


It depends on the patient’s symptoms, underlying lung condition, immune status, and radiologic findings.
Because Aspergillus is ubiquitous, many patients have false-positive findings on respiratory culture and need no additional workup or treatment. But positive respiratory cultures may also indicate underlying serious lung disease. A thorough history to detect symptoms, underlying chronic lung disease, or an immunocompromising state followed by targeted laboratory tests and radiologic evaluation are adequate to ascertain the significance of this finding in the vast majority of patients.
THREE MAJOR GROUPS OF DISEASE
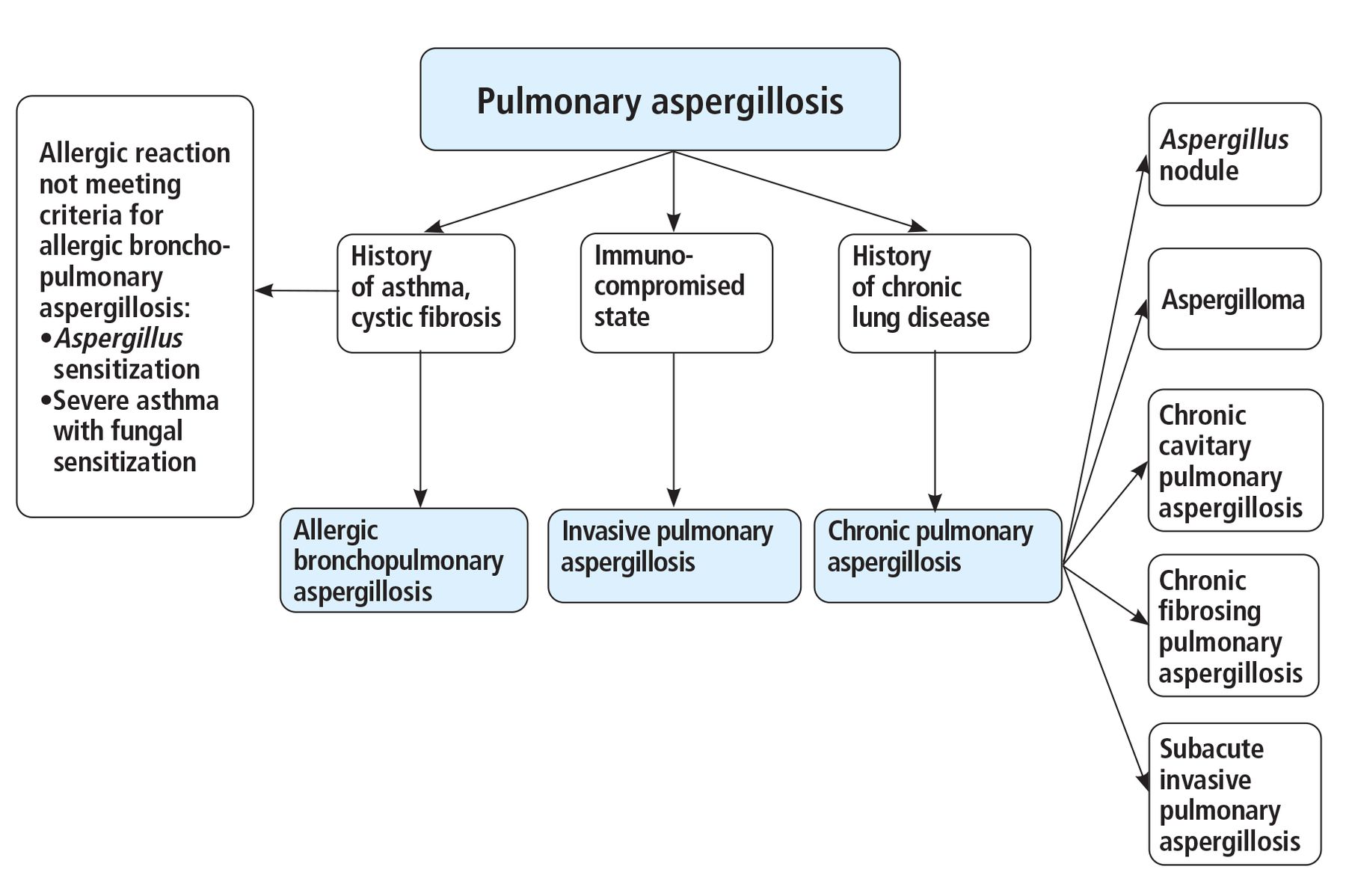
Aspergillus is an environmentally ubiquitous and easily aerosolized mold encountered through daily exposure.1 Broadly, Aspergillus-related lung diseases can be categorized into 3 major groups (Figure 1).

