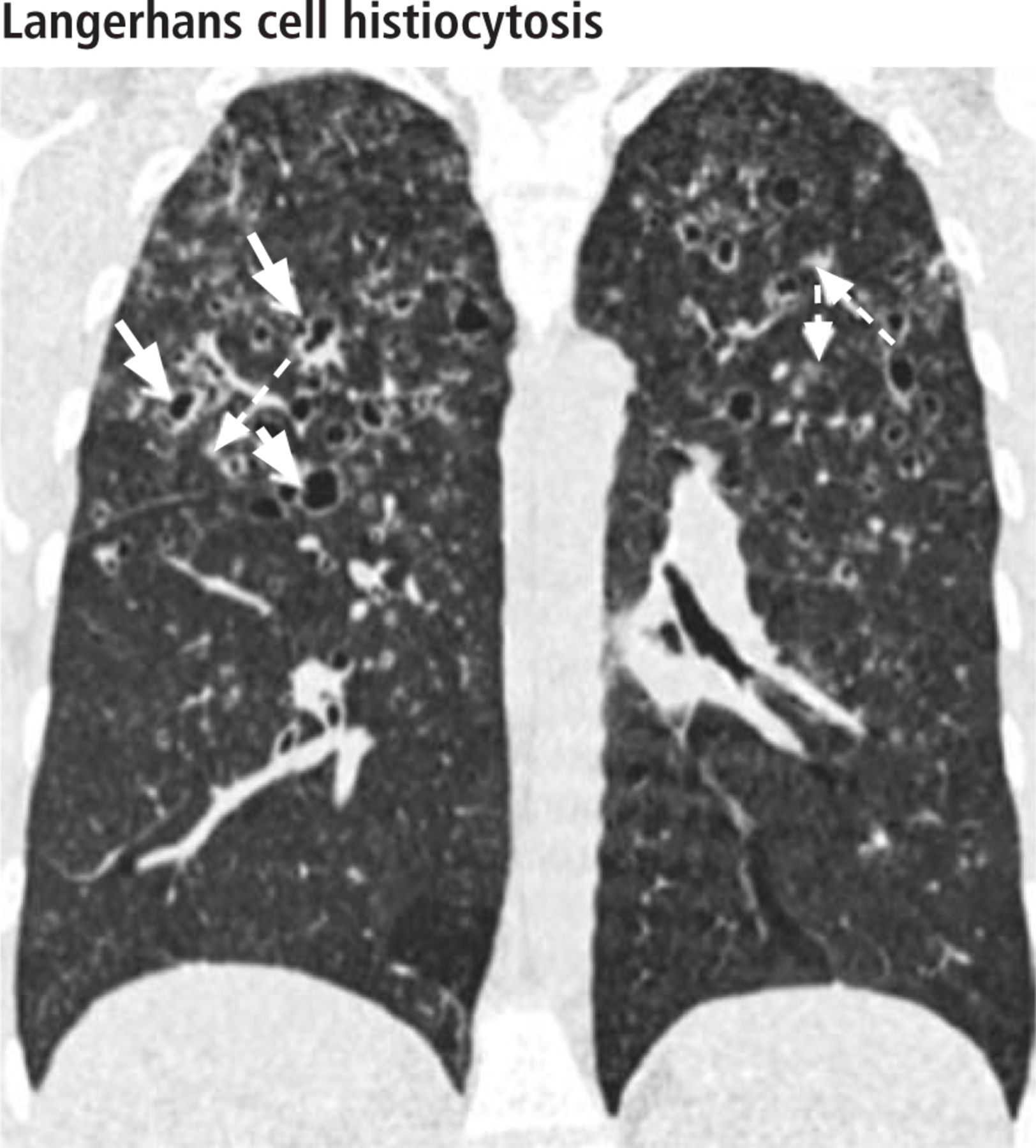
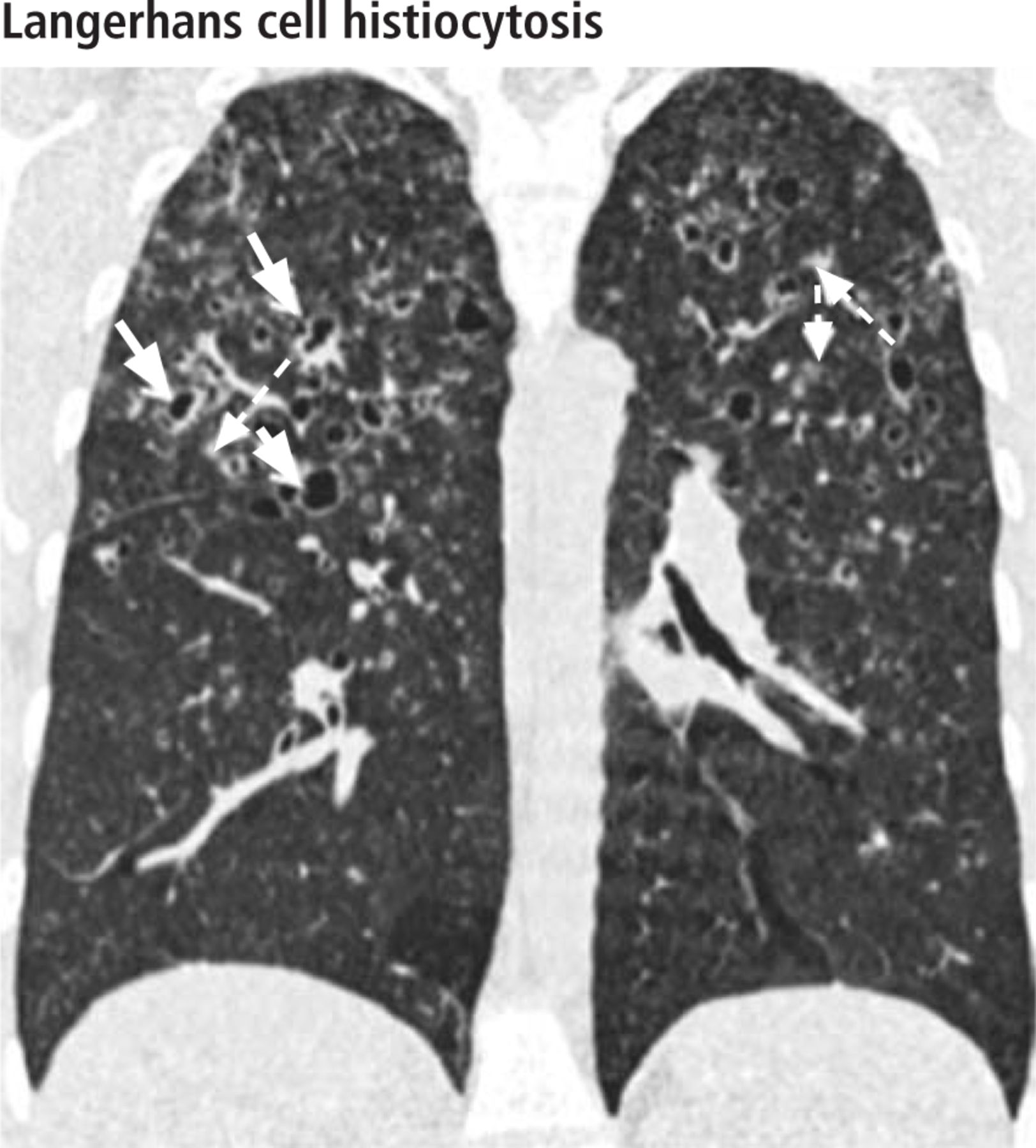
- FIGURE 5
In a 46-year-old woman with a 26-pack-year history of smoking, a coronal reformatted image shows various-sized cysts (solid white arrows) and nodules (dashed white arrow) in the upper and midlung zones—a characteristic imaging pattern of smoking-related pulmonary Langerhans cell histiocytosis, which was later confirmed with biopsy in this patient.
