


Article Figures & Data
Figures
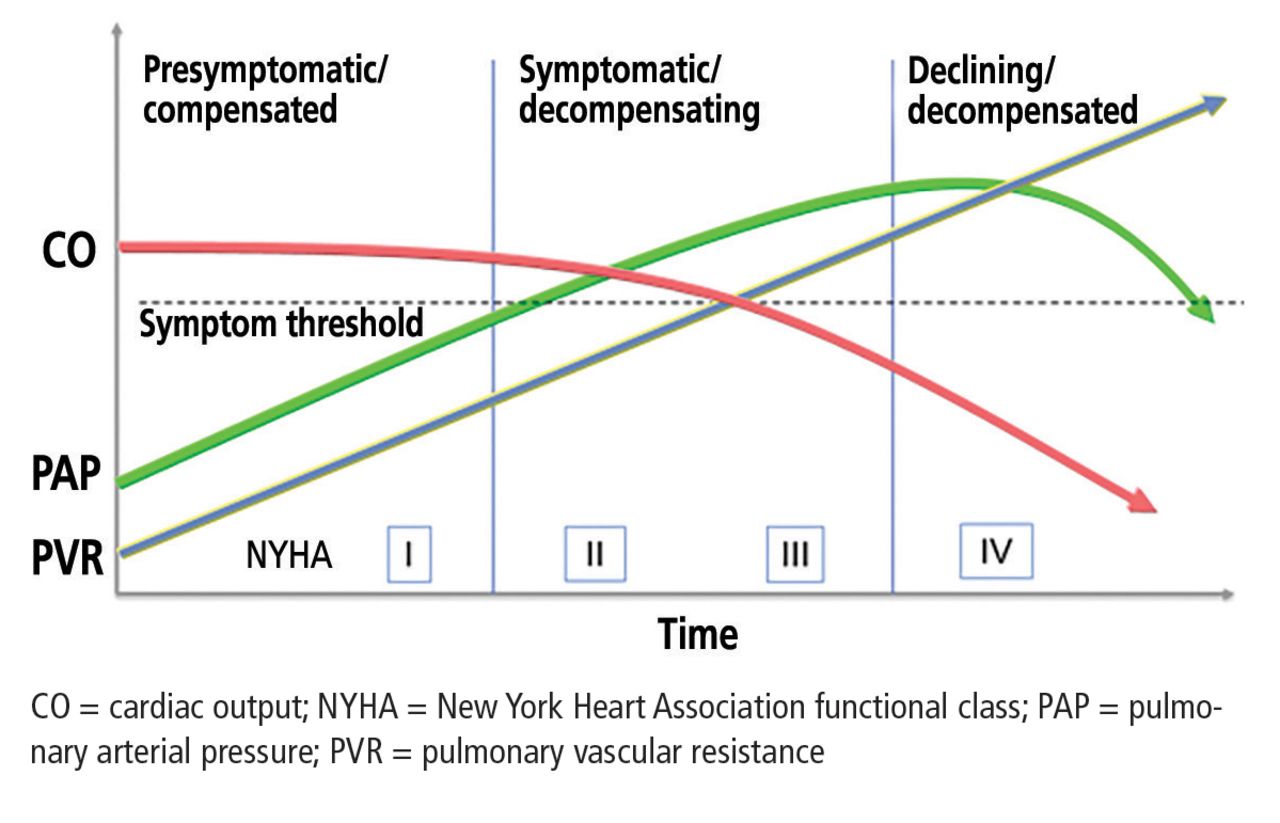
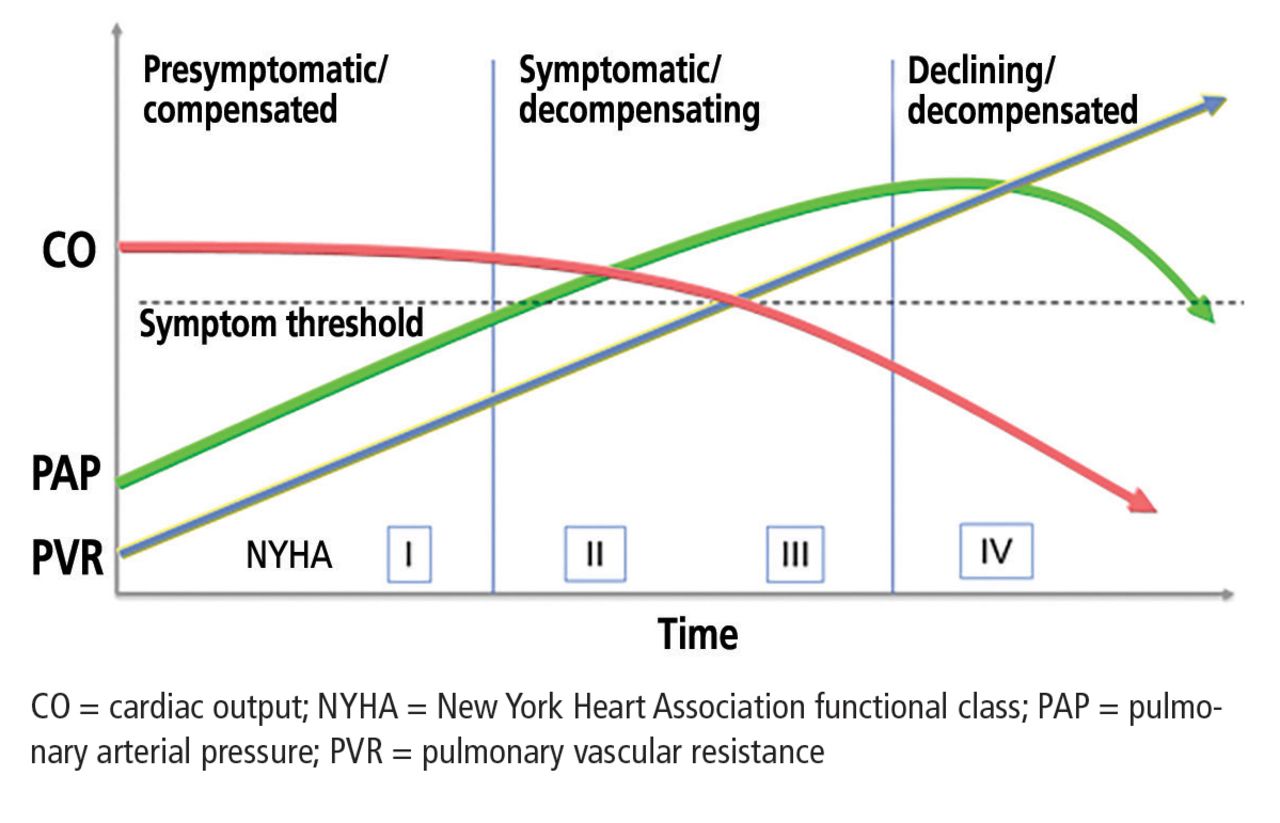
- Figure 2
Natural progression of disease in patients with