


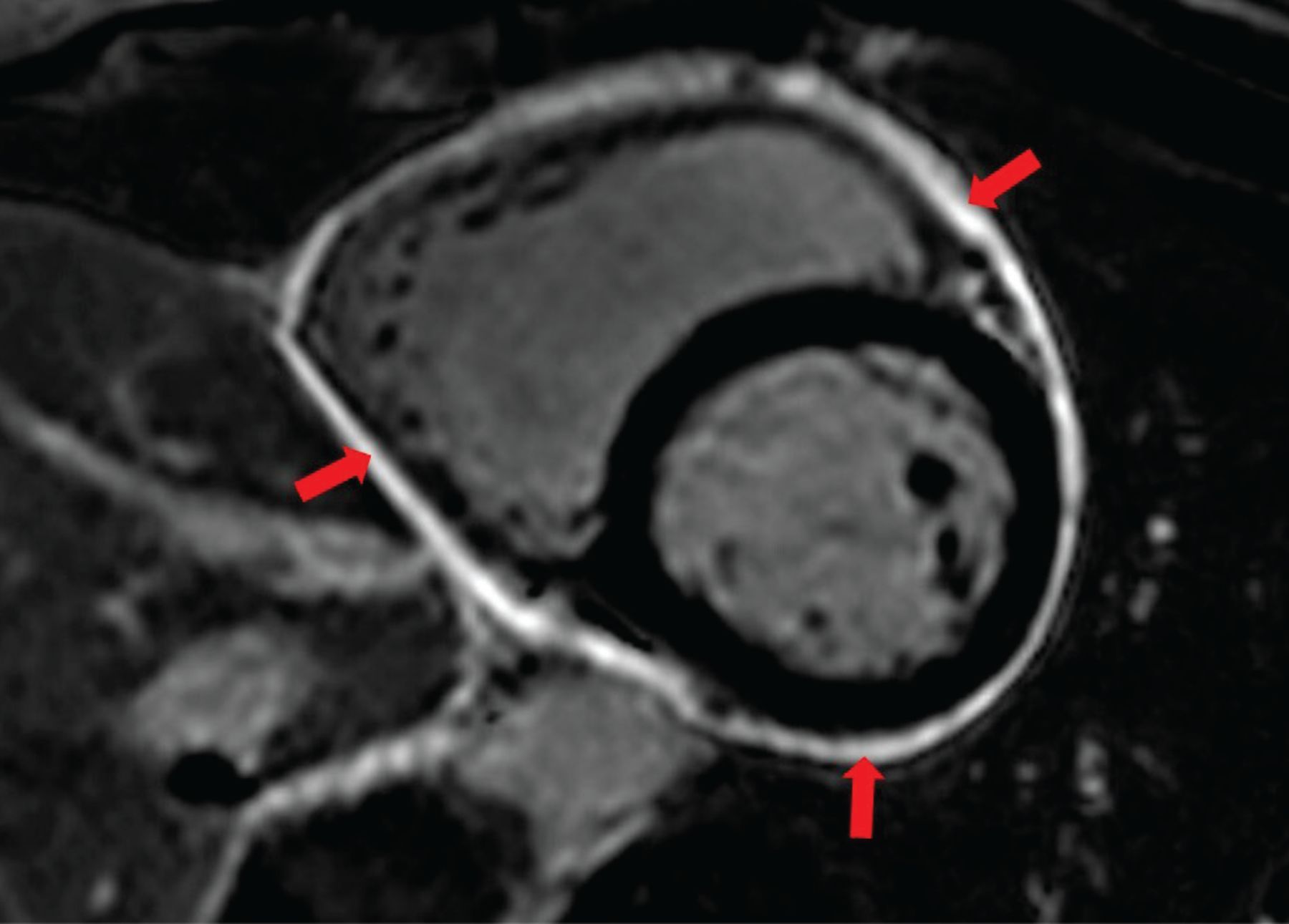
A 47-year-old woman presents with recurrent episodes of pleuritic chest pain. She is physically active and exercises 5 times per week on average, although recently she has had to stop after noticing worsening of her symptoms with strenuous exercise. Inflammatory markers are found to be elevated, and echocardiography reveals a new small pericardial effusion. Cardiac magnetic resonance imaging (MRI) with gadolinium contrast reveals circumferential delayed hyperenhancement of the pericardium (Figure 1). A diagnosis of acute pericarditis is made, and the patient is started on anti-inflammatory therapy. When is it safe to recommend resumption of her physical activity?