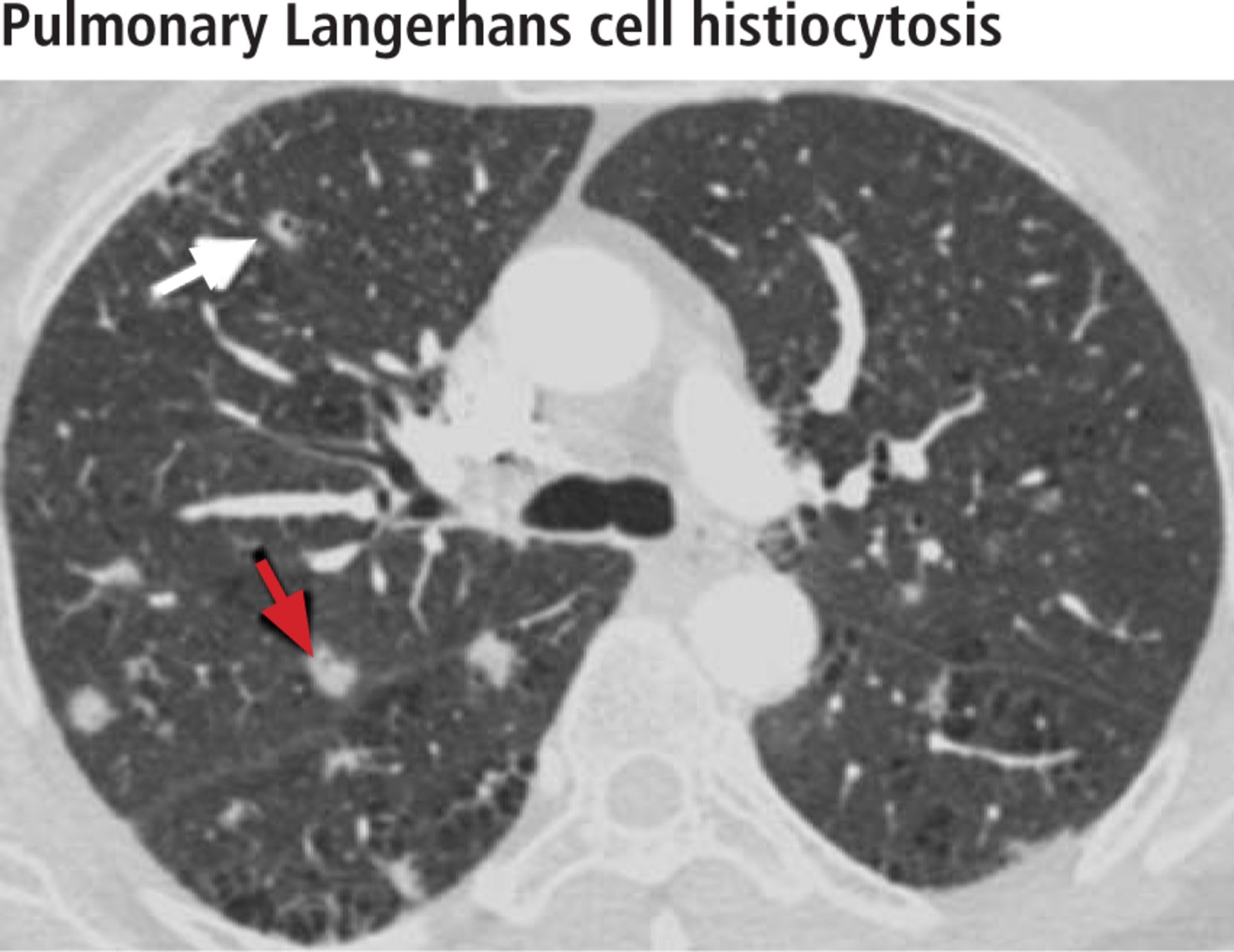
- FIGURE 6
Early-stage pulmonary Langer-hans cell histiocytosis (nodule-predominant) mimics metastasis in a 56-year-old woman with a 19-pack-year history of smoking. High-resolution CT obtained through the midlungs shows few irregularly marginated nodules (red arrow), one of which is cavitary (white arrow). There is a background of centrilobular emphysema. No cysts are seen. Histologic study confirmed the diagnosis.
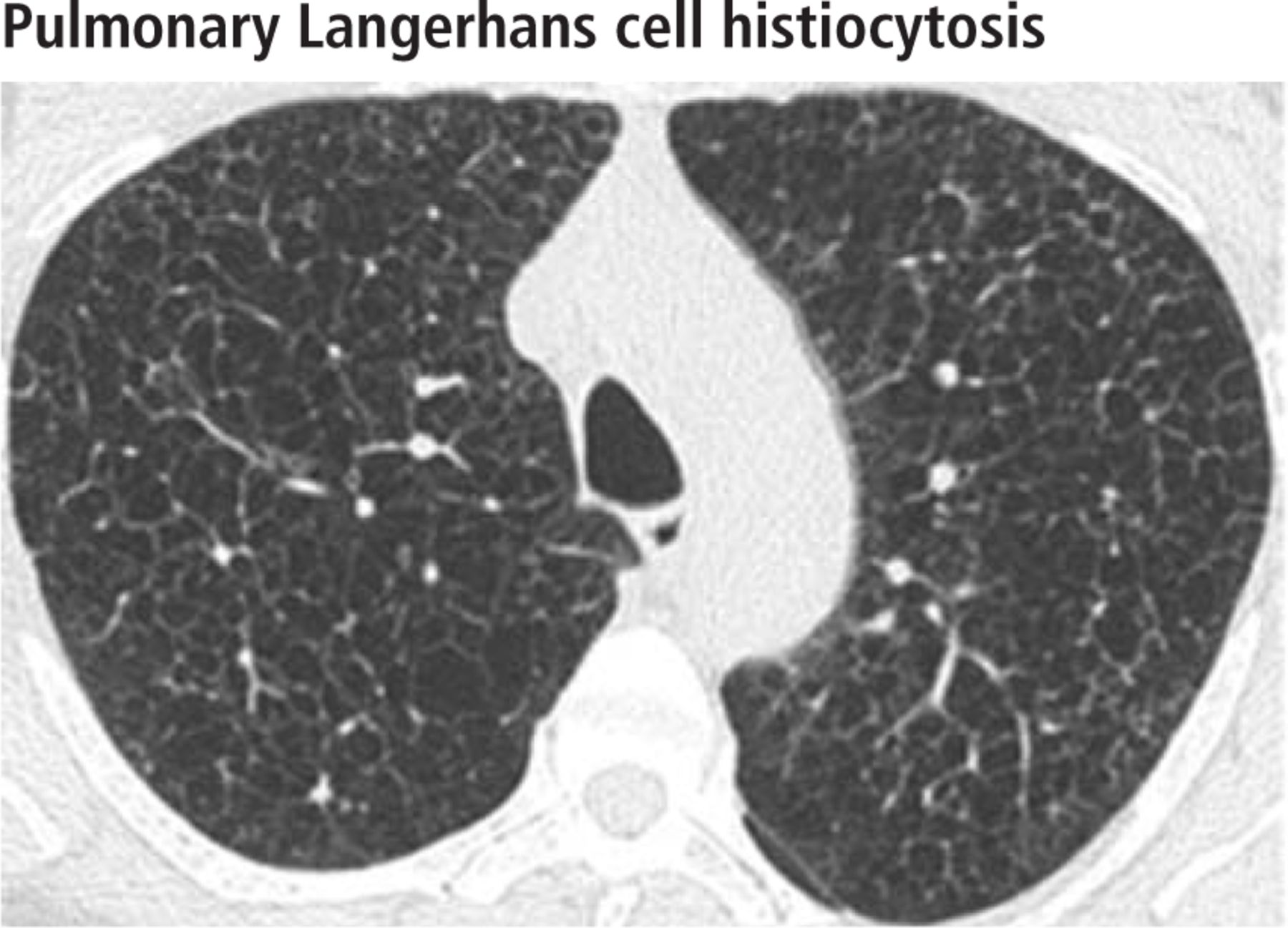
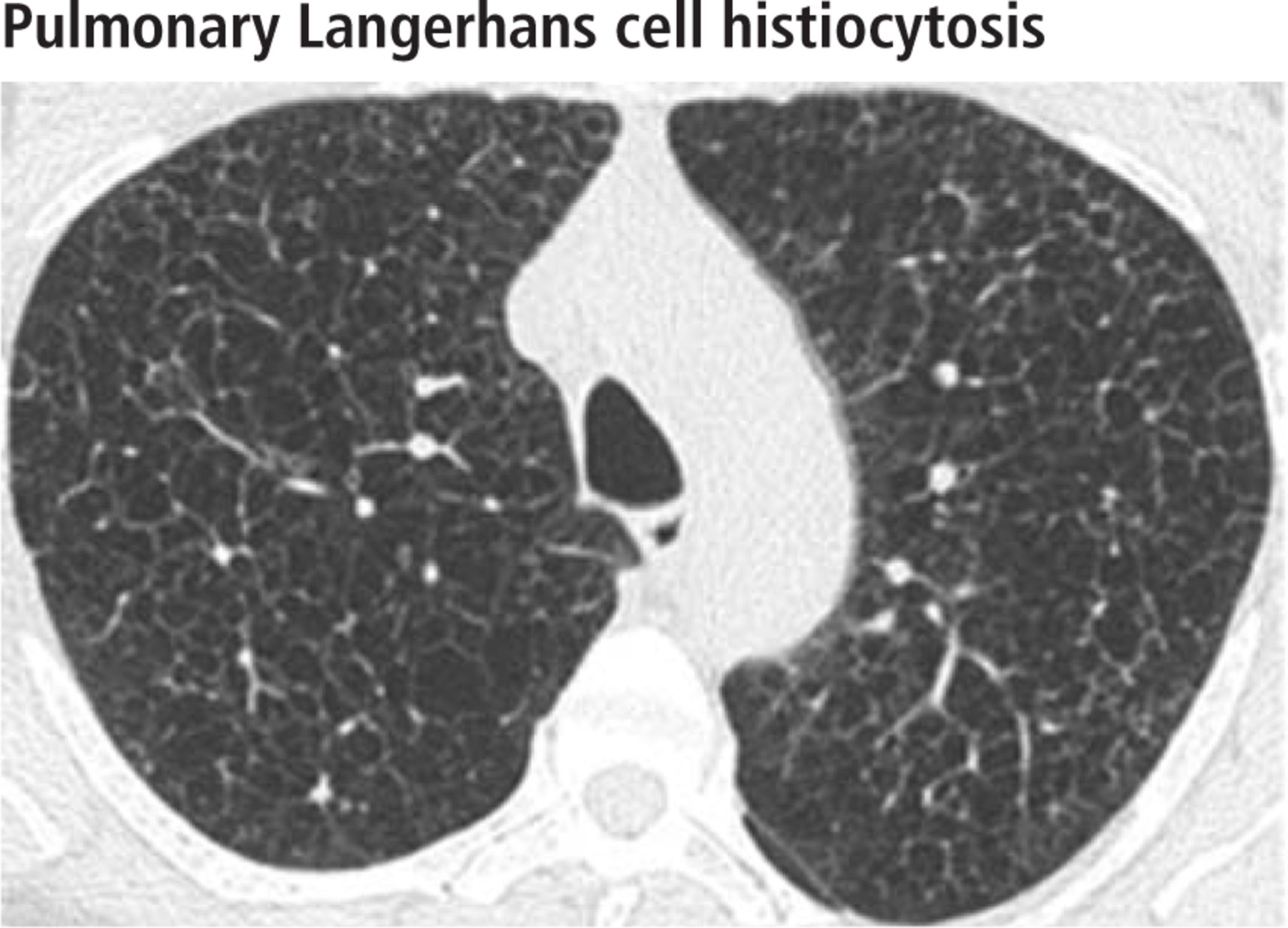
- FIGURE 7
In a 49-year-old male smoker with biopsy-confirmed pulmonary Langerhans cell histiocytosis, high-resolution CT obtained through the upper lungs shows numerous