Pulmonary aspergillosis types, based on the patient’s medical history.
Allergic bronchopulmonary aspergillosis (ABPA) is an inflammatory lung condition caused by hypersensitivity reaction to Aspergillus antigens that almost exclusively occurs in patients with asthma or cystic fibrosis.2 Allergic reactions that do not fulfill the criteria for ABPA include Aspergillus sensitization and severe asthma with fungal sensitization.
Invasive pulmonary aspergillosis (IPA). IPA, unlike ABPA and chronic aspergillosis, is a severe, life-threatening, and often systemic disease process caused by Aspergillus species invading blood vessels, classically presenting in severely immunocompromised hosts and critically ill patients.3 A rare form of IPA is invasive Aspergillus tracheobronchitis.
Chronic pulmonary aspergillosis is an umbrella term for a spectrum of disease patterns typically occurring in immunocompetent hosts with underlying lung diseases such as tuberculosis, chronic obstructive pulmonary disease, sarcoidosis, lung cancer, and lung radiation exposure and presenting with cavitary lesions that may progress slowly over time.4
WHEN IS A POSITIVE CULTURE CLINICALLY SIGNIFICANT?
Aspergillus infections, most commonly with A fumigatus and A flavus, account for approximately 15,000 hospitalizations and an estimated $1.2 billion in hospital costs annually across the United States.5 Therefore, it is not uncommon for physicians to encounter an Aspergillus-positive respiratory culture in the clinical setting. This begets the question, Is the finding clinically significant?
In an adult patient without significant medical history, isolation of Aspergillus species in respiratory culture is likely a false-positive finding due to contamination or colonization of the respiratory flora by these ubiquitous fungal organisms. In hospitalized patients who undergo routine respiratory cultures, 80% to 90% of those with positive Aspergillus findings do not have significant aspergillosis lung disease.6,7 Even in patients with proven Aspergillus pulmonary infection, respiratory cultures are positive in 20% to 50% of patients, and as such the isolation of Aspergillus in respiratory cultures is neither sensitive nor specific in the diagnosis of most fungal respiratory infections and is not an integral part of the diagnostic criteria for Aspergillus-related lung diseases.8 Under these circumstances, in a patient who has no underlying lung disease and no immunocompromised state, we recommend observation and no further diagnostic or therapeutic intervention.
On the other hand, in a patient with respiratory symptoms, critical illness, underlying chronic lung disease, or an immunocompromising condition, detection of Aspergillus in respiratory culture may indicate underlying Aspergillus lung disease.3 In these situations, we recommend additional workup, and if the Aspergillus is proven to be the causative agent, then appropriate treatment should be started.
THE HISTORY AND PHYSICAL
It is imperative to assess the patient’s history to quickly identify risk factors for pulmonary aspergillosis. We recommend first obtaining a thorough history and physical examination for all patients.
Key factors to consider include symptoms such as hemoptysis, chest pain, fever, and recent respiratory illness. Carefully assess for underlying chronic lung conditions including asthma, cystic fibrosis, chronic obstructive pulmonary disease, tuberculosis, lung surgery, radiation, pneumoconiosis, or sarcoidosis. In addition, a thorough evaluation should be done for conditions that may affect the immune system including leukemia, hematopoietic stem cell or solid-organ transplant, immunosuppressive therapy, and chronic corticosteroid therapy.3,5–10 In immunocompromised patients who present with sepsis and demonstrate tachypnea, tachycardia, fever, hypotension, and hypoxia, IPA should be considered, and rapid identification and treatment of the causative agent are crucial, as the mortality rate is high.