pulmonary arterial hypertension.
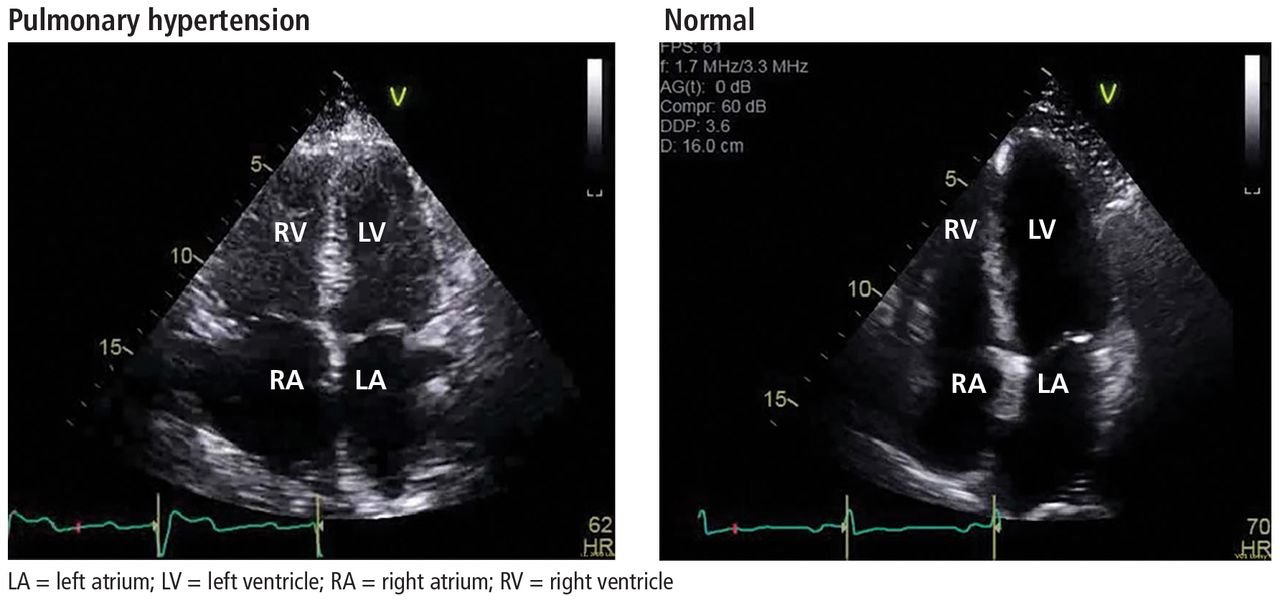
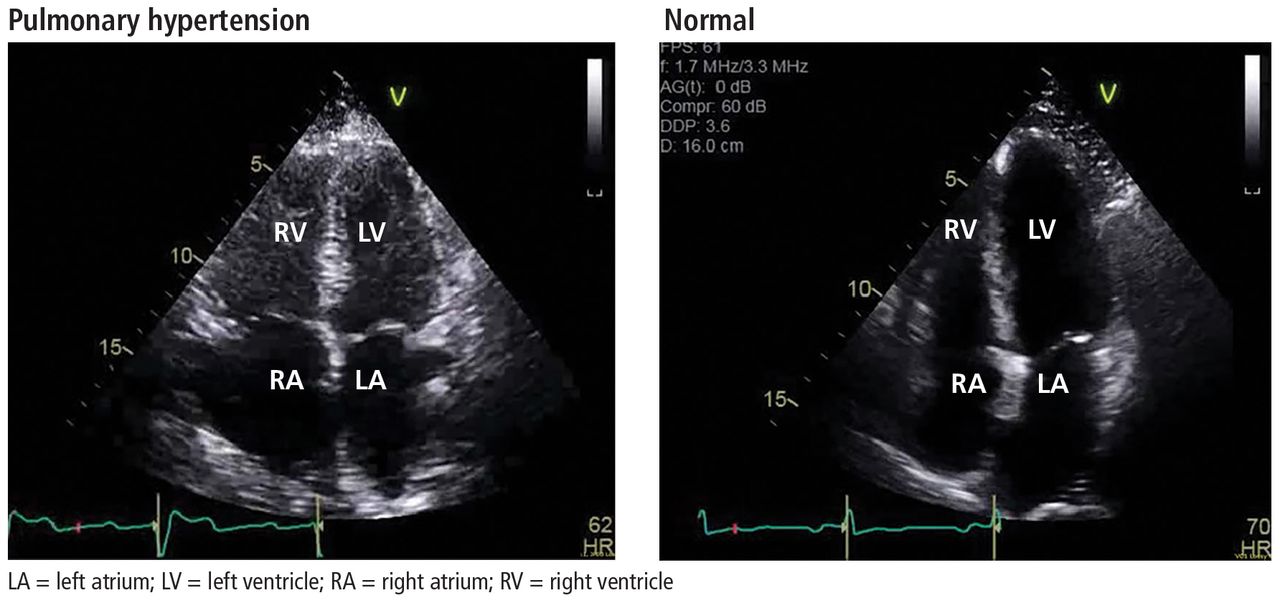
- Figure 3
Echocardiographic views of a patient with pulmonary hypertension (left) and a patient without (right). Note the increased right ventricular-left ventricular ratio and right atrial enlargement in the patient with pulmonary hypertension.