well-circumscribed, thin-walled cysts with absence of nodules. This appearance is typical of advanced (“burned out”) pulmonary Langerhans cell histiocytosis and is virtually indistinguishable from emphysema on high-resolution CT.
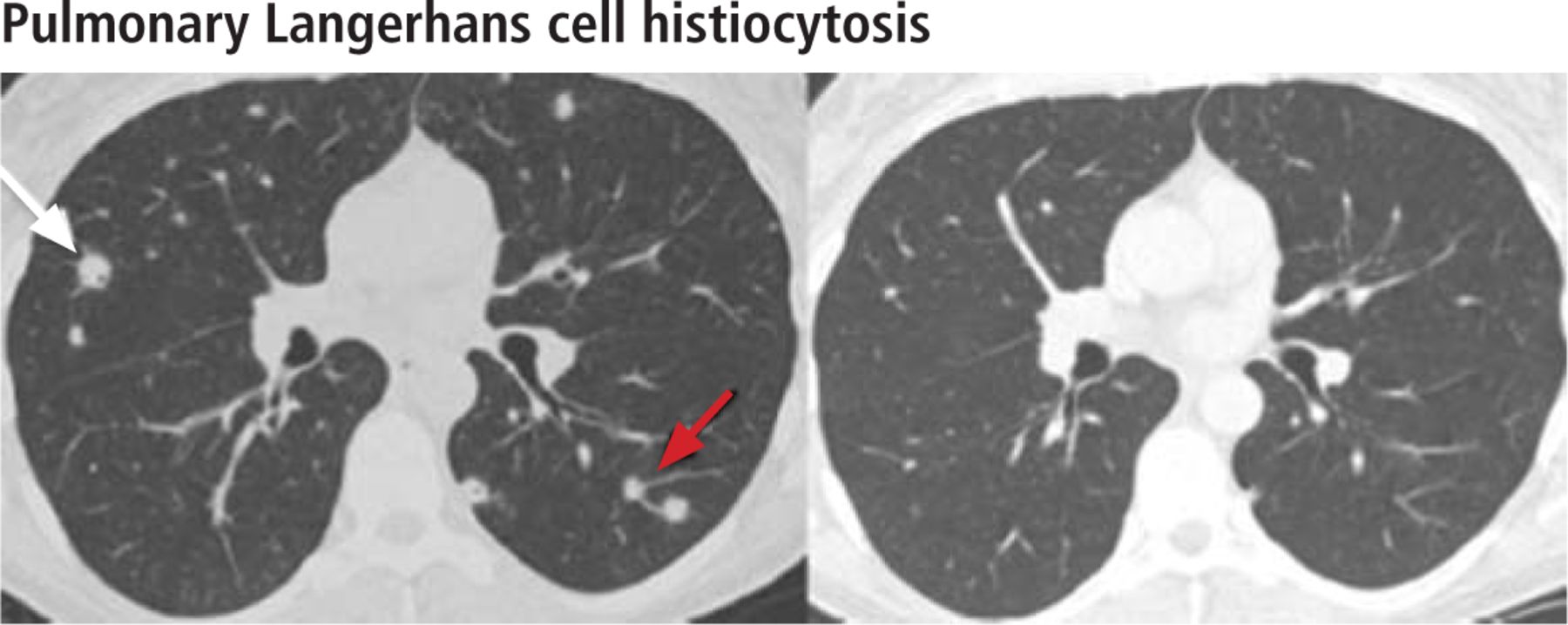
- FIGURE 8
In a 41-year-old woman with a 22-pack-year history of smoking and pulmonary Langerhans cell histiocytosis, high-resolution CT through the midlungs at the time of initial diagnosis (left) shows a few solid (red arrow) and cavitary (white arrow) nodules. The lung bases were spared. No cysts were seen. High-resolution CT 2 years after smoking cessation and oral corticosteroid therapy (right) shows near-complete resolution of the nodules.
