


ABSTRACT
Benign paroxysmal positional vertigo (BPPV), caused by wayward crystals (“rocks”) in the semicircular canals of the inner ear, is the most common cause of brief symptoms of vertigo secondary to head and body movements. Diagnosing and treating it are simple to do in the medical office. This article reviews the differential diagnosis for patients presenting with dizziness and vertigo, the pathophysiology of BPPV, how to diagnose it using maneuvers to elicit symptoms and nystagmus, how to interpret the nystagmus pattern to determine where the rocks are, and how to treat it using different maneuvers to reposition (“roll”) the rocks back where they belong.
BPPV symptoms typically last seconds to minutes and are not associated with hearing loss or other neurologic signs or symptoms.
Dizziness or vertigo when lying down or changing positions is a strong predictor of BPPV. The condition is easily diagnosed with the Dix-Hallpike and supine roll maneuvers.
Treatment can be done by a general practitioner or by a specialist in vestibular rehabilitation or vestibular audiology. If repositioning maneuvers do not relieve the symptoms, a full workup, including radiographic imaging and a vestibular test battery, should be considered.
Dizziness is a common complaint that can affect people of all ages: roughly 15% of American adults report a balance or dizziness problem.1 It is the reason for many emergency room visits, secondary to benign conditions (eg, vestibular conditions, migraine, psychogenic conditions) and serious conditions (eg, stroke, inflammatory central nervous system disease, intracranial tumor, or hemorrhage).
Unfortunately, balance disorders are often difficult to diagnose and manage, owing in part to the subjective symptoms and the complexity of the neurologic, cardiovascular, metabolic, toxic, vestibular, and psychiatric conditions that can cause them. The symptoms can also be similar to those of life-threatening conditions, making the diagnostic workup challenging.
This article provides an update on benign paroxysmal positional vertigo (BPPV), a common balance disorder, and how to distinguish it from other causes of dizziness, vertigo, and imbalance with easy position-changing maneuvers. We also discuss how best to treat it, also with position-changing maneuvers.
DIZZINESS VS VERTIGO
Patients use the term dizziness to describe several different sensations, but medically speaking it is different from vertigo. Dizziness is any distortion of the sensation of where one is within a space, whereas vertigo is a false sensation of movement, specifically rotation or spinning.2
A thorough case history can differentiate between these sensations and point to a cause.
Questions should focus on the following:
Quality of symptoms, such as vertigo, oscillopsia (the illusion that objects are moving back and forth), general imbalance, or lightheadedness
Time course of symptoms, such as speed of onset, duration, the circumstance of onset, time since the initial episode, and frequency of episodes
Associated factors, such as migraine or changes in vision, hearing, or breathing
Exacerbating and relieving factors, such as head or body movements, closing or opening the eyes, looking in one direction or another, entering or leaving a busy visual field, coughing, sneezing, or loud sounds
Other pertinent medical history, such as issues with vision, disabilities of the lower extremities, medications that can cause dizziness, diabetes, neuropathy, cerebrovascular disease, stroke, neck pain, seizures, hypertension, cardiac problems, or ototoxicity.
Common vestibular disorders have typical characteristics (Table 1)3,4 that are key to quickly narrowing down the cause of symptoms and making appropriate referrals.
Symptoms and temporal pattern of common disorders of dizziness
A COMMON CAUSE OF DIZZINESS AND VERTIGO
BPPV is one of the most common vestibular causes of dizziness. Royl et al5 reported that it was the most frequent diagnosis in patients presenting to the emergency department with dizziness. Its prevalence increases with age, and it more often affects people over age 40. It is more common in women than in men.6
Even though BPPV is common, it often goes unrecognized,7 leading to costly and unnecessary diagnostic procedures, referrals, and treatment. Undetected and untreated, BPPV can also lead to poor quality of life and to falls,8 the leading cause of injury and trauma-related hospital admissions in older adults.9
BRIEF EPISODES OF VERTIGO, ASSOCIATED WITH MOVEMENT
BPPV presents as brief episodes of vertigo, typically lasting seconds to minutes and associated with head movement, neck movement, or overall positional changes.1 Common triggers include:
Rolling over in bed
Looking up or down
Rising from a supine position
Lying down from a sitting position
Leaning forward.
There can be a short-lasting latency of seconds between the initial positional change and corresponding symptoms. Patients may also experience nausea or emesis during an episode and report a general sense of floating or imbalance.