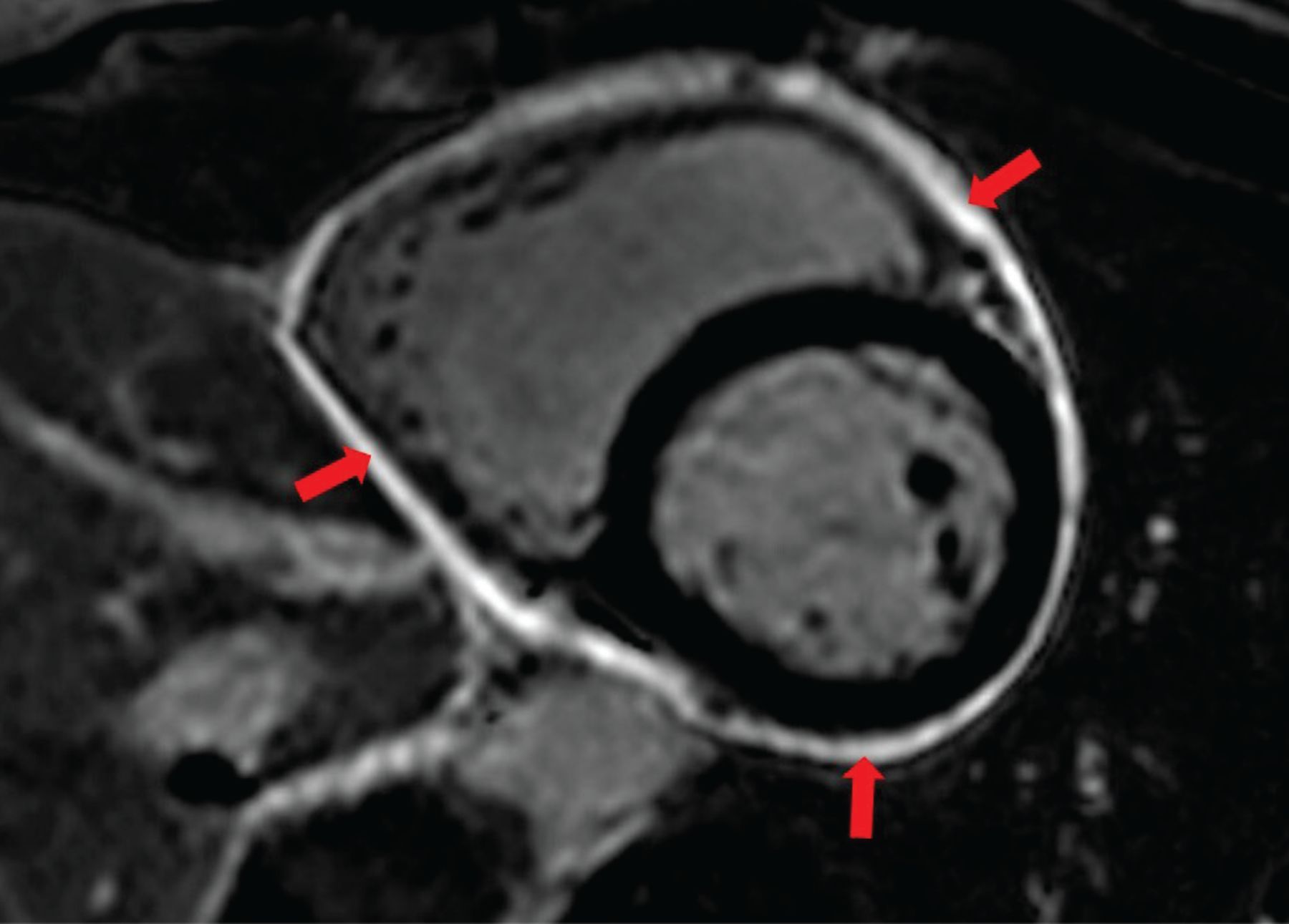
Cardiac magnetic resonance imaging with gadolinium contrast showing delayed contrast enhancement of the pericardium on fat-suppression imaging sequences in a 47-year-old female with acute pericarditis. The arrows point to the circumferential contrast enhancement of the pericardium. Our experience suggests that complete remission may take as long as 3 to 5 years.
