


A 42-year-old man presented with a lump on the side of his left hip, which had developed after he fell on his hip while playing basketball about 2 weeks earlier. He was able to continue playing and finished the game. After the game he noticed a lump, which rapidly increased in size. Significant bruising developed afterwards, and the area was mildly painful. The lump did not interfere with his daily activities, but it was annoying.
His medical, surgical, social, and family histories were unremarkable. Physical examination revealed a significant oval-shaped local swelling in the lateral aspect of his left hip with extensive surrounding ecchymosis (Figure 1). On palpation the swelling was mildly tender and fluctuant. Range of motion of the hip was normal and did not aggravate his pain.

Left lateral hip 2 weeks after a fall.
Ultrasonography to evaluate for fluid collection revealed a subcutaneous heterogeneous and hypoechoic area superficial to the greater trochanter, muscular structure, and the fascia (Figure 2). There was no enlargement of the greater trochanter bursa. Aspiration with an 18-gauge needle under ultrasonographic guidance provided no fluid. Based on the clinical presentation and imaging, the diagnosis of Morel-Lavallée lesion was made.
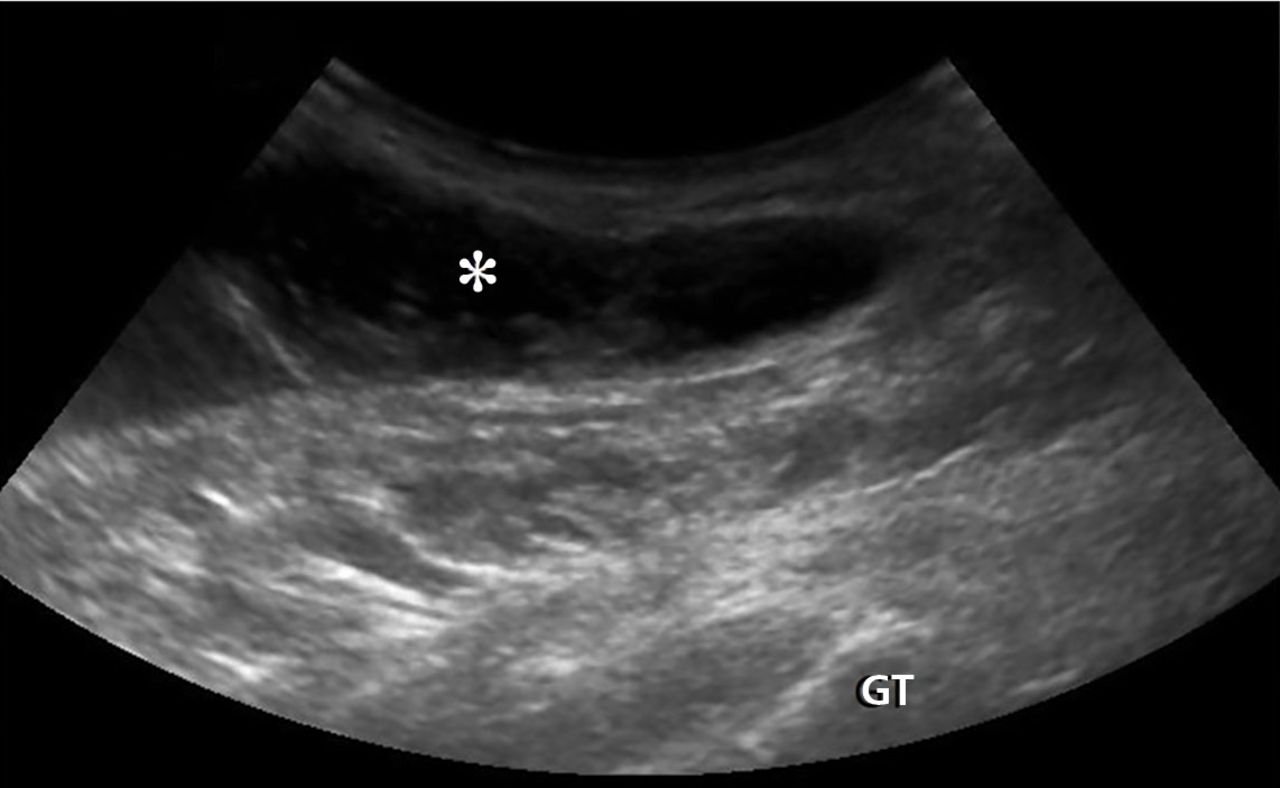
Ultrasonography with a curvilinear 2- to 5-MHz probe and a long-axis view revealed a superficial heterogeneous and hypoechoic area (asterisk) at the greater trochanter (GT).
THE DIFFERENTIAL DIAGNOSIS
Traumatic swelling of the lateral hip is an uncommon condition with few possible causes (Table 1).1–5 A comprehensive evaluation beginning with a history and physical examination is essential.
Differential diagnosis of a traumatic lateral hip lump
Morel-Lavallée lesion is an uncommon condition resulting from shearing trauma and collection of fluid in the space between deep fatty tissue and superficial fascia.6 It is usually the result of severe trauma, as in a motor vehicle accident, but it can also result from sports-related trauma, as in our patient.6–8 Lateral hip, gluteal, and sacral regions are the most common locations for Morel-Lavallée lesions and are often associated with an underlying fracture.6,9
Morel-Lavallée lesions usually develop hours or days after trauma, although they may develop weeks or even months later.2 Symptoms include bulging, pain, and loss of cutaneous sensation over the affected area. Although ultrasonography can be used, magnetic resonance imaging (MRI) is the gold standard for diagnosis and staging.6,10 If there is concern for fracture, plain radiography should be performed.
Mellado and Bencardino classified Morel-Lavallée lesions into 6 types based on their morphology, presence or absence of a capsule, signal behavior on MRI, and enhancement pattern.10 The exact rate of infection in patients with Morel-Lavallée lesions is unknown; however, the risk of infection seems to be highest after surgical intervention or aspiration.5,6
Another potential complication is fluid reaccumulation, which most often occurs with large lesions (> 50 mL) and lesions with a fibrous capsule or pseudocapsule.5 Large lesions can compromise adjacent neurovascular structures, particularly in the extremities.5 Potential consequences include dermal necrosis, compartment syndrome, and tissue necrosis.5
MANAGEMENT APPROACH
Aspiration of a fluid-filled mass is useful in both diagnosis and management of Morel-Lavallée lesions. Treatment includes watchful waiting; compression and pressure wraps; injection of a sclerosing agent (eg, doxycyline, alcohol); needle aspiration; percutaneous drainage with debridement, irrigation, and suction; and incision and evacuation.6
The approach to treatment depends on the stage of the lesion and whether an underlying fracture is present. Depending on the amount of blood and lymphatic products and the acuity of the collected fluid (hours to days post-trauma), aspiration with a large-bore needle (eg, 14 to 22 gauge) may or may not be successful.7 In general, traumatic serosanguinous fluid collections are less painful and resolve faster than well-formed coagulated hematomas.
Patients who have a large lesion, significant pain, or decreased range of motion should be referred to an orthopedic surgeon.
Our patient was managed conservatively, and his symptoms completely resolved in 2 months.
- Copyright © 2017 The Cleveland Clinic Foundation. All Rights Reserved.




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.