


A 55-year-old woman presented 1 hour after noticing tongue discomfort while eating. On self-examination, she had noticed a rapidly expanding dark purple mass. She had experienced similar episodes previously, but in each case, the mass had ruptured in a day or 2 and healed within a week.
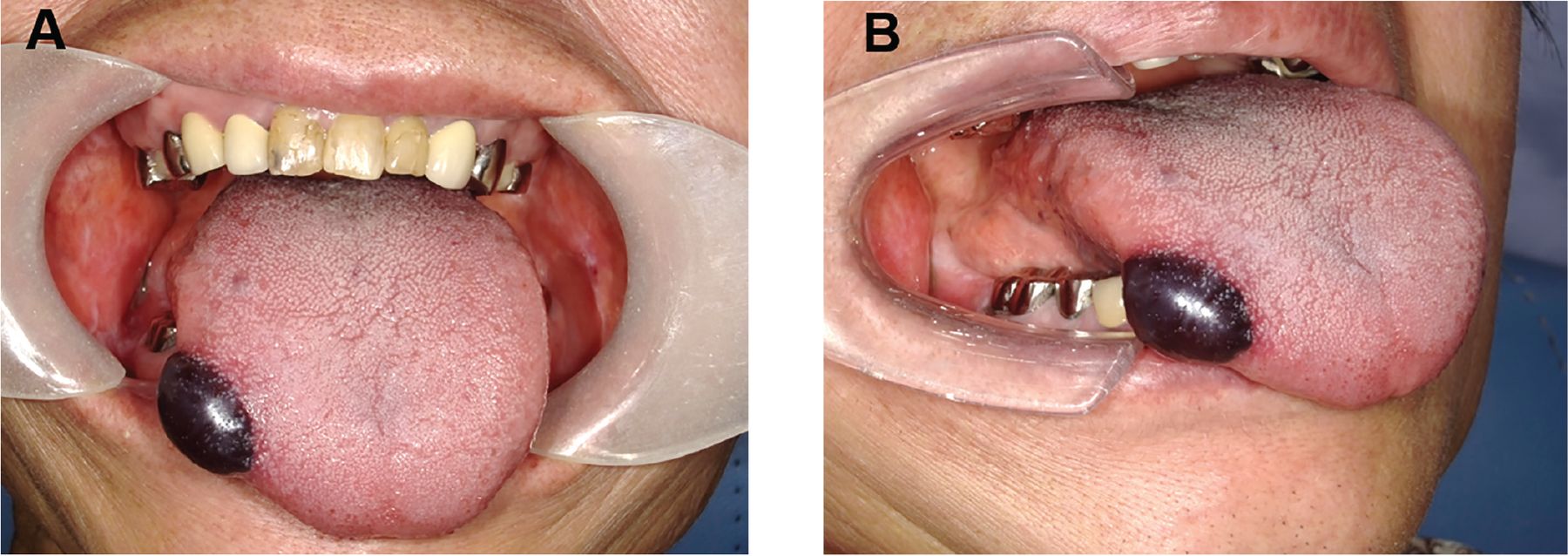
The patient had no significant medical history. On examination, a dark purple mass was noted (Figure 1). Results of blood tests were normal, and bleeding diathesis was ruled out. The patient was diagnosed with angina bullosa hemorrhagica and advised that it may recur in other parts of the oral cavity and pharynx, could cause dyspnea if in the pharynx, and caution should be exercised.