Although there is little published evidence, experts recommend against participation in exercise and competitive sports during episodes of acute and recurrent pericarditis and 1 to 3 months after an acute episode to ensure resolution of disease.
EXERCISE AND PERICARDITIS: TRIGGERS AND MECHANISMS
Physical exercise is thought to worsen pericardial inflammation, and it has been implicated as a trigger for inflammation in genetically predisposed patients.1,2 The proposed mechanisms include a tachycardia-mediated increase in shear stress through friction of the pericardial layers and an increase in the release of free radicals causing oxidative stress through enhanced blood supply to the pericardium.1 Additionally, extreme physical exercise in elite athletes can decrease the innate and adaptive immune response.3 However, this interplay and its relevance to the clinical course of pericarditis in elite athletes has not been studied specifically. Exercise restriction is commonly recommended to patients with pericarditis as a means to decrease symptoms and the risk of complications, even though published evidence of a causative relationship between exercise and worsening pericarditis is limited to case reports.4
Elevations in heart rate appear to be particularly implicated in worsening pericardial inflammation, and studies have shown a correlation between C-reactive protein levels and heart rate in patients hospitalized with acute pericarditis.5 Local inflammation from pericarditis has been proposed as a mechanism that worsens tachycardia, which in turn can perpetuate a vicious cycle of inflammation.6 Some experts have suggested maintaining heart rates below 100 beats per minute in patients with pericarditis, and a role has been proposed for using cardiac MRI to monitor disease activity in order to guide the resumption of exercise.4
In an observational study by Imazio et al,7 beta-blockers were administered to patients with acute pericarditis targeting a heart rate of less than 70 beats per minute. Patients who received beta-blockers had a lower rate of symptom recurrence at 3 weeks (4% vs 14%, P = .024) and a trend toward fewer recurrences at 18 months.7 Although mechanisms other than heart rate reduction, such as downregulation of proinflammatory cytokines, could contribute to symptom reduction in these patients, this study indirectly supports the contention of exercise restriction to lower heart rates in patients with acute pericarditis. Of note, no randomized clinical trials using heart-rate-lowering therapies in this patient population have been conducted.
SOCIETY GUIDELINES
Several professional societies have published recommendations on physical exercise in patients with pericarditis (Table 1),8–10 but the recommendations are generally not supported by data from randomized clinical trials and instead rely on observational data and expert opinion. Moreover, the guidelines emphasize recommendations for return to competitive sports for athletes rather than recommendations on activity levels in the general population of nonathletes.
Exercise recommendations in patients with isolated pericarditisa
The European Association of Preventive Cardiology (EAPC) released recommendations on return to play for athletes in 2019.8 They recommend against participation in competitive sports during the acute phase of pericarditis and not resuming sports activity for 1 to 3 months after resolution of the active phase. Return to play was deemed reasonable if biomarkers had normalized, left ventricular function was normal, and no resting or exercise-induced ventricular arrhythmias could be detected on 24-hour electrocardiography monitoring or exercise electrocardiography.
The European Society of Cardiology (ESC) released guidelines on sports cardiology and exercise in patients with cardiovascular disease in 2020.9 They provide more generalized recommendations for the general population of patients in terms of leisurely activity. In contrast to the EAPC recommendations, both competitive sports and leisure-time exercise are actively discouraged until complete recovery from pericarditis. Similar to the EAPC recommendations, return to activity is recommended after a period of 30 days to 3 months after resolution of disease, depending on severity.
The American Heart Association and American College of Cardiology (AHA/ACC) released a joint scientific statement in 2015 on disqualification and eligibility for competitive athletes with cardiovascular abnormalities.10 In concordance with the ESC and EAPC recommendations, the AHA/ACC statement recommends against participation in competitive sports during the acute phase of pericarditis. Return to full activity is recommended in the complete absence of evidence for the disease. They provide no specific guidance in terms of timing of return or stratification of physical activity for athletes and nonathletes.
