


An 85-year-old woman with stage 3 chronic kidney disease presented to our hospital with dyspnea and intermittent mild fever. She had a history of significant odynophagia and dysphagia. In the previous 2 days, the submandibular area had become erythematous and swollen.
The patient’s vital signs were the following:
Glasgow coma Scale 14 out of 15 (ie, responsive)
Blood pressure 107/60 mmHg
Pulse rate 91 beats per minute
Body temperature 36.8°C (98.2°F)
Respiratory rate 20 breaths per minute
Oxygen saturation 95% on room air.
Physical examination revealed the “double tongue” sign on the floor of the mouth (Figure 1), with tender, slightly erythematous swelling under the jaw. She had slight difficulty opening her mouth, but she had no dental caries or cervical lymphadenopathy.
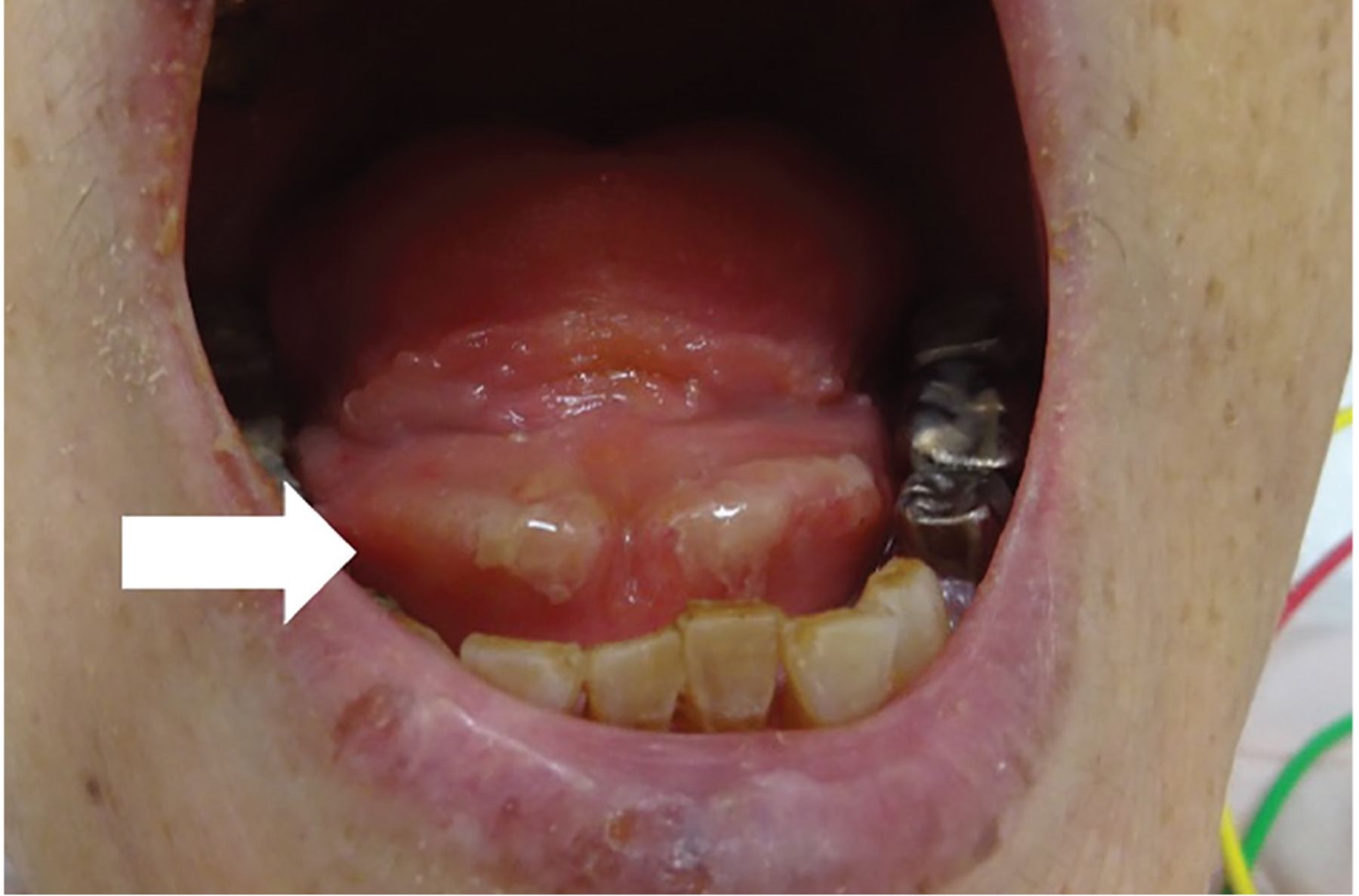
Swelling in the submandibular space pushes the tongue upward, resulting in what resembles a double tongue (arrow).