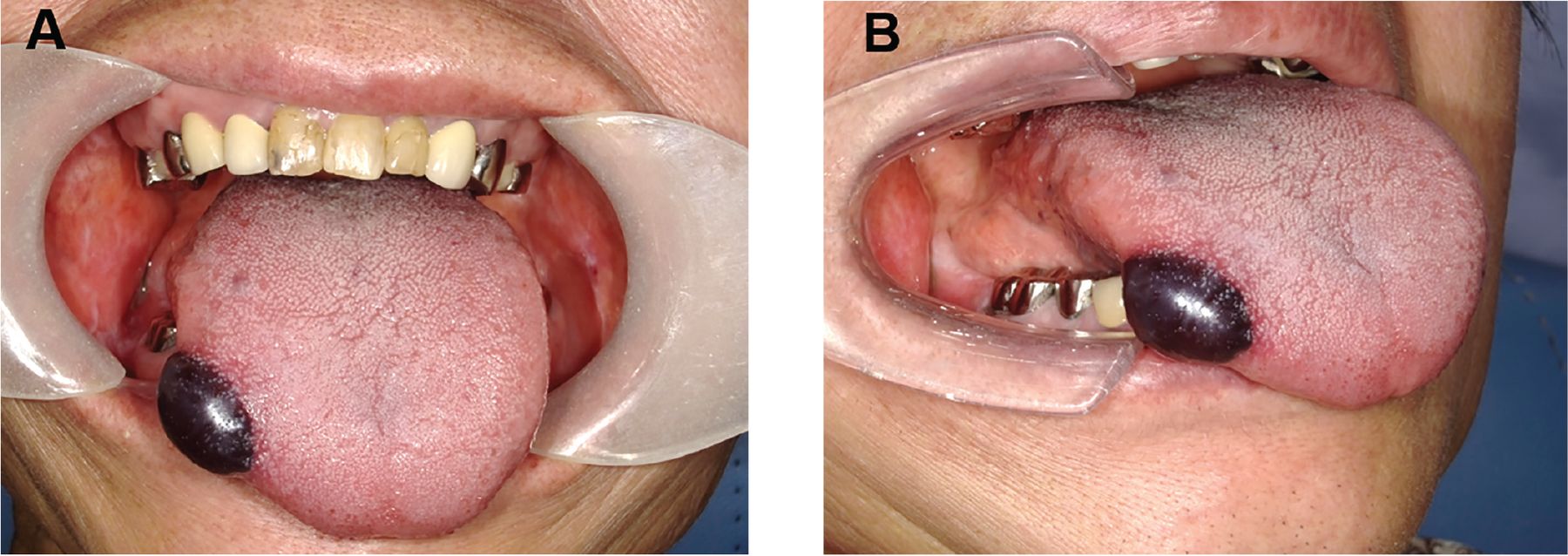
Oral findings at the first visit. (A) Front view. (B) Side view. A well-defined, round, dark purple mass was seen on the right lateral border of the tongue.
After returning home, the patient pressed her tongue against her teeth; the mass ruptured, and a slightly painful erosion formed that spontaneously healed without scarring after approximately 2 weeks.
FEATURES OF ANGINA BULLOSA HEMORRHAGICA
Angina bullosa hemorrhagica is a condition with unknown etiology, in which hemorrhagic blisters (hematomas) spontaneously arise in the oral cavity, regardless of blood abnormalities or systemic diseases.1 It frequently occurs on the soft palate, buccal mucosa, and tongue, and only rarely on the masticatory mucosa such as the gingiva and hard palate. The lesions predominantly occur in middle-aged and older individuals, and only rarely in children.1–5
Angina bullosa hemorrhagica frequently occurs during or immediately after ingestion of hard foods and hot beverages, which may result in trauma to the mucous membranes.2 Studies have also reported lesions in patients with a history of inhaled corticosteroid use, fragility of blood vessels, diabetes, and hypertension.3,5
The differential diagnosis includes dermatoses that present as mucocutaneous bullous lesions, such as pemphigus vulgaris, mucous membrane pemphigoid, bullous pemphigoid, amyloidosis, acquired epidermolysis bullosa, linear immunoglobulin A dermatosis, herpetiformis dermatitis, and oral bullous lichen planus, as well as hematologic diseases such as leukemia, thrombocytopenia, and von Willebrand disease.1,2
Angina bullosa hemorrhagica is benign and often heals spontaneously, so no specific treatment is required.1–5 However, airway obstruction due to hematoma has been reported.4 In particular, softpalate hematomas should be incised and drained to avoid a possible obstruction of the upper aerodigestive tract.1,5 In addition, owing to frequent recurrence and unknown etiology, follow-up to avoid misdiagnosis is needed.
DISCLOSURES
The authors report no relevant financial relationship which, in the context of their contributions could be perceived as a potential conflict of interest.
- Copyright © 2022 The Cleveland Clinic Foundation. All Rights Reserved.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.