CAUSES OF BPPV
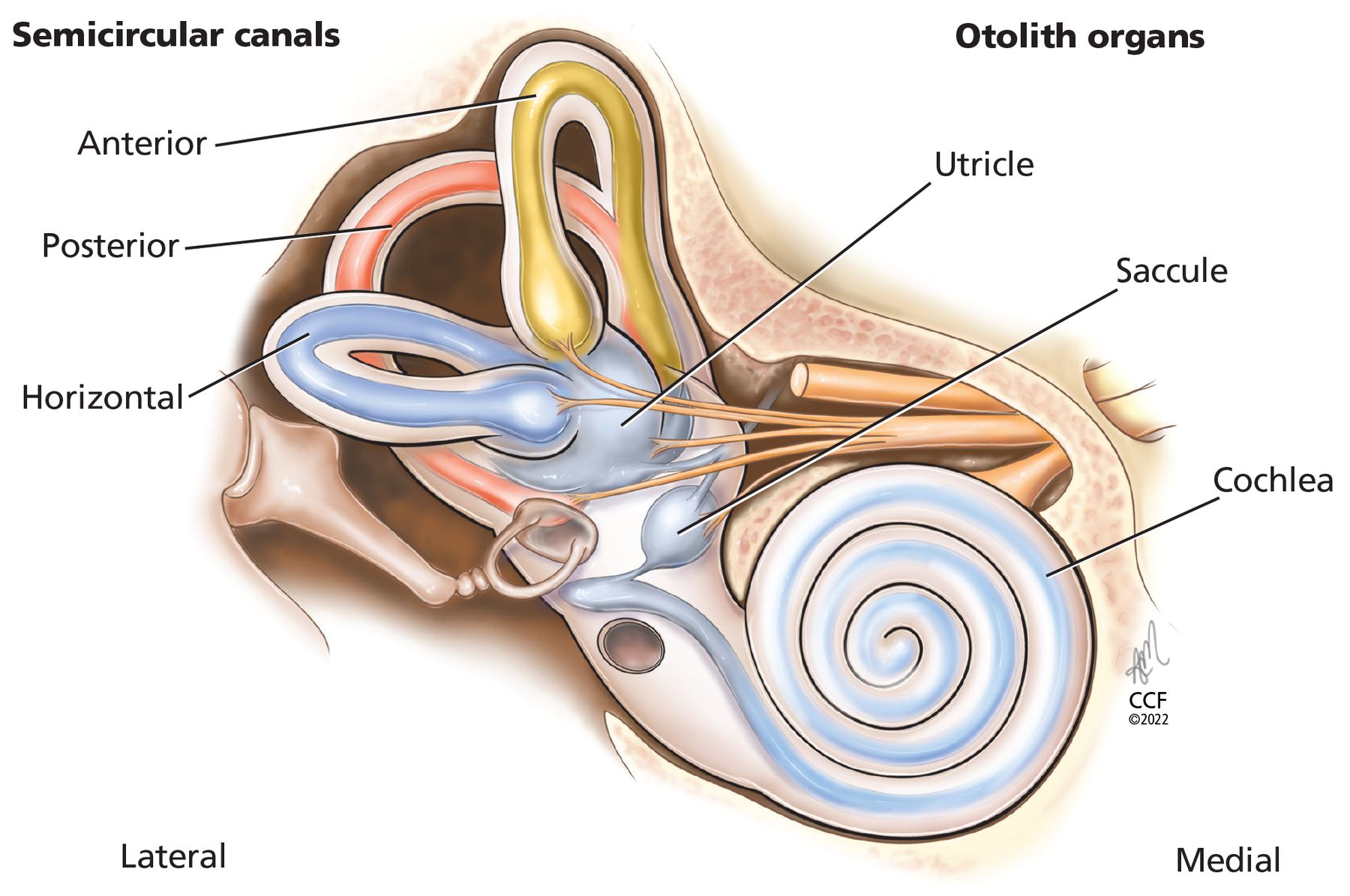
Deep within the petrous part of the temporal bone lies the membranous labyrinth, housed within the bony labyrinth (Figure 1). The membranous labyrinth is filled with fluid (endolymph) and houses the cochlea and the vestibular structures: the 3 semicircular canals–anterior, posterior, and horizontal (also called lateral)—and the 2 otolith organs (saccule and utricle). The semicircular canals sense angular acceleration, and the otolith organs sense linear acceleration, providing our internal cues for orientation of position in space, movement, gaze stabilization, and postural control.

The semicircular canals (anterior, posterior, horizontal) sense angular acceleration, and the otolith organs (saccule, uticle) sense linear acceleration, providing internal cues for orientation of position in space, movement, gaze stabilization, and postural control.