Laboratory testing on hospital admission revealed the following:
White blood cell count 6.9 × 109/L (reference range 4–11)
Neutrophils 5.7 × 109/L (1.5–8.0)
C-reactive protein 10.8 mg/dL (0–0.3)
Blood urea nitrogen 33.5 mg/dL (8–21)
Creatinine 1.8 mg/dL (0.58–0.96)
Estimated glomerular filtration rate 20.9 mL/min/1.73 m2 (≥ 60).
Laboratory data showed elevated C-reactive protein induced by oral infection, elevated blood urea nitrogen and creatinine levels due to dehydration, and pre-renal acute kidney injury caused by poor oral intake for approximately 2 days.
Computed tomography showed enlarged mylohyoid and geniohyoid muscles, surrounding inflammatory findings, and small gas retentions. There were no findings suggestive of malignant neoplasms of the neck, chest, or abdomen. The patient was diagnosed with Ludwig angina based on the physical examination and features noted on computed tomography.
TREATMENT FOLLOWED BY A SECOND SIGN
An oral surgeon performed incision and drainage, and the patient was prescribed antibiotic therapy with intravenous ampicillin-sulbactam 1.5 g every 12 hours for 14 days in the hospital. Pus culture detected Streptococcus parasanguinis and Bacteroides fragilis.
Her recovery was uneventful, and the double-tongue sign disappeared completely at discharge on day 16 without any complications. However, 3 days later, she returned because her tongue had turned black without other symptoms. She was diagnosed with black hairy tongue caused by antibiotic therapy (Figure 2). Her tongue color returned to normal spontaneously after 14 days.

Black hairy tongue sign. Although there are no subjective symptoms, the tongue’s surface takes on a dark, hairy appearance (arrow) due to abnormal elongation and discoloration of the filiform papillae. The discoloration cannot be removed by brushing or scraping.
TONGUE EXAMINATION KEY TO DIAGNOSIS
This case exemplifies how careful physical examination of the tongue can help achieve a meaningful diagnosis. Ludwig angina is a rare deep-neck infection occurring on the floor of the mouth under the tongue. Prompt treatment is needed to prevent airway obstruction.1,2
In this patient, early recognition of the double-tongue sign resulted in an accurate diagnosis. Although the sensitivity, specificity, and likelihood ratios for Ludwig angina were not quantified, the double-tongue sign is a valuable physical finding, characterized by elevated floor of the oropharynx caused by infection in the submandibular space.1,3
Black hairy tongue
Black hairy tongue is characterized by abnormal elongation and discoloration of the filiform papillae, typically resulting in a carpet-like appearance on the dorsal surface of the tongue.4–6 Black hairy tongue is a benign and painless condition.4–6 However, its etiology and pathophysiology remain vague. Studies suggest that it occurs more commonly in men and is caused by changes in the oral flora due to aging, smoking, alcohol use, poor oral hygiene, and specific antibiotic treatments.5,6 An association with beta-lactam antibiotics has been reported.6 The condition resolves spontaneously when oral hygiene is maintained.
Tongue examination may not be commonly performed often in clinical practice. However, this case shows that understanding characteristic tongue findings helps achieve a meaningful diagnosis and prevent excessive examination and intervention.
DISCLOSURES
The authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
Acknowledgments
The authors would like to thank the staff of the General Medicine Center for their passion for community care and attentive patient care. We would also like to thank the general practitioners in Shimane for their guidance in training young practitioners.
- Copyright © 2022 The Cleveland Clinic Foundation. All Rights Reserved.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.