


Article Figures & Data
Figures
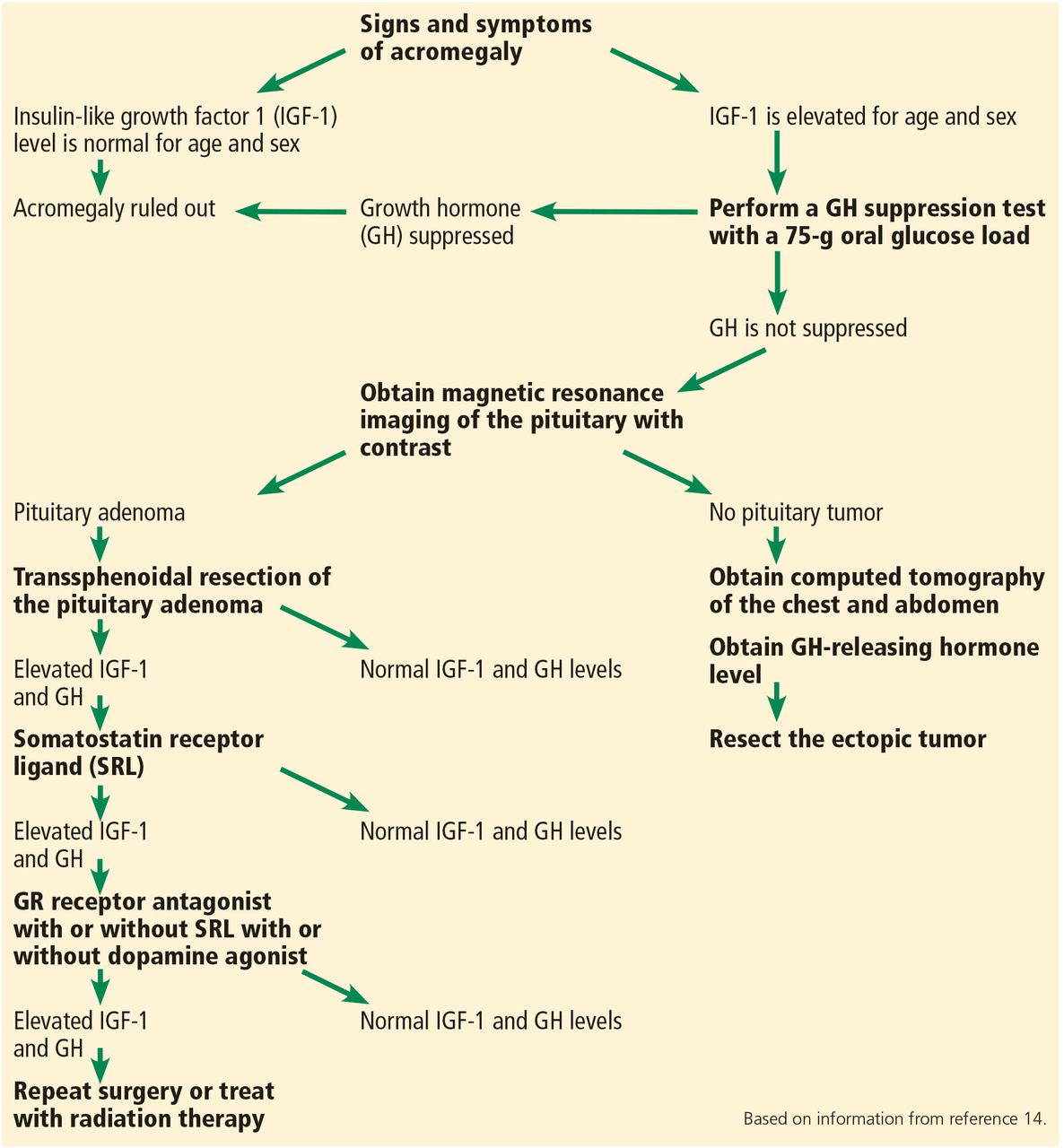
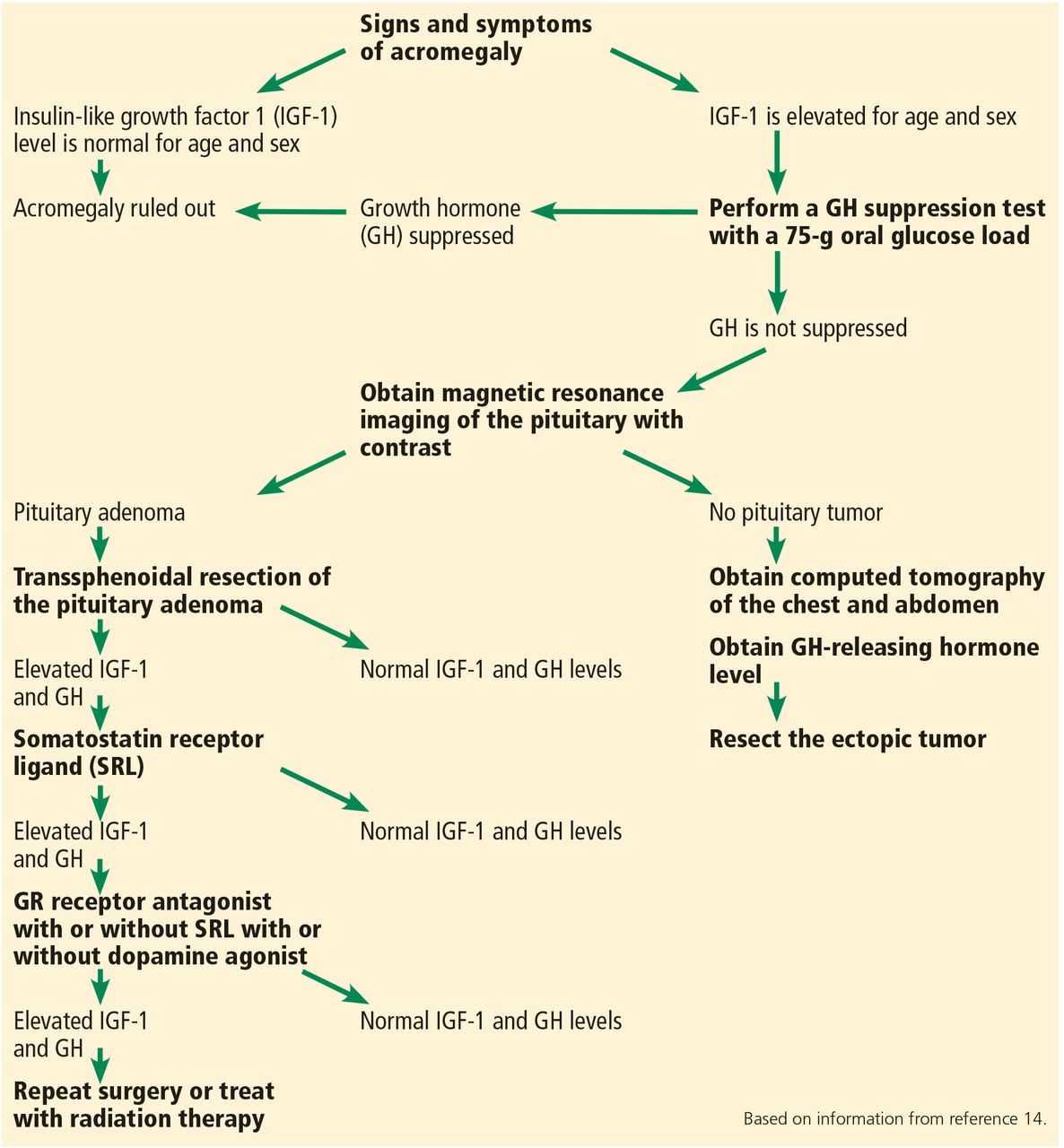
- Figure 1
Diagnostic and treatment algorithm for acromegaly.
Tables
Neurologic symptoms due to pituitary tumor’s mass effect
Visual field deficits, headache, cranial nerve palsiesMusculoskeletal system
Increased thickness of soft tissue of hands and feet (enlarging size of gloves and shoes, rings becoming too small), prognathism, jaw malocclusion, arthropathy and osteoarthritis (affects up to 75% of patients and is a leading cause of morbidity and disability in patients with acromegaly), carpal tunnel syndrome (present in about 64% of patients on presentation), proximal myopathy, hypertrophy of frontal bones (frontal bossing)Integumentary system
Oily texture, hyperhidrosis, skin tags, deep skin creasesCardiovascular system
Biventricular hypertrophy, asymmetric septal hypertrophy, cardiomyopathy, congestive heart failure, diastolic heart failure, arrhythmias (up to 40% of patients develop conduction disorders), hypertensionRespiratory system
Obstructive sleep apneaGastrointestinal system
Colon polyps, colon cancer, macroglossia, hepatomegalyEndocrine and metabolic system
Irregular menses, galactorrhea, decreased libido, erectile dysfunction, thyromegaly, diabetes mellitus, hypertriglyceridemia; in multiple endocrine neoplasia syndrome 1, acromegaly may be associated with primary hyperparathyroidism and pancreatic islet tumors.Based on information from references 2 and 3.