Body movements cause the fluid in the semicircular canals to move and stimulate cilia on sensory hair cells. This triggers transmission of neural signals to the brain to initiate appropriate reflex responses for the eyes, head, and postural adjustments. These reflexive movements allow us to see things clearly when our head and body are in motion and keep us from falling.
The 3 semicircular canals are positioned at 90-degree angles to one another and thus can sense rotation in all directions. The 3 in the right ear are functionally paired with the 3 in the left ear:
The right horizontal with the left horizontal
The right anterior with the left posterior
The right posterior with the left anterior.
Thus, for instance, when turning one’s head to look over the right shoulder, the right horizontal semicircular canal is excited and the left horizontal is inhibited.
The utricle and saccule are gravity-sensitive and contain dense crystals called otoconia resting on top of the sensory organs. With linear movements (eg, leaning to the side), the otoconia move, signaling reflexive responses similar to those of the semicircular canals to maintain eye, head, and body equilibrium.
BPPV is caused by free-floating otoconia that have been dislodged from the otolith organs as a result of injury, infection, diabetes, migraine, osteoporosis, prolonged bedrest, or aging.10 Dislodged otoconia can gather in the semicircular canals. Since each semicircular canal is oriented in a different plane in space, when the dislodged otoconia gather in 1 or more of them, they can be stimulated upon positional changes and cause vertigo and nystagmus.
Most cases of BPPV are either idiopathic or caused by head trauma,11 but it can be a result of other vestibular disorders (eg, Menière disease, labyrinthitis) or central nervous system disorders (eg, migraine, multiple sclerosis).
Recent evidence suggests BPPV has a seasonal aspect, perhaps related to varying vitamin D levels throughout the year. Otoconia are composed of calcium carbonate and therefore could have risk factors for demineralization, similar to bone. Maia et al12 analyzed 214 patients diagnosed with idiopathic BPPV in Brazil over 5 years and found that significantly more patients presented in the autumn and winter than in the spring and summer. This suggests that lower vitamin D levels, due to less sunlight, could be contributing to the seasonality of BPPV.
DIAGNOSTIC MANEUVERS