LABORATORY TESTS AND IMAGING
In patients with clinical presentations suggestive of aspergillosis, we suggest pairing a basic laboratory assessment (ie, a complete blood cell count) with radiographic imaging. Initial laboratory findings may narrow the differential diagnosis by identifying eosinophilia, which suggests ABPA, or severe neutropenia, which suggests IPA.
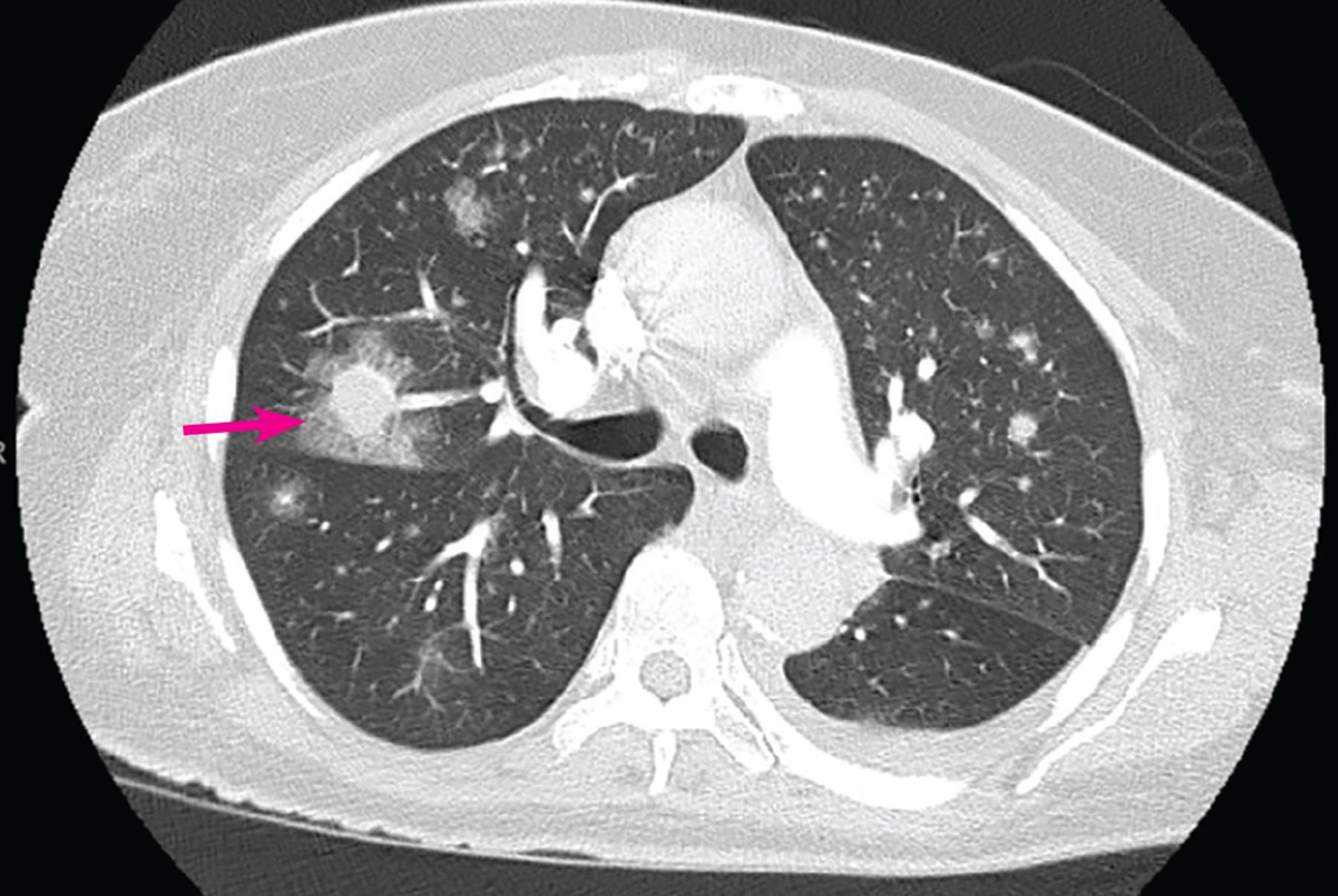
For imaging, we recommend high-resolution computed tomography (CT) of the chest rather than chest radiography to evaluate for Aspergillus-related lung disease, as it has superior ability to identify nodules, consolidation, cavitary lesions, and bronchiectasis. The finding of a cavitary lesion with or without intracavitary radiopacity suggests chronic aspergillosis, whereas the “halo” sign or “air crescent” sign suggests IPA (Figure 2), and bronchiectasis is seen in patients with ABPA.11 In evaluating chest CT findings, it is always useful to compare against previous imaging results and to consider other conditions that may coexist with positive Aspergillus in the respiratory sample.