MYOPERICARDITIS
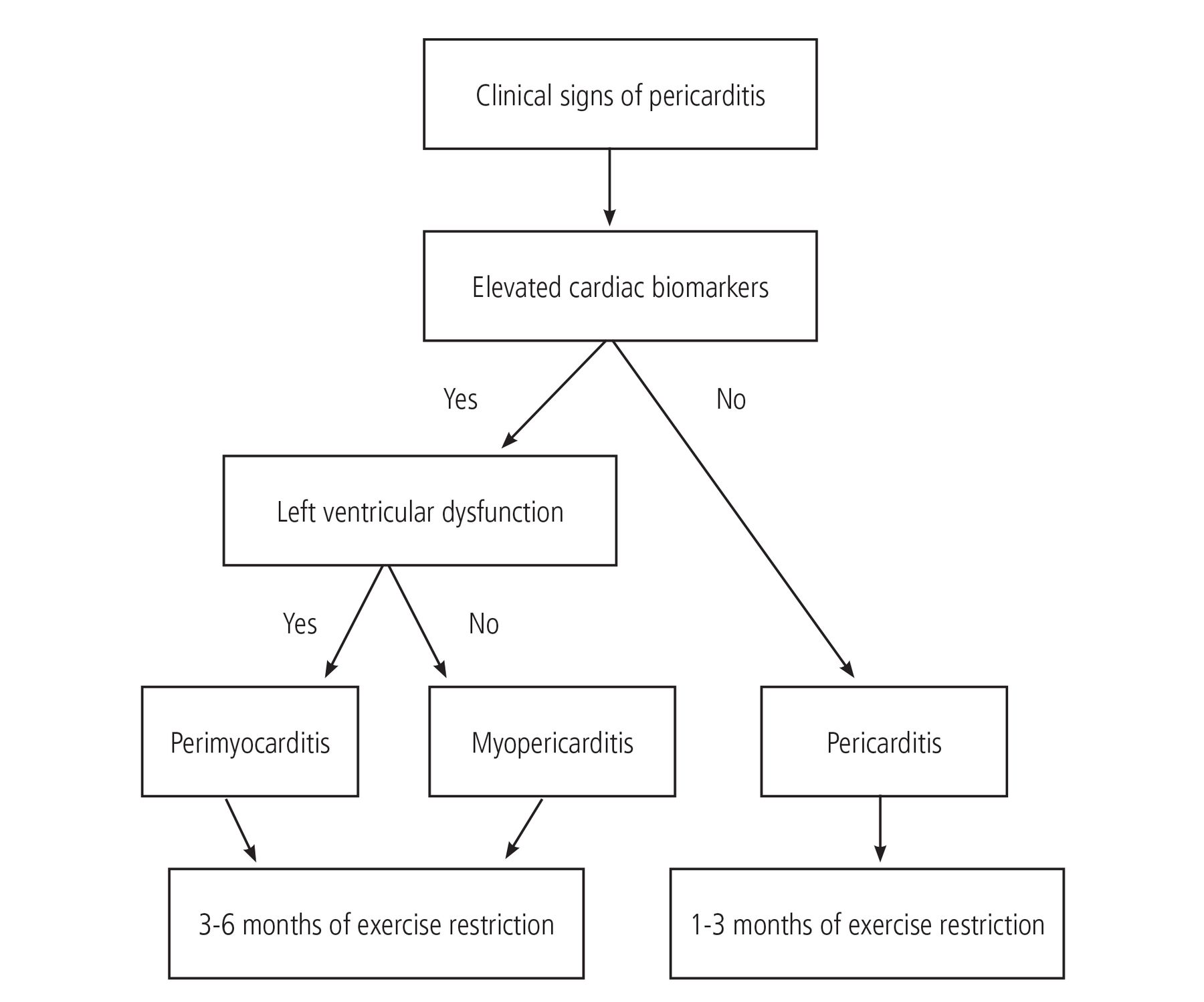
Myopericarditis is a term used to describe predominant pericarditis with concurrent myocardial involvement as defined by the detection of biomarkers of myocardial necrosis in the blood. The relative myocardial involvement can be variable and ranges from isolated inflammation of the pericardium to perimyocarditis, a term used to describe predominant myocardial involvement typically evidenced by new focal or diffuse left ventricular systolic dysfunction. Figure 2 shows a proposed algorithm for determining exercise restriction in patients with these conditions, based on ESC and AHA/ACC recommendations.9,10

Proposed algorithm for exercise restriction in pericarditis with or without myocardial involvement, based on European Society of Cardiology and American Heart Association/American College of Cardiology recommendations. The detection of biomarkers of myocardial injury indicates active myocardial inflammation, which necessitates exercise restriction for 3 to 6 months regardless of left ventricular function.