BPPV is relatively simple to diagnose and treat. By moving the patient into different positions, observing their eye movements, and asking if they feel like their head is spinning, clinicians can determine which semicircular canal is being stimulated. Otoconia in the posterior semicircular canal account for up to 90% of cases, and otoconia in the horizontal canal account for most of the rest, while involvement of the anterior semicircular canal is relatively rare and is usually due to failed repositioning maneuvers to remove otoconia from the posterior canal.13
Nystagmus consists of oscillation of the eyes14 and can be horizontal (to the side and back), torsional (rotary in nature), or vertical (up or down and back), or a combination of some or all three. The direction and characteristics of the eye movements correspond to the semicircular canal stimulated during positioning (Table 2). The symptoms are brief, often lasting less than 60 seconds.
Observed nystagmus patterns based on semicircular canal involvement
Dix-Hallpike maneuver
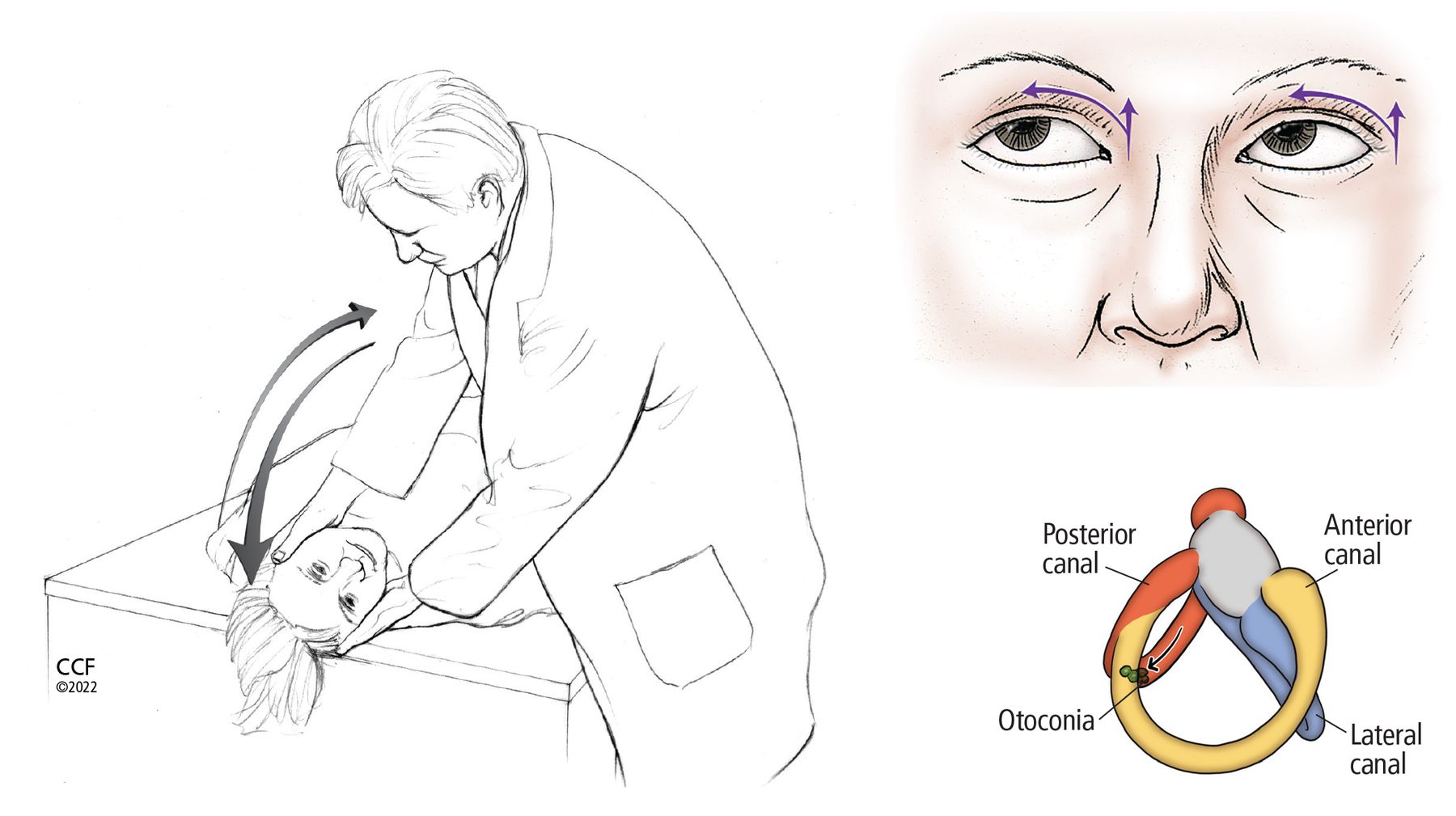
The variants of BPPV affecting the vertical semicircular canals (ie, the posterior and anterior) are diagnosed by performing the Dix-Hallpike maneuver.15 This consists of 2 positional changes (sitting to supine, and supine to sitting) with the patient’s head turned 45° (Figure 2).16 When the patient is moved from the sitting to the supine position, the clinician may observe the excitatory eye movement pattern of the canal with the otoconia, with horizontal nystagmus toward the involved ear and either of the following:
Up (if the otoconia are in the posterior canal)
Down (if they are in the anterior canal).

The Dix-Hallpike maneuver to detect otoconia in the posterior or anterior semicircular canals. If the otoconia are suspected to be in the right ear, the patient sits upright with the head turned 45° to the right; if the otoconia are suspected to be in the left ear, the patient turns the head to the left. The clinician then quickly moves the patient into a head-hanging supine position and checks for signs of nystagmus, and the patient reports any symptoms (eg, dizziness, vertigo). After 60 seconds, the patient is returned to a seated position with the head still turned, and the clinician again observes symptoms and signs. During the maneuver, movement of otoconia within the right posterior semicircular canal (in the lower-right image) causes an excitatory response—ie, nystagmus—to the right and up, as the arrows indicate in the upper-right image.
When the patient moves from supine back to sitting, a reverse nystagmus pattern should be observed, indicating inhibition of the canal with the otoconia, with torsional nystagmus toward the healthy side and either of the following:
Down (for the posterior canal)
Up (for the anterior canal).
The maneuver is then repeated with the patient’s head turned the other way, ie, to assess both right and left sides.
