


Laboratories have been using new (2021) equations to estimate the glomerular filtration rate (GFR). Notably, the new equations differ from earlier ones in that they do not include a coefficient for race. The change was motivated by a desire to reduce racial inequities and improve the health of Black patients. As a result, Black patients are getting lower estimated GFRs than they did with preexisting equations. But will there be unintended consequences? Here, we discuss the history of GFR equations and the potential clinical consequences of the new ones.
HEALTH DISPARITIES IN BLACK AMERICANS
About 37 million Americans—more than 1 in 7—have chronic kidney disease, and a disproportionate number are Black.1 In fact, Black Americans are almost 4 times more likely to have kidney disease than White Americans.1,2
Some of this disparity can be attributed to the prevalence of APOL1 genetic variants that confer risk for kidney disease in people of African ancestry.3 APOL1 risk variants were significantly associated with more severe kidney disease in patients with hypertension-attributed nephropathy, lupus nephritis, sickle cell disease, and human immunodeficiency virus-associated nephropathy.4–7 However, social determinants of health such as economic stability, education, access to food, neighborhood and physical environment, social context, and healthcare systems play a significant and complex role in health outcomes.8 For example, Black patients are less likely to have medical insurance, undergo screening, or be referred to a nephrologist before starting dialysis.9–11
Influenced by America’s social justice movement, medical communities are examining how they may be contributing to healthcare inequities.12 As a result, the widely accepted equations for estimating the GFR, a key number in assessing kidney function, came under scrutiny because they included race as a categorical variable. In August 2020, the National Kidney Foundation (NKF) and the American Society of Nephrology (ASN) formed a task force to evaluate this issue, and 1 year later, they released their recommendations with a new set of equations that do not include race.13
DIRECTLY MEASURING THE GFR: THE GOLD STANDARD, BUT CUMBERSOME
Kidney function is primarily assessed by measuring the rate kidneys can remove solutes from plasma. While renal clearance is the net rate of removal by glomerular filtration plus tubular secretion minus tubular reabsorption, the GFR specifically describes the flow of plasma from the glomerulus into the Bowman space per unit of time and is a surrogate of kidney function. In other words, substances freely filtered by the glomerulus that are not absorbed or secreted by the nephron are equal to GFR. Unfortunately, isolating an endogenously produced substance has been elusive, and therefore we have had to use exogenous substances (inulin, isotopes) or estimate the GFR using endogenous substances (creatinine, cystatin).
The GFR can be directly measured by injecting exogenous substances:
Inulin, a fructose polysaccharide discovered more than 200 years ago in many plant species, is in many ways the ideal marker for directly measuring GFR.14 Infused into the circulation, it is freely filtered by the glomerulus, is not reabsorbed or secreted by the tubules, and is therefore completely excreted. It achieves a steady plasma concentration and is neither produced nor metabolized by the kidneys. Thanks to these properties, inulin’s renal clearance is equal to its GFR. Unfortunately, measuring the inulin GFR is time-intensive and technically challenging, requiring constant infusion of the exogenous substance with frequent urine and serum collections.
Other exogenous substances, including iothalamate compounds containing radioactive (“hot”) or nonradioactive (“cold”) isotopes of iodine, are now considered the gold-standard markers for measuring GFR. Nonradioactive iothalamate is preferred in order to avoid radiation exposure and regulations associated with proper handling and storage of the radioactive material. However, iothalamate GFR measurement is costly, time-consuming, not widely available, and often limited to research.
CREATININE AND CYSTATIN C ARE ENDOGENOUS MARKERS
Creatinine
Creatinine, an endogenous waste product of the breakdown of creatine, is widely used as a marker of kidney function. We can measure 24-hour creatinine clearance in the urine or estimate the GFR using a variety of equations based on the serum concentration of creatinine (see below), avoiding the intensive process of measuring GFR directly. Like inulin, creatinine is freely filtered, but unlike inulin, it is also secreted by the tubules, so creatinine clearance is higher than the actual GFR. The 24-hour urine creatinine clearance is still widely used as an estimate of GFR, but the results may be 10% to 20% higher than the true GFR because of active creatinine secretion by the tubules.15
Moreover, several other processes affect serum and urine creatinine levels (Table 1). These include generation of creatinine, kidney tubular secretion, and reabsorption and vary from person to person, depending on muscle mass, exercise, diet, hydration, and other factors.16 Additionally, creatinine secretion is increased in advanced chronic kidney disease, further limiting its accuracy as a filtration marker.17,18
Non-GFR determinants of creatinine and cystatin C
Black patients on average have higher serum creatinine concentrations at the same measured GFRs compared with non-Black patients.19,20 It has been speculated that this difference is due to differences in biometric variables such as muscle mass. However, Hsu et al21 studied this and found that even after controlling for biometric variables such as height, weight, body mass index, body surface area, fat-free mass, and urinary creatinine excretion, Black patients still had 8.7% higher creatinine concentrations than non-Black patients. This suggested that additional non-GFR determinants have not been accounted for, such as the gastrointestinal creatinine excretion or the rate of creatinine generation per unit of lean muscle.