Any evidence of myocardial involvement is considered a contraindication to exercise regardless of left ventricular systolic function, and professional societies recommend exercise electrocardiography, 24-hour Holter monitoring, and echocardiography no less than 3 to 6 months before resuming exercise.11 The underlying rationale behind this recommendation is the concern that exercise can worsen the inflammatory response with potentially fatal consequences. Indeed, sudden cardiac death without prodromal symptoms has been reported in patients with myocarditis following strenuous activity, and mouse models of myocarditis have shown an association between daily exercise and sudden cardiac death.9,11 Return to exercise can be guided by the use of cardiac MRI to assess for delayed hyperenhancement and myocardial edema on T2-weighted imaging, enabling clinicians to tailor their recommendations for asymptomatic patients who may or may not have active inflammation on imaging. And while there is no clear consensus about the appropriate use of MRI, the ESC guidelines recommend repeating it if edema or delayed hyperenhancement was present on the initial MRI.9,11
Recently, myocarditis has gained increased relevance given its association with COVID-19 infection. However, the overall risk is low. A 2021 study found evidence of cardiac involvement in 0.7% of athletes and 3% in athletes who underwent primary screening MRI.12
THE BOTTOM LINE
Patients with isolated pericarditis should refrain from physical exercise during acute episodes. Athletes should avoid competitive sports for 1 to 3 months after an acute episode, depending on the severity, as part of shared decision-making with their treating clinicians. It is reasonable to resume physical activity if biomarkers (C-reactive protein, erythrocyte sedimentation rate) have normalized, left ventricular function is normal, and there are no residual abnormalities on electrocardiography.
Although specific guidance is lacking for the non-athlete population, we generally recommend patients to limit their physical activity to walking and to limit their active heart rate to 100 beats per minute as long as they are receiving anti-inflammatory medications for pericarditis.
Active myocardial involvement should be considered a contraindication to exercise, given its reported association with sudden cardiac death. There is insufficient evidence to routinely recommend beta-blockers to patients with acute pericarditis. However, it is reasonable therapy in patients in whom beta-blockers can have synergistic effects (eg, those with hypertension or atrial fibrillation) or if their resting heart rate was significantly elevated at baseline. We would aim to decrease the active heart rate to below 100 beats per minute.
BACK TO THE CASE SCENARIO
In the scenario presented earlier, our patient showed delayed hyperenhancement on cardiac MRI. In our experience, these imaging findings can resolve over the course of 3 to 5 years, and anecdotally, exercise can worsen both symptoms and radiologic evidence of disease activity. In light of this, for patients such as this, we would recommend continued exercise restriction if there is ongoing neovascularization or inflammation on MRI. However, acknowledging the health benefits of exercise during a risk-benefit discussion with the patient is always warranted.
Randomized trials are needed to validate the use of imaging to tailor exercise recommendations in acute pericarditis and to determine if there is a role for the use of emerging biologic treatments, such as the anti-interleukin 1 agents anakinra and rilonacept, in enabling a timely return to exercise and competitive sports.
DISCLOSURES
Dr. Klein reports advisor or review panel participation with Cardiol Therapeutics, Kiniksa, and Pfizer; consulting for Kiniksa Pharmaceuticals and Pfizer; and intellectual property rights with Elsevier and Wolters-Kluwer. Dr. Berglund reports no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
Acknowledgment
We acknowledge the contributions of Michael Emery, MD, whose insightful comments have increased the accuracy of this publication.
- Copyright © 2022 The Cleveland Clinic Foundation. All Rights Reserved.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.