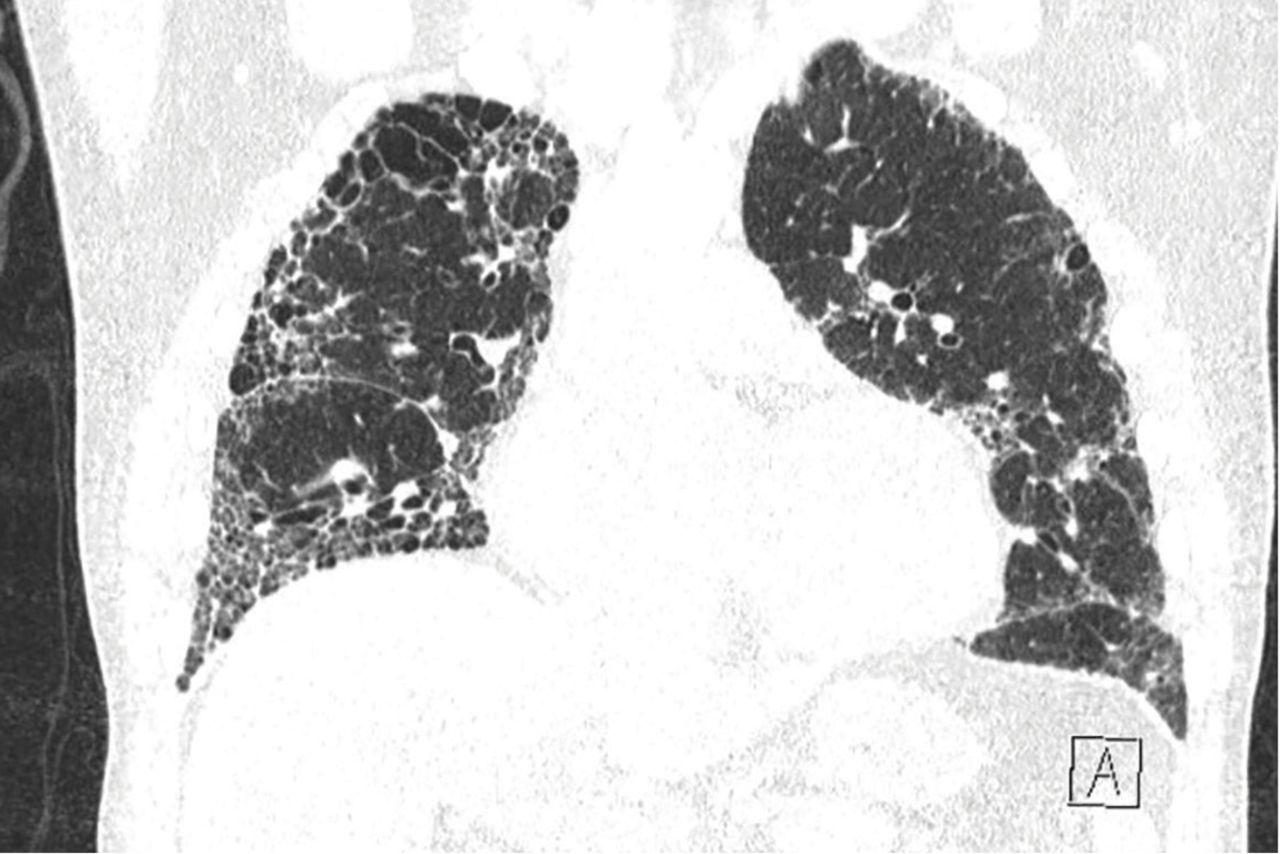
- Figure 4
A patient with combined pulmonary fibrosis and emphysema. In patients with findings consistent with underlying structural lung disease, further diagnostic testing for pulmonary arterial hypertension may not be warranted.