Supine roll test
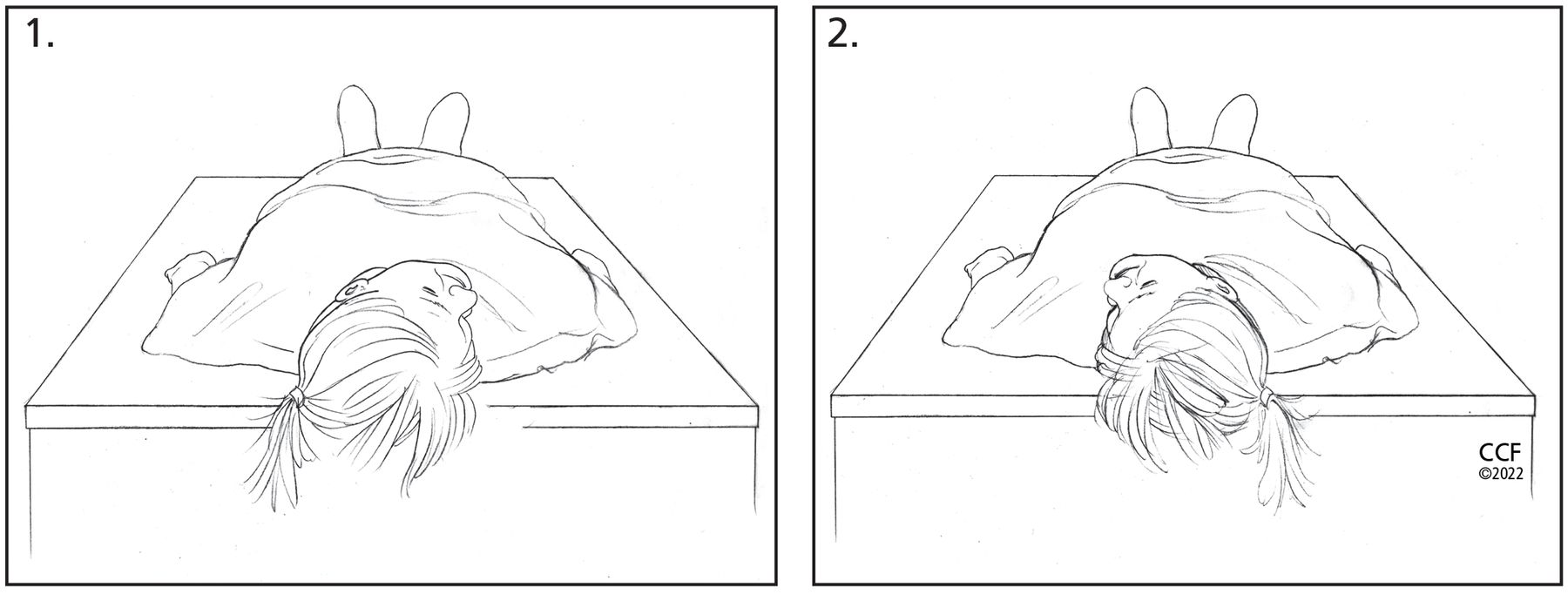
The Dix-Hallpike maneuver may not always elicit vertigo and nystagmus in cases of BPPV that are due to otoconia in the horizontal semicircular canal. Therefore, the supine roll test is recommended as the second screening maneuver (Figure 3).16

The supine roll test to detect otoconia in the horizontal semicircular canals. (A) With the patient in a supine position, the clinician quickly rotates the patient’s head to the right and assesses for horizontal nystagmus and patient symptoms. (B) After 30 to 60 seconds, the clinician quickly rotates the patient’s head to the left and again observes for horizontal nystagmus and symptoms. The direction of nystagmus (ie, geotropic vs apogeotropic) with the head-movement changes indicates the involved horizontal canal (Table 2).
A positive sign of BPPV during this test is horizontal nystagmus in both the head-right and head-left positions. If the nystagmus is in the same direction that the head is turned, the pattern is called geotropic. If it is in the opposite direction, the pattern is called apogeotropic.
Refer when in doubt
Recent clinical practice guidelines outline that proper diagnosis of BPPV is made when both patient-reported symptoms and the appropriate nystagmus pattern are observed during position changes.17 However, false-negative results can occur. When BPPV is strongly suspected based on history but the Dix-Hallpike and supine roll maneuvers are negative, the patient should be referred to a vestibular therapist or vestibular audiologist for further evaluation.