- FIGURE 9
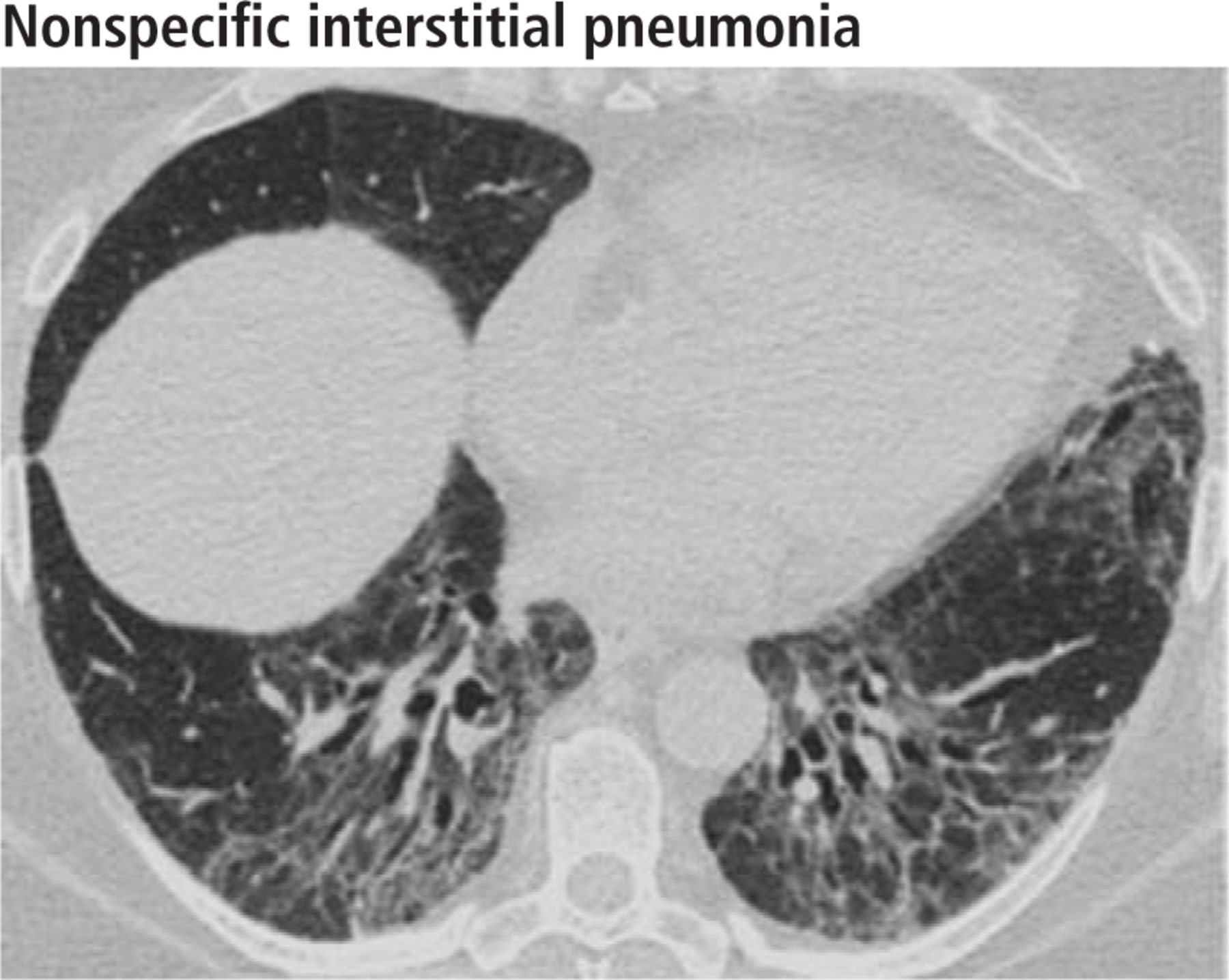
In a 53-year-old woman with mild dyspnea, high-resolution CT through the lower lungs shows bilateral symmetric peripheral distribution of ground-glass opacities, a feature of nonspecific interstitial pneumonia.
- FIGURE 10
High-resolution CT through the lower lungs in a 60-year-old woman with nonspecific interstitial pneumonia shows bilateral symmetric peribronchovascular distribution of ground-glass and reticular opacities with traction bronchiectasis.