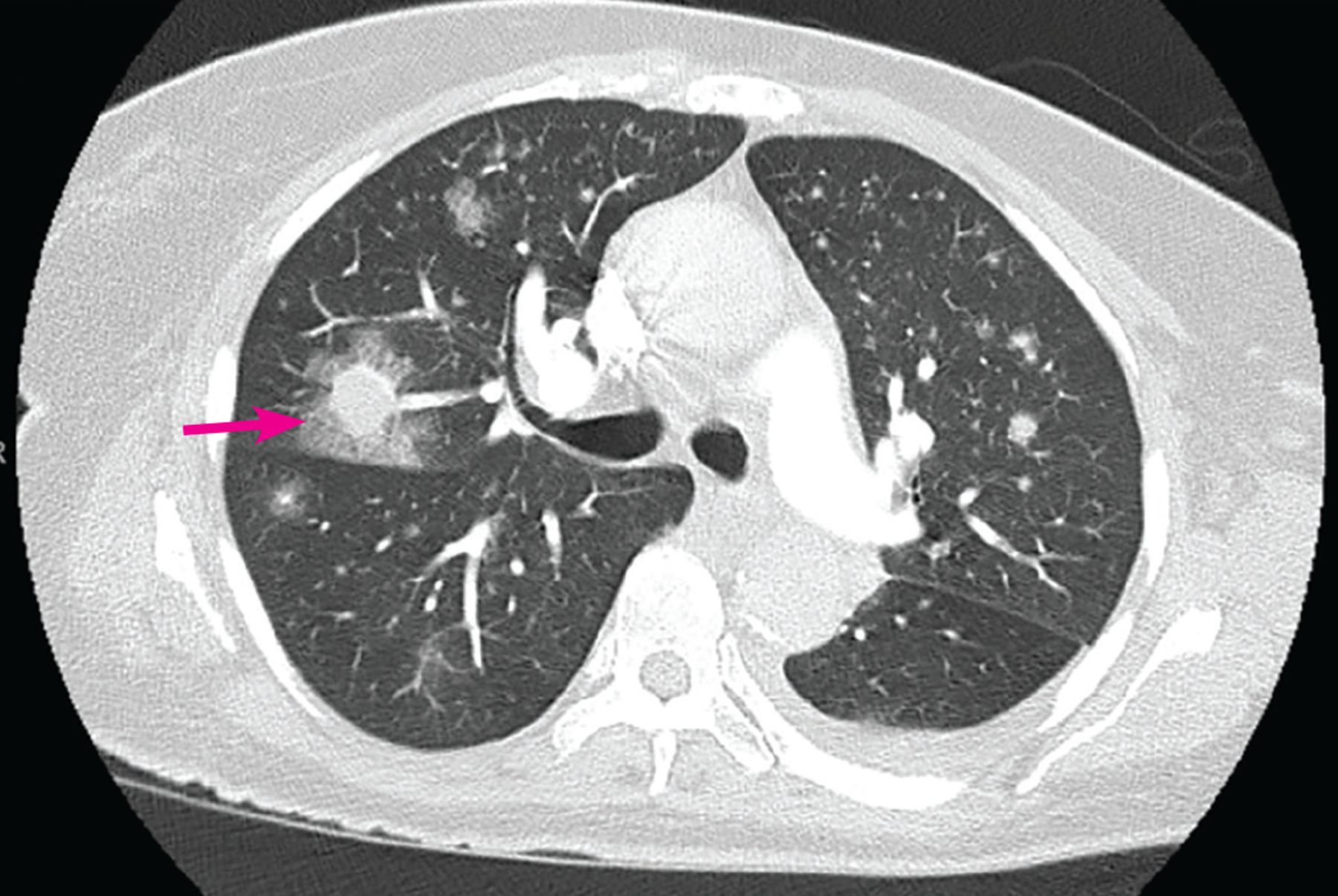
Computed tomography shows multiple pulmonary nodules, some surrounded by ground-glass changes consistent with the “halo” sign (arrow) in a patient with invasive pulmonary aspergillosis.
Galactomannan and beta-D-glucan
In patients with risk factors and suspicious imaging findings, we recommend next testing for the serologic markers galactomannan and beta-D-glucan.
The specificity and sensitivity of these tests in the diagnosis of IPA depend on the host and cutoff value. When a cutoff assay index of 0.5 is used, the combined sensitivity for serum galactomannan has been calculated as 74% (95% confidence interval [CI] 64–82) and its sensitivity as 85% (95% CI 77–90). Serum beta-D-glucan had a sensitivity of 81% (95% CI 73–87) and specificity of 61% (95% CI 46–75).10
The detection of galactomannan in bronchoalveolar lavage fluid is more sensitive and specific in the diagnosis of IPA, with a combined sensitivity of 79% (95% CI 65–88) and specificity of 84% (95% CI 74–91). The procedure is relatively safe and should be considered in patients who have risk factors or have significant radiologic findings that suggest Aspergillus lung disease.
If the clinical or radiologic picture suggests ABPA, measuring serum total and Aspergillus-specific immunoglobulin E levels is needed to confirm the diagnosis.
Biopsy is the gold standard but rarely needed