TREATMENT MANEUVERS
Once BPPV has been diagnosed, treatment is based on the semicircular canal involved. This involves a series of clinician-guided head and body movements to move the otoconia out of the semicircular canal and back into the utricle, with the assistance of gravity. The process is simple and can be performed on a standard examination chair that can fully recline, or on a table. These maneuvers can often provide immediate and long-lasting relief.10 In several studies, their effectiveness ranged from roughly 76% to 93%.18–20
Epley maneuver for posterior or anterior canal BPPV
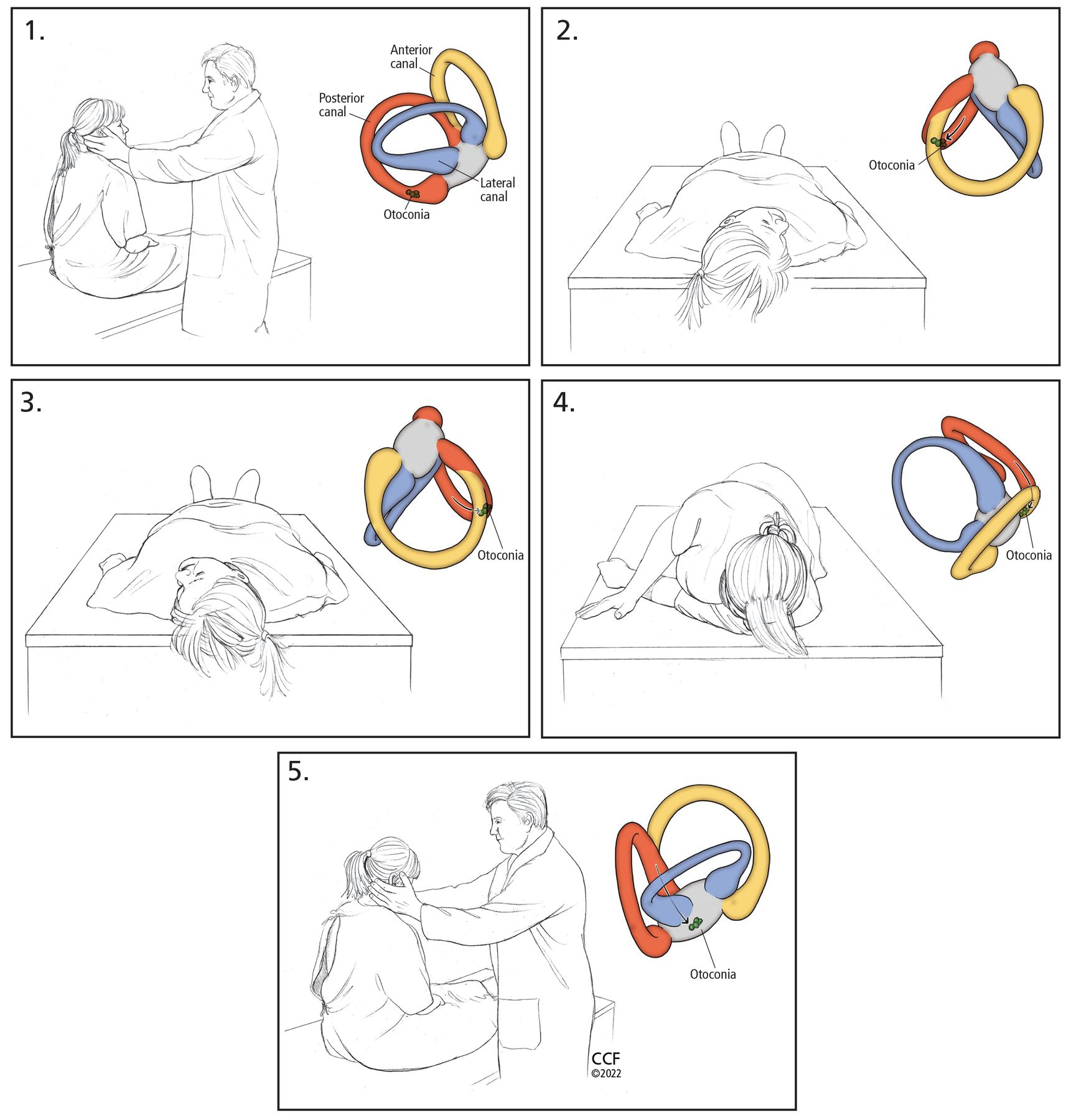
In 1992, Epley21 described a series of head and body movements to move otoconia out of the vertical (ie, the posterior and anterior) semicircular canals. The procedure is easy to perform but requires careful attention to keep the patient’s head and body in the proper position throughout the maneuver (Figure 4).16 Also, the patient’s eyes should be monitored throughout each stage of the maneuver to observe the pattern of nystagmus, which should remain consistent with that observed during the Dix-Hallpike or supine roll maneuver. Consistent nystagmus patterns ensure that the clinician has not moved the otoconia to a different semicircular canal rather than the otolith organs.