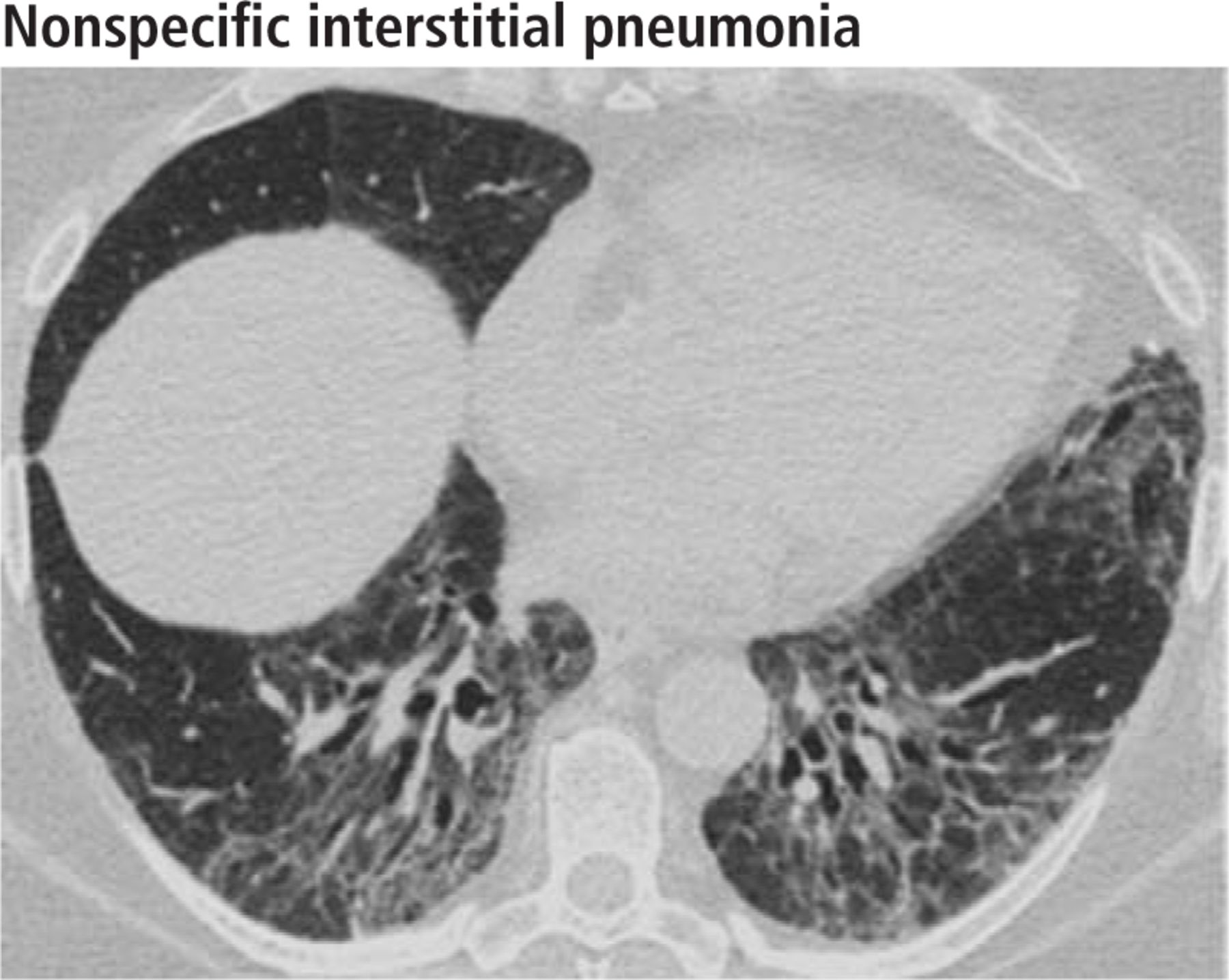
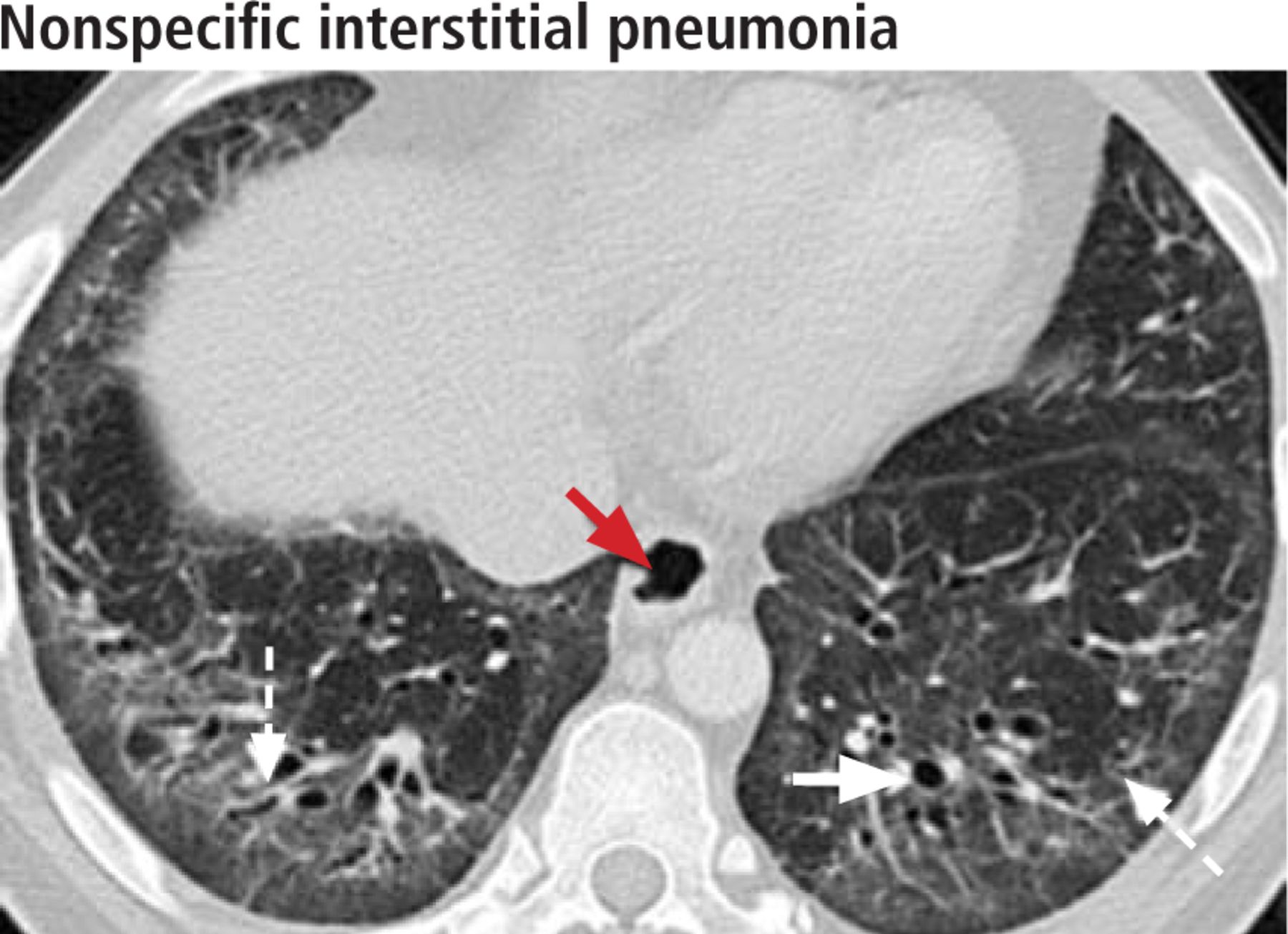
- FIGURE 11
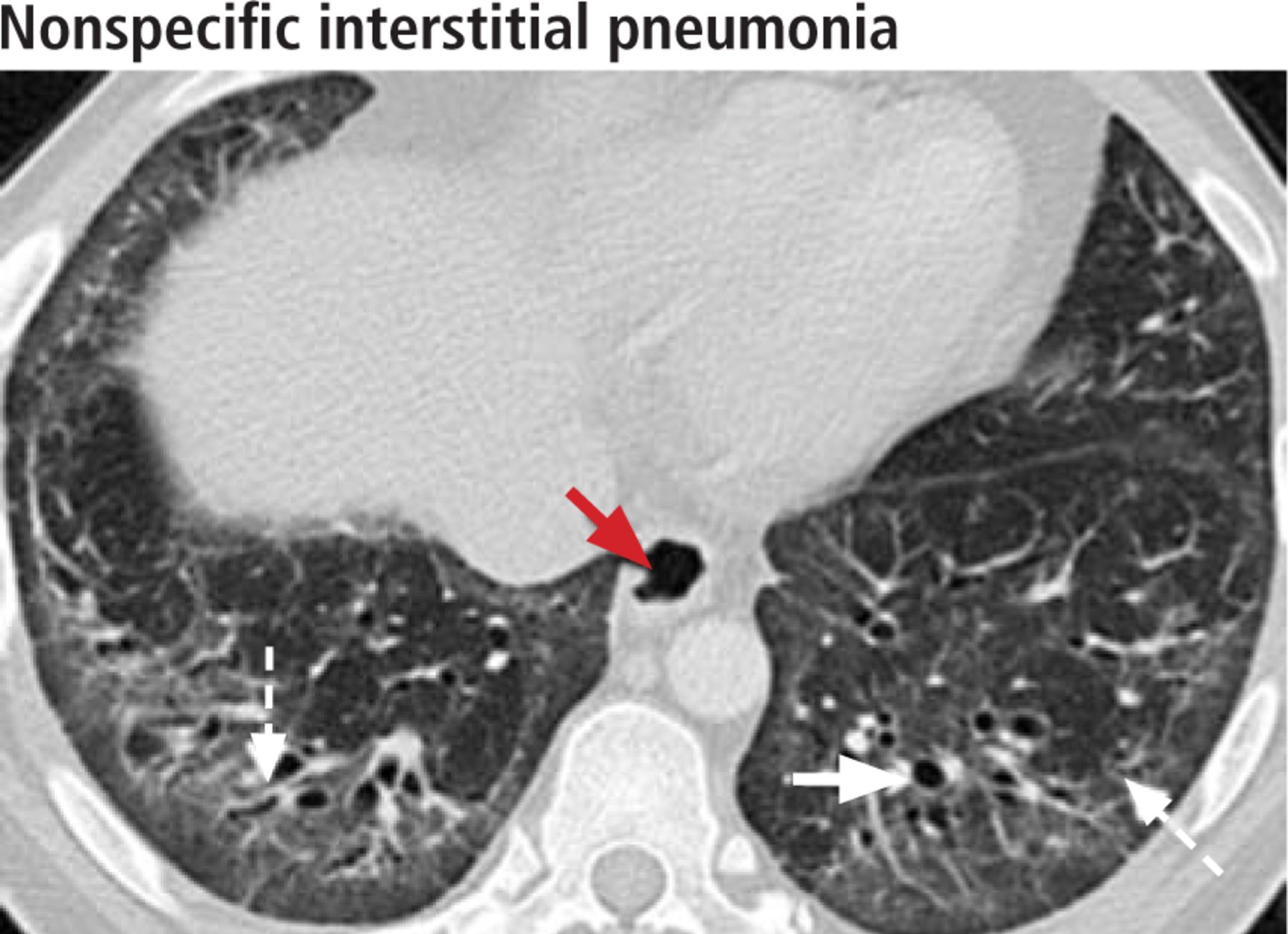
High-resolution CT through the lower lungs in a 45-year-old woman with scleroderma and nonspecific interstitial pneumonia shows bilateral symmetric peripheral ground-glass attenuation with reticular opacities, traction bronchiectasis (white solid arrow), traction bronchiolectasis (white dashed