Medication Dose Normalization of IGF-1 Reduction of tumor size Comments Somatostatin receptor ligands (SRLs) Octreotide Starting dose 50 mg subcutaneously every 8 hours; can be increased every 2 weeks, usually up to 300 mg per day 30%–40% Arrested growth or reduced tumor size in about 50% Endocrine Society guidelines recommend use of either an SRL or pegvisomant as the initial adjuvant medical therapy. In patients with large tumors abutting the optic chiasm, an SRL is preferred as pegvisomant does not suppress tumor growth. An SRL is used as primary therapy in patients who cannot be cured by surgery, have extensive cavernous sinus invasion, have no chiasmal compression, or are poor surgical candidates. Octreotide long-acting release 10–40 mg intramuscularly every 4 weeks 30%–40% Lanreotide depot/autogel 60–120 mg deeply subcutaneous every 4 weeks 30%–40% Arrested growth or reduced tumor size in about 50% Pasireotide 40–60 mg intramuscularly every 28 days About 35% Arrested growth or reduced tumor size in about 50% A novel SRL with enhanced binding to more somatostatin receptors than the other SRLs. Associated with hyperglycemia in 57% of patients (see Table 3). Human GH receptor antagonist Pegvisomant 10–40 mg subcutaneously daily 63% Usually, no change, but tumor growth may occur in 3%–5% of patients Can be combined with an SRL. IGF-1 but not GH should be used as a marker of efficacy. Improves glycemic control, useful when comorbid diabetes mellitus is present. Very expensive. Dopamine agonist Cabergoline 1–4 mg by mouth weekly 20%–30% No change Can be an initial adjuvant therapy in patients with modest elevations of IGF-1 and GH, with or without concomitant hyperprolactinemia, and with mild signs and symptoms of acromegaly. Can be used in combination with an SRL or pegvisomant. Therapeutic response tends to decrease with time. GH = growth hormone; IGF-1= insulin-like growth factor 1
Based on information from references 14 and 15.
Medication Side effects Comments Octreotide
Octreotide long-acting release
Lanreotide depot/autogelCommon: abdominal cramps, flatulence and diarrhea; these symptoms usually subside with continued treatment; cholelithiasis and gallbladder sludge occur in approximately 25% of patients, usually without symptoms
Less common: local skin irritation, pain at the injection site, reversible hair loss
Glycemic control usually improves because these agents inhibit both insulin and glucagon as well as growth hormone secretion; rarely, glycemic control may worsenEndocrine Society guidelines recommend against routine abdominal ultrasound for monitoring for cholelithiasis in patients receiving somatostatin receptor ligands (SRLs) because symptomatic gallbladder disease is infrequent. Pasireotide In contrast to other SRLs, pasireotide causes hyperglycemia in 57% of patients
Other side effects are similar to those of the other SRLsPegvisomant Elevated liver aminotransferases in 9% of patients
Injection site reactions (local discomfort, reversible lipohypertrophy, or lipoatrophy) in 2.2% of patientsThe Endocrine Society guidelines suggest monitoring liver function tests monthly for the first 6 months, and then every 6 months in patients receiving pegvisomant.
Stop the drug if liver aminotransferase levels are elevated > 3 times the upper level of normal.Cabergoline Gastrointestinal upset, nasal congestion, fatigue, orthostasis, headache
Cardiac valve abnormalities have occurred in patients with Parkinson disease on high doses of cabergoline (> 2 mg/week)There is no consensus on frequency of cardiac valve monitoring in patients on cabergoline. If the dose exceeds 2 mg a week, consider obtaining a baseline echocardiogram and then serial echocardiograms; no specific recommendation currently exists. Based on information in reference 14.




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.