Tables
Group 1:
Pulmonary arterial hypertension
Idiopathic
Heritable
BMPR2 mutation
Other mutations
Drug- and toxin-induced
Associated with:
Connective tissue disease
Human immunodeficiency virus (HIV) infection
Portal hypertension
Congenital heart disease
Schistosomiasis
Pulmonary veno-occlusive disease or pulmonary capillary hemangiomatosis
Idiopathic
Heritable
EIF2AK4 mutation
Other mutations
Drug-, toxin-, and radiation-induced
Associated with:
Connective tissue disease
HIV infection
Persistent pulmonary hypertension of the newborn
Group 2:
Pulmonary hypertension due to left heart disease
Left ventricular systolic dysfunction
Left ventricular diastolic dysfunction
Valvular disease
Congenital or acquired left heart inflow or outflow tract obstruction and congenital cardiomyopathies
Congenital or acquired pulmonary vein stenosisGroup 3:
Pulmonary hypertension due to lung diseases, hypoxia, or both
Chronic obstructive pulmonary disease
Interstitial lung disease
Other pulmonary diseases with mixed restrictive and obstructive pattern
Sleep-disordered breathing
Alveolar hypoventilation disorders
Chronic exposure to high altitude
Developmental lung diseases
Group 4:
Chronic thromboembolic pulmonary hypertension and other pulmonary artery obstructions
Chronic thromboembolic pulmonary hypertension
Other pulmonary artery obstructions
Angiosarcoma
Other intravascular tumors
Arteritis
Congenital pulmonary artery stenosis
Parasites (hydatidosis)
Group 5:
Pulmonary hypertension with unclear or multifactorial mechanisms
Hematologic disorders: chronic hemolytic anemia, myeloproliferative disorders, splenectomy
Systemic disorders, sarcoidosis, pulmonary histiocytosis, lymphangioleiomyomatosis
Metabolic disorders: glycogen storage disease,
Gaucher disease, thyroid disorders
Others: pulmonary tumoral thrombotic microangiopathy, fibrosing mediastinitis, chronic renal failure (with or without dialysis), segmental pulmonary hypertensionReproduced with permission of the European Society of Cardiology and the European Respiratory Society. European Respiratory Journal Oct J 2015; 46(4):903–975. doi:10.1183/13993003.01032-2015
Right atrial dilation (area > 18 cm2) Elevated right atrial pressure based on inferior vena cava (IVC) assessment (IVC > 21 mm and collapses < 50% with inspiratory sniff) Ratio of right ventricle to left ventricle basal diameter > 1 Interventricular septal flattening or bowing towards the left ventricle A “mid-systolic notch” across the right ventricular outflow tract Reduced right ventricular outflow Doppler acceleration time < 105 msec Increased early diastolic pulmonary regurgitation velocity > 2.2 m/sec Pulmonary artery diameter > 25 mm Based on information in Galiè et al, reference 1.
Determinants of prognosis Estimated 1-year mortality Low-risk (< 5%) Intermediate risk (5%–10%) High risk (> 10%) Clinical signs of right heart failure Absent Absent Present Progression of symptoms No Slow Rapid Syncope No Occasional Repeated WHO functional class I, II III IV 6-minute walk distance > 440 m 165–440 m < 165 m Natriuretic peptide levels BNP < 50 ng/L
NT-proBNP < 300 ng/mLBNP 50–300 ng/L
NT-proBNP 300–1,400 ng/LBNP > 300 ng/L
NT-proBNP > 1,400 ng/LImaging
(echocardiography, CMRI)RA area < 18 cm2
No pericardial effusionRA area 18–26 cm2
No or minimal pericardial effusionRA area > 26 cm2
Pericardial effusionHemodynamics RA pressure < 8 mm Hg
CI ≥ 2.5 L/min/m2
SvO2 > 65%RA pressure 8–14 mm Hg
CI 2.0–2.4 L/min/m2
Svo2 60%–65%RA pressure > 14 mm Hg
CI < 2.0 L/min/m2
Svo2 < 60%CI = cardiac index; CMRI = cardiac magnetic resonance imaging; NT-proBNP = N-terminal pro-B-type natriuretic peptide; RA = right atrium; Svo2 = saturation of venous oxygen; WHO = World Health Organization. Reproduced with permission of the European Society of Cardiology and the European Respiratory Society. European Respiratory Journal Oct 2015; 46(4):903–975. doi:10.1183/13993003.01032-2015




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- ABSTRACT
- A PATIENT SUSPECTED OF HAVING PULMONARY HYPERTENSION
- DIAGNOSTIC EVALUATION OF SUSPECTED PULMONARY HYPERTENSION
- CLINICAL MANIFESTATIONS
- ECHOCARDIOGRAPHY IN SUSPECTED PULMONARY HYPERTENSION
- EVALUATING LEFT HEART DISEASE (WHO GROUP 2)
- EVALUATION OF LUNG DISEASE (WHO GROUP 3)
- EVALUATION OF THROMBOEMBOLIC DISEASE (WHO GROUP 4)
- RIGHT HEART CATHETERIZATION
- LOOKING FOR CAUSES OF ‘IDIOPATHIC’ PAH
- GROUP 5: MISCELLANEOUS FORMS OF PULMONARY HYPERTENSION
- PROGNOSTIC RISK STRATIFICATION IN THE PATIENTS WITH PAH
- REFERENCES
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- No citing articles found.