arrows), and subpleural sparing. A dilated esophagus (red arrow) correlates with the history of scleroderma.
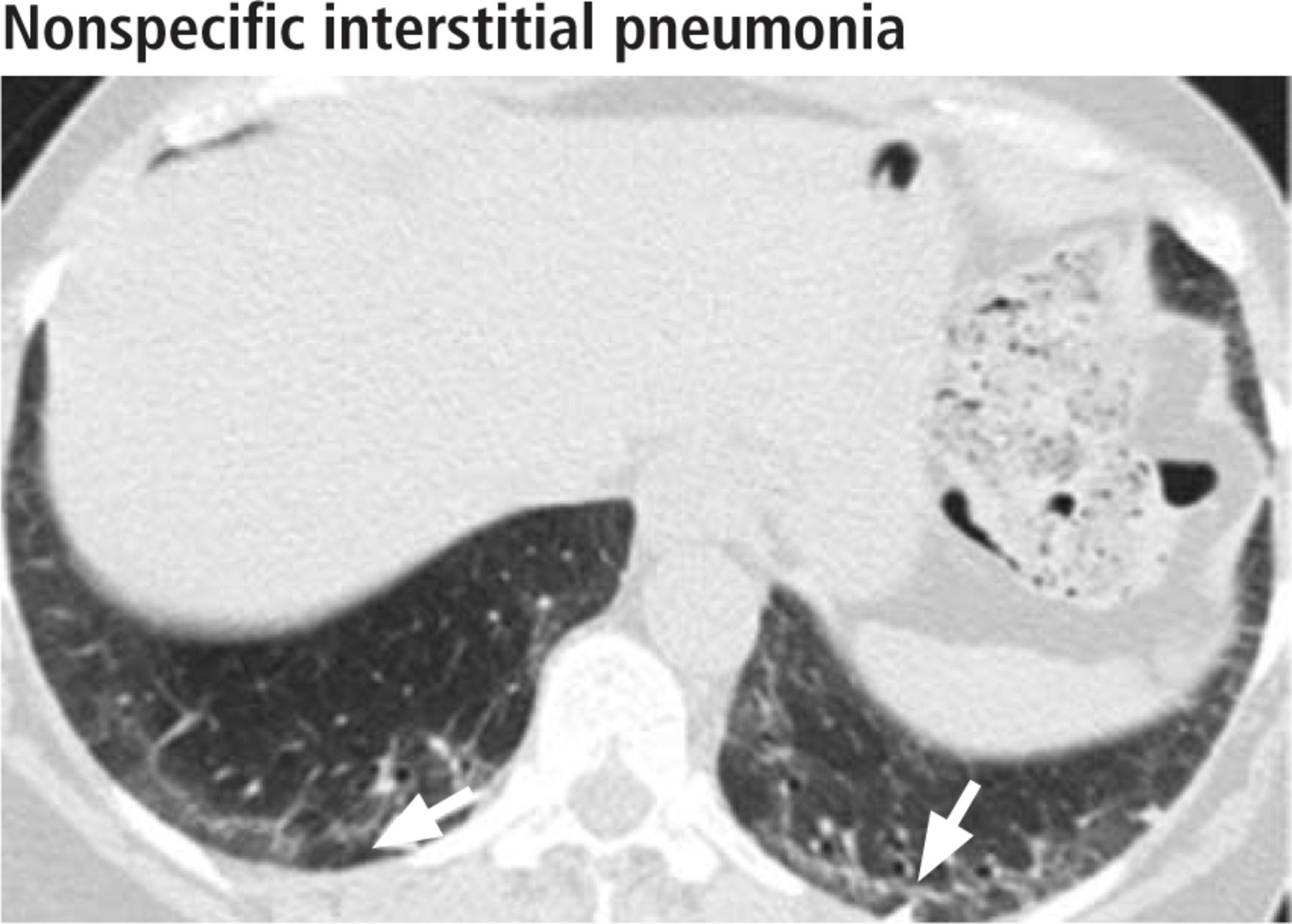
- FIGURE 12
In a 52-year-old woman with mild dyspnea and fatigue, high-resolution CT through the lower lungs shows bilateral symmetric peripheral ground-glass opacities with sparing of the immediate subpleural lung (white arrows), the most specific sign of nonspecific interstitial pneumonia.