The gold standard for diagnosis of most cases of Aspergillus-related lung disease is surgical biopsy and histopathologic confirmation. Unfortunately, biopsy often cannot be done owing to concomitant pulmonary comorbidities, severe immunocompromise, or critical illness with respiratory failure. Innovations in bronchoscopic procedures for microbiologic and pathologic samples, coupled with advances in radiology and Aspergillus biomarkers, have significantly reduced the need for surgical lung biopsy in these patients.
MANAGEMENT
Management depends on the Aspergillus-related diagnosis and the patient’s clinical status. When considering conditions such as ABPA or chronic aspergillosis, we suggest waiting until the diagnosis is confirmed before initiating treatment.
However, IPA is more rapidly progressive and has a high mortality rate. Therefore, if clinical suspicion is high, therapy should not be delayed for the establishment of the diagnosis of proven or probable disease. In these situations, we suggest starting empiric therapy with a triazole agent while waiting for the results of cultures and biomarkers.
ALWAYS CONSIDER THE CLINICAL PICTURE
Due to the ubiquity of Aspergillus, many patients have false-positive findings on respiratory culture and require no additional workup or treatment. However, Aspergillus-positive respiratory cultures may be an indication of underlying serious Aspergillus lung disease. A thorough history to detect symptoms, underlying chronic lung disease, or immunocompromising state, followed by targeted laboratory tests and radiologic evaluation, is adequate to ascertain the significance of this finding in most patients.
DISCLOSURES
The authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
- Copyright © 2021 The Cleveland Clinic Foundation. All Rights Reserved.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.