The Epley maneuver to clear otoconia from the posterior or anterior semicircular canals:
Place the patient in a seated position on the bed and turn their head 45° toward the ear with the suspected otoconia. The color insets show movement of otoconia.
Quickly move the patient to a supine position with head turned and extended downward.
Move the patient’s head to the other side, being careful to keep it in the correct plane. The final position after turn should be 45° toward the unaffected ear, extended downward.
Assist the patient onto the unaffected side with the patient’s chin remaining 45° toward the unaffected ear (patient will be looking toward the ground in this position).
Finally, help the patient back to a seated position, keeping their head turned over their shoulder.
Semont maneuver, an alternative to the Epley maneuver
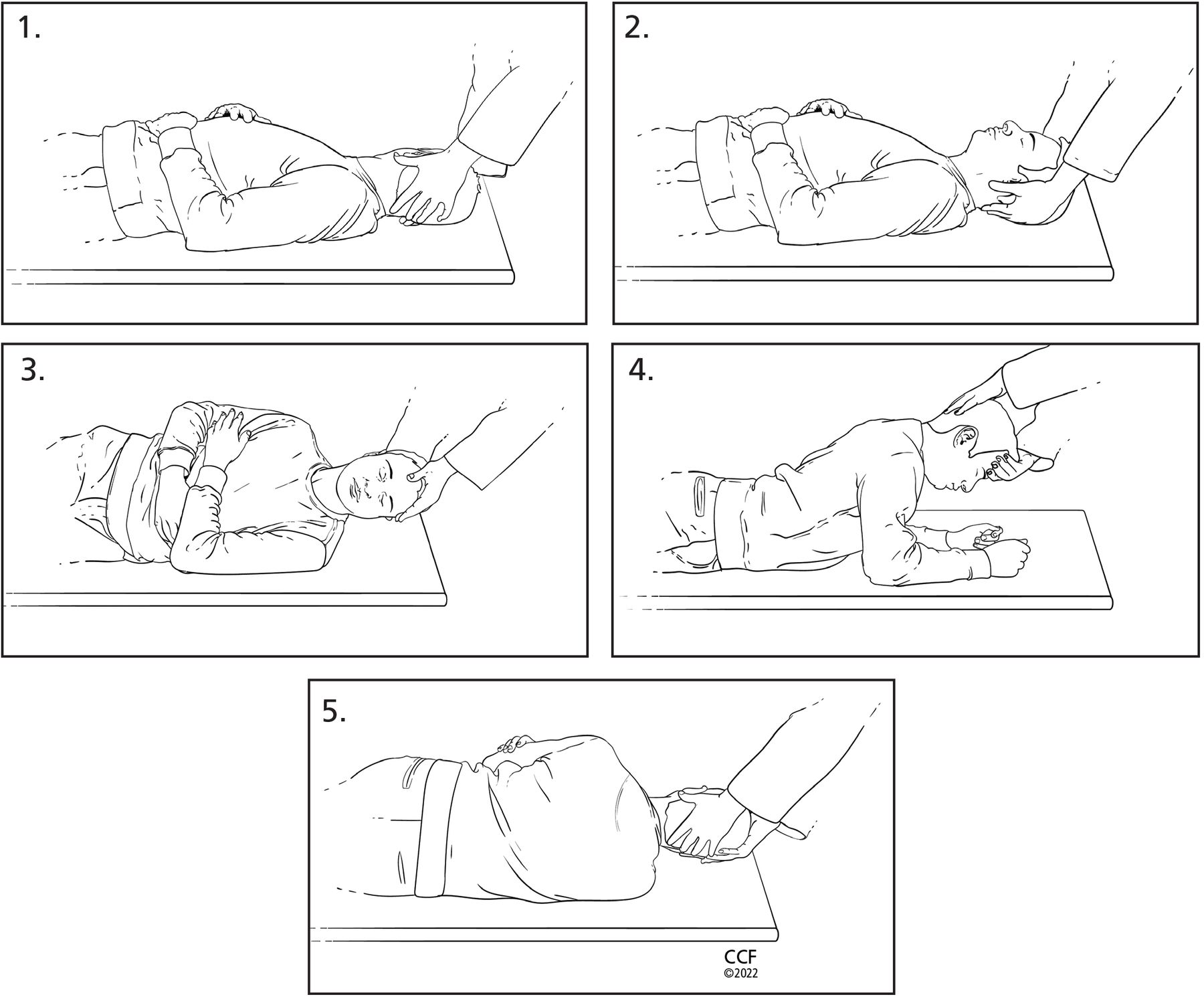
The Semont maneuver is a suitable alternative to the Epley maneuver for treating vertical canal BPPV.22 This maneuver requires quickly moving the patient through a series of head and body positions (Figure 5).