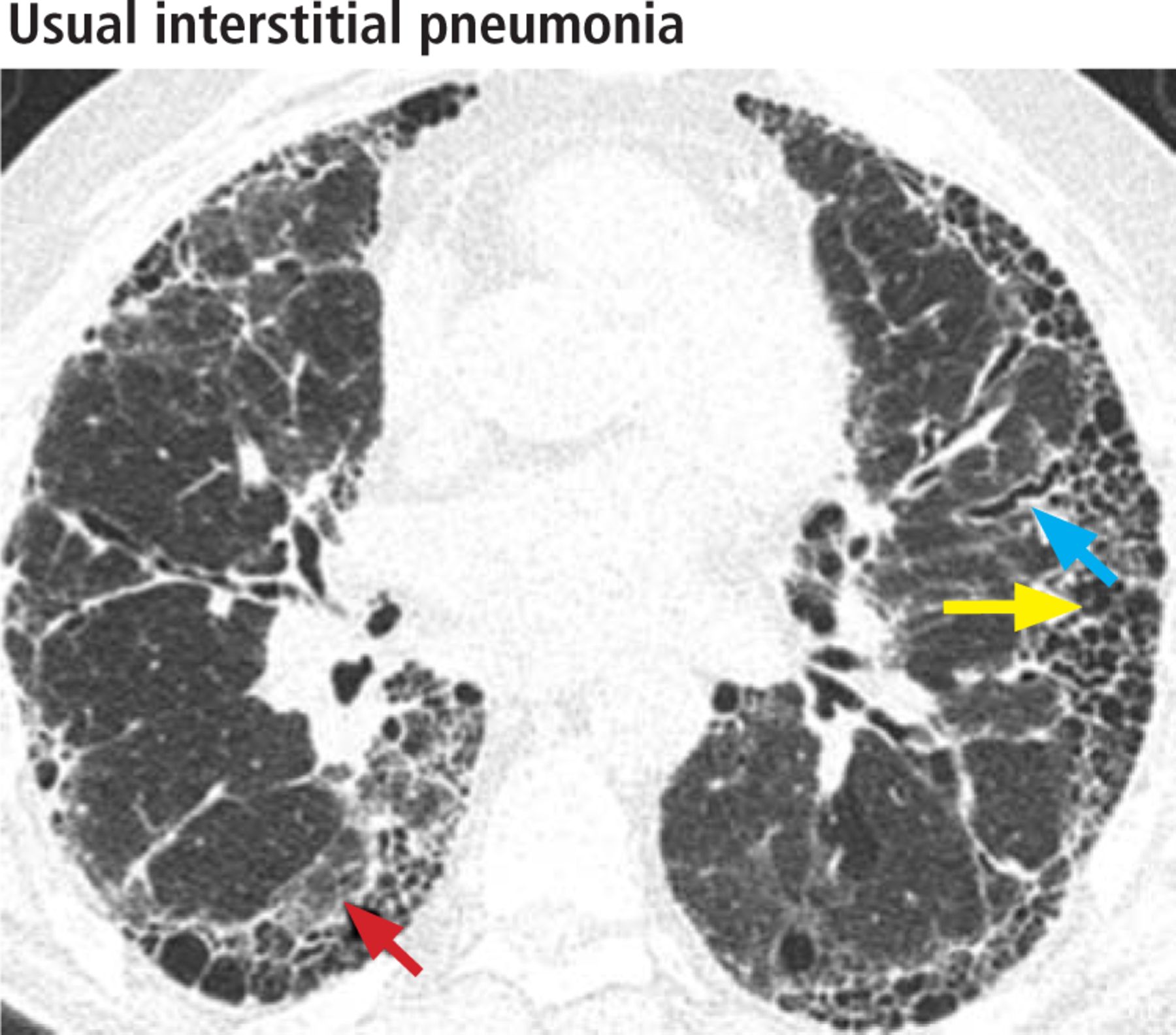
- FIGURE 13
In a 68-year-old man, high-resolution CT through the lower lungs shows features of usual interstitial pneumonia: bilateral subpleural reticular opacities, traction bronchiectasis (blue arrow), ground-glass opacities (red arrow), and honeycombing, seen as rows of clustered subpleural cystic air spaces (yellow arrow).
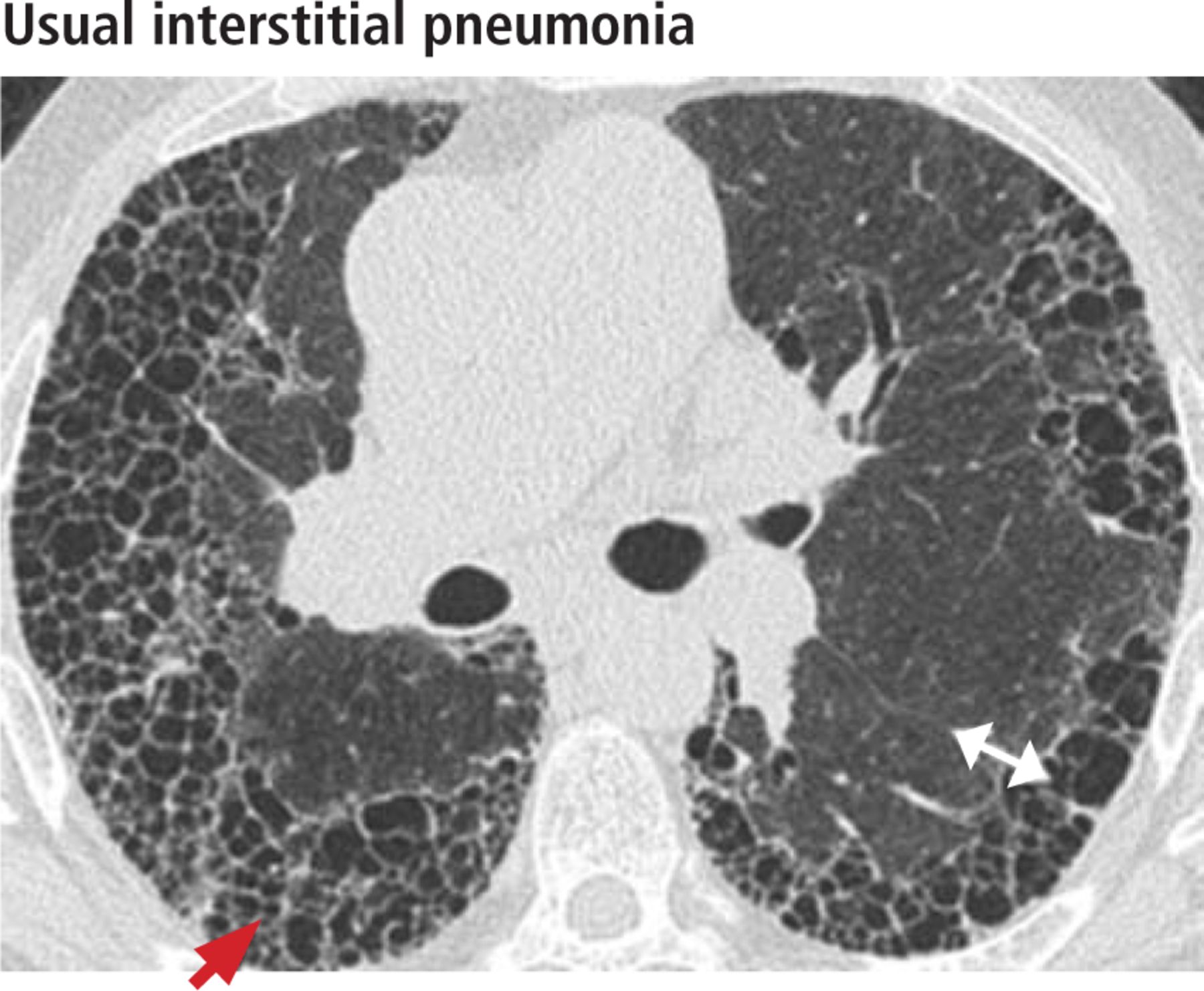
- FIGURE 14
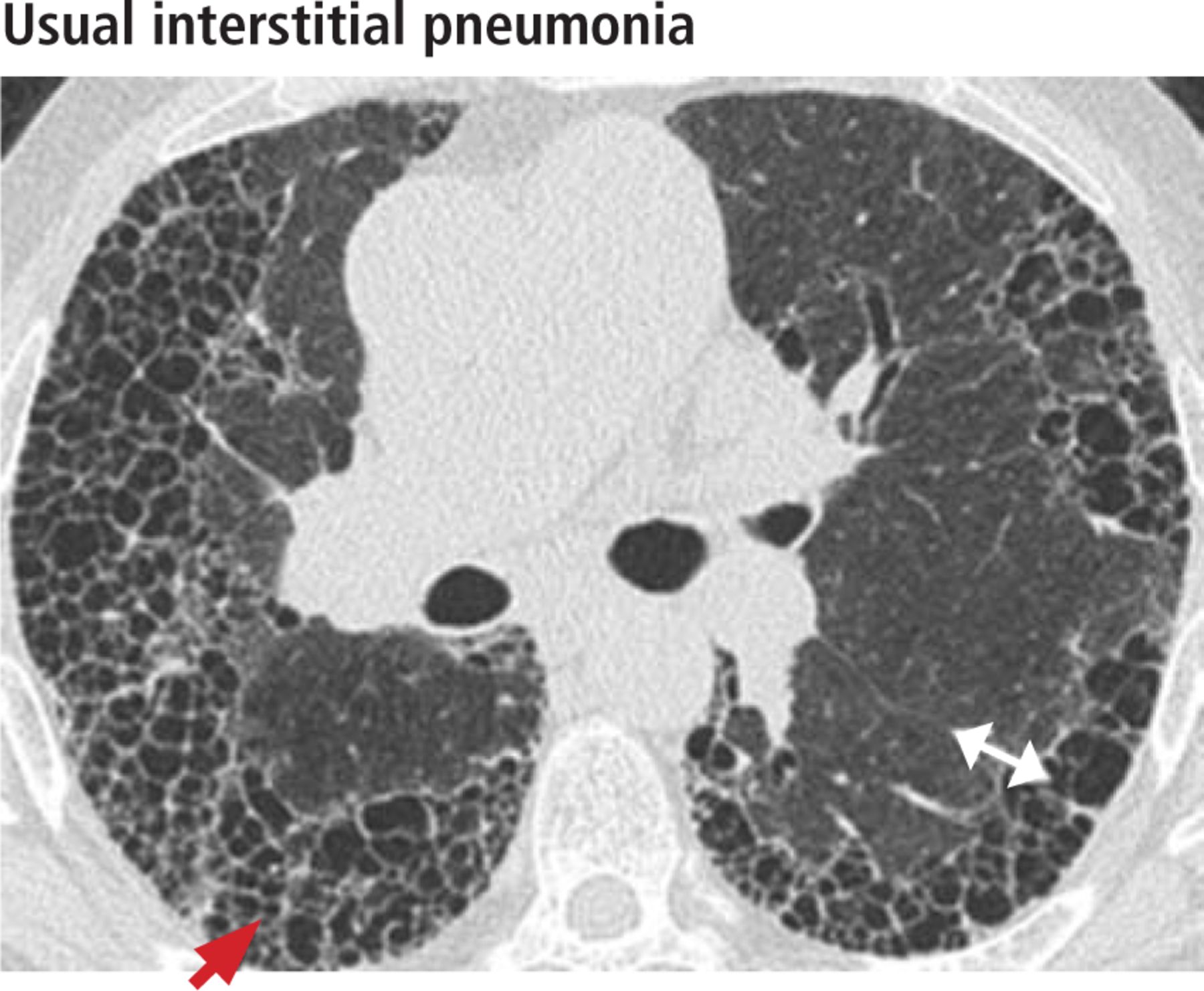
In a 67-year-old man with usual interstitial pneumonia, high-resolution CT through the lower lungs shows basal-predominant subpleural honeycombing (red arrow). Morphologic heterogeneity is seen with areas of fibrosis immediately adjacent to normal lung (white double arrow).







Tables
Respiratory bronchiolitis Respiratory bronchiolitis interstitial lung disease Desquamative interstitial pneumonia Pulmonary Langerhans cell histiocytosis Zonal distribution Upper lobe Upper lobe Lower lobe (60%)
Diffuse (20%)
Patchy (20%)Upper lobe (spares the costophrenic angles) Clinical findings Absent Cough and dyspnea Cough and dyspnea Cough and dyspnea, constitutional symptoms (1/3 of patients) and pneumothorax (15%) Findings on high-resolution computed tomography Poorly defined centrilobular ground-glass nodules Poorly defined centrilobular ground-glass nodules
Patchy ground-glass opacities
Bronchial wall thickening
Reticulation occasionally (no traction bronchiectasis or honeycombing)Ground-glass opacity (widespread, bilateral and symmetrical in 86%)
Reticular opacities (59%)
Traction bronchiectasis
Honeycombing is uncommon (< 1/3 of patients)Cysts: bizarrely shaped and nonuniform in size
Nodules: irregular or cavitary, centrilobular and peribronchial in locationAssociated features Centrilobular emphysema
Air-trappingCentrilobular emphysema
Peripheral cystic spaces (dilated bronchioles and alveolar ducts)Characteristic image Figure 1 Figure 2 Figures 3 and 4 Figures 5–8 Typical clinical course Usually asymptomatic; may progress to respiratory bronchiolitis-interstitial lung disease if smoking continues Cough and progressive dyspnea on exertion Cough and progressive dyspnea; can progress despite smoking cessation Fever, weight loss, nonproductive cough, dyspnea, chest pain; spontaneous pneumothorax also seen Role of lung biopsy None None Surgical lung biopsy may be indicated if diagnosis is uncertain Surgical lung biopsy may be indicated if diagnosis is uncertain Nonspecific interstitial pneumonia Usual interstitial pneumonia, idiopathic pulmonary fibrosis Craniocaudal distribution Basilar, symmetric Apicobasal gradient Axial distribution Subpleural and peribronchovascular Subpleural Morphology Ground-glass opacities (80%)
Subpleural sparing (20%–50%)—most specific
Reticulation (fine or coarse)
Traction bronchiectasis
Consolidation
Honeycombing (uncommon, 1%–5%)Reticulation (coarse)
Honeycombing (up to 70%)
Traction bronchiectasis
Ground-glass opacities (in regions of fibrosis, less extensive than the reticulation)
Architectural distortionCharacteristic image Figures 9–12 Figures 13 and 14 Typical clinical course Progressive dyspnea, cough, and hypoxemia; often have extrapulmonary manifestations (eg, joint pain, rash, Raynaud phenomenon); may respond to immunosuppressive therapy, especially if ground-glass opacities are present Progressive dyspnea, cough, and hypoxemia; newly approved antifibrotic agents may slow progression of disease Role of lung biopsy Surgical lung biopsy may be indicated if diagnosis is uncertain Surgical lung biopsy may be indicated if diagnosis is uncertain Usual interstitial pneumonia (including idiopathic pulmonary fibrosis) Basal predominance of honeycombing Absence of relative subpleural sparing Absence of centrilobular nodules Nonspecific interstitial pneumonia Relative subpleural sparing Absence of lobular areas with decreased attenuation Lack of honeycombing Information from Silva CI, Müller NL, Lynch DA, et al. Chronic hypersensitivity pneumonitis: differentiation from idiopathic pulmonary fibrosis and nonspecific interstitial pneumonia by using thin-section CT. Radiology 2008; 246:288–297.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}