Semont maneuver, an alternative way to clear otoconia from the posterior or anterior canals:
Place the patient in a seated position on the bed and turn the head 45° away from the ear with the suspected otoconia in the vertical semicircular canal.
Quickly move the patient on their side with the nose facing the ceiling.
Quickly move the patient back up and onto their other side with the head in the same 45° angle with the nose facing toward the ground. The examiner then assists the patient to a seated position, keeping the head at 45° away from the ear with suspected vertical semicircular canal benign paroxysmal positional vertigo (BPPV).
Note: The head position described in step 1 is used for posterior semicircular canal BPPV. The patient should turn the head 45° toward the ear with suspected vertical semicircular canal BPPV if the anterior semicircular canal is affected.
As with the Epley maneuver, the clinician should focus on nystagmus patterns throughout the maneuver, which should be consistent with those observed during diagnostic screening (eg, the Dix-Hallpike maneuver).
The log roll maneuver for treating horizontal canal BPPV
As indicated above, properly diagnosing the affected side for horizontal semicircular canal BPPV requires carefully reviewing the nystagmus pattern (geotropic vs apogeotropic) during the supine roll test.
Geotropic horizontal-canal BPPV is more common than apogeotropic.17 Often, listening to the patient describe their symptoms and observing the nystagmus patterns help to determine which side is affected and should be treated. Referral to a vestibular specialist is warranted to ensure the correct side and proper treatment. Additionally, many other disorders can present with direction-changing horizontal nystagmus, and thorough evaluation to rule in or rule out BPPV should be made in these cases (see “BPPV care path” below).
Given that geotropic horizontal semicircular canal BPPV is more common than the apogeotropic variant, clinicians can perform the log roll 360° maneuver. If the apogeotropic variant is present, the Gufoni maneuver can be performed.4,17 Following the steps shown in Figure 6 ensures proper head and body placement for moving the debris out of the affected horizontal canal. It is imperative to support the patient’s head during all movements. The patient should be kept in each position until symptoms and nystagmus stop.

Log roll (360°) maneuver to clear otoconia from the horizontal semicircular canal:
Place the patient in the supine position and turn their head 90° toward the ear with the suspected otoconia in the horizontal semicircular canal.
Next, turn the patient’s head back to center, with the head elevated 30°.
Maneuver the patient onto their side (90°) toward the unaffected ear.
Move the patient into the prone position with elbows flexed. Note: Sometimes treatment can end in this position (called 270° maneuver).
Finally, help the patient back onto their back toward the ear involved, completing a complete 360° rotation.
BPPV CARE PATH
The following care path is a suggested guideline to evaluate and treat BPPV.17
Determine if the patient’s symptoms of dizziness or vertigo last seconds to minutes in response to position changes. If the patient has acute neurologic or cardiovascular symptoms, consider further workup to rule out stroke or a cardiovascular diagnosis.
Take vital signs, including blood pressure.
Check medications.
Perform cranial nerve examination; look for any nystagmus or disconjugate eye movements.
Perform the Dix-Hallpike maneuver and the supine roll maneuver. If these maneuvers elicit symptoms and nystagmus, consider treatment for BPPV (Table 3) or refer the patient to a vestibular physical therapist or vestibular audiologist to perform the treatment maneuver.
If the patient meets diagnostic criteria for BPPV and has no other symptoms or signs suggesting another otologic or neurologic disorder, do not recommend radiographic imaging or formal vestibular testing. If the patient does have separate otologic or neurologic indications or a complicated history or if the diagnosis of BPPV is unclear, a full workup should be considered including referral to an ear, nose, and throat specialist, a vestibular audiologist for formal vestibular testing, and a neurologist.
Many patients experience lingering symptoms of imbalance after successful treatment of BPPV. Consider referral to a vestibular rehabilitation program to promote compensation for and habituation to symptoms.
Patients may also find it useful to perform particle-repositioning maneuvers at home to help treat recurrent or persistent BPPV. Patients may be provided with handouts on how to perform home treatment or referred to online resources (eg, https://my.clevelandclinic.org/health/diseases/11858-benign-paroxysmal-positional-vertigo-bppv).
Treatment maneuvers for BPPV, based on location of otoconia
DISCLOSURES
The authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
- Copyright © 2022 The Cleveland Clinic Foundation. All Rights Reserved.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.