Cystatin C
Cystatin C, an endogenous protein produced at a constant rate by all nucleated cells, can be used as an alternative or adjunct marker.22 It is freely filtered by the glomerulus and is neither reabsorbed nor secreted by the tubules. We used to think that its serum concentration, unlike that of creatinine, was not affected by sex, age, race, muscle mass, or protein intake.22
However, that may not be entirely true. Knight et al,23 in a study with 8,058 participants, found that older age, male sex, greater weight and height, current cigarette smoking, and higher serum C-reactive protein levels were independently associated with higher cystatin C levels. Manetti et al,24 in a small study, found that cystatin C levels were higher in patients with hyperthyroidism and lower in patients with hypothyroidism (Table 1). Lack of availability, high cost of testing, and lack of insurance reimbursement have limited its use.
SERUM CREATININE-BASED AND CYSTATIN C-BASED EQUATIONS
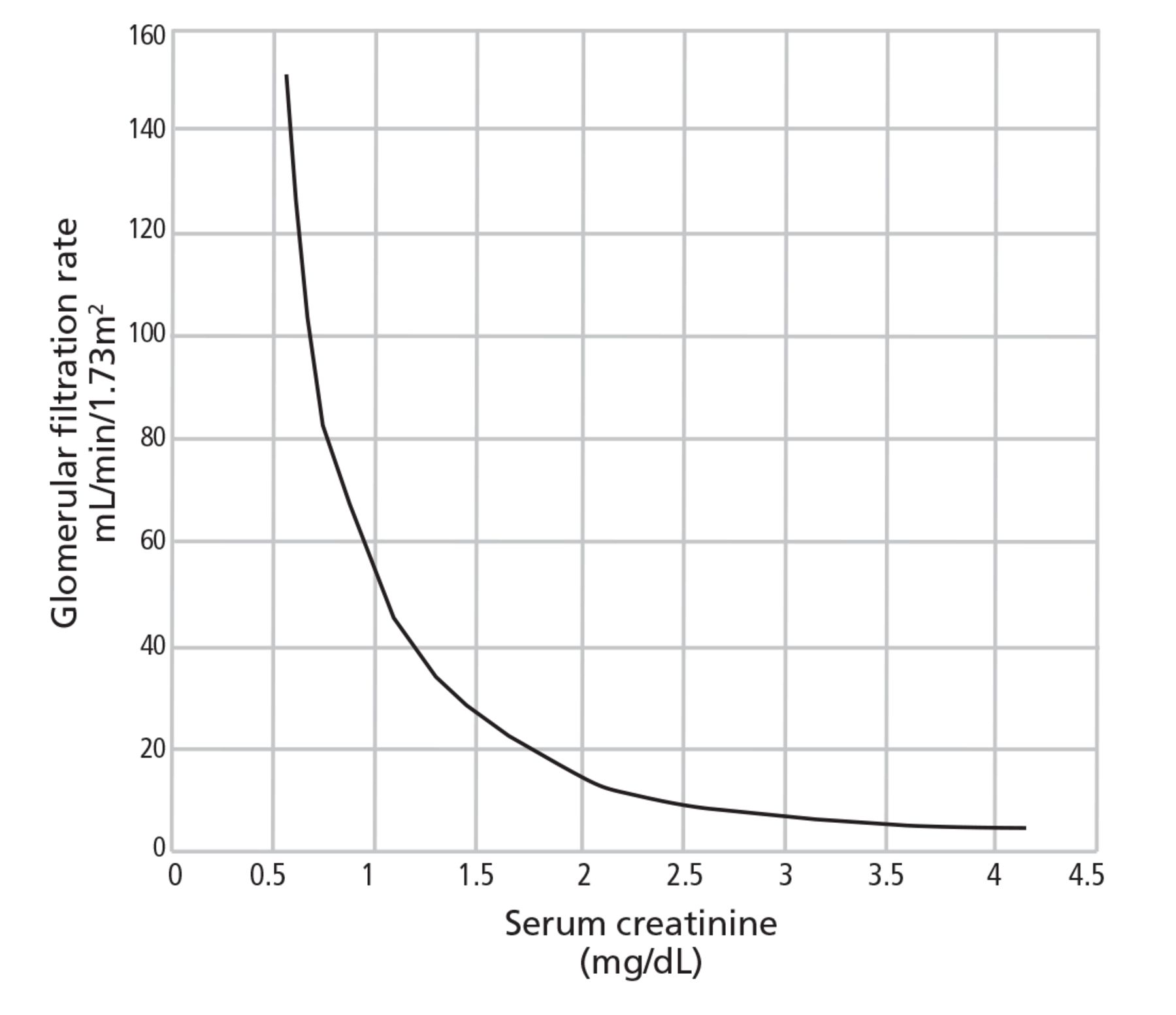
Serum creatinine has a nonlinear relationship to GFR (Figure 1). A small increase of serum creatinine at higher levels of GFR represents a larger decline in kidney function while a larger increase in serum creatinine at lower levels of GFR represents smaller declines in kidney function. Measuring serum creatinine concentration levels in isolation without consideration for other non-GFR determinants such as age, sex, weight, and race to estimate body habitus would be a very crude measure of estimated GFR. Therefore, researchers over the decades have been trying to develop equations that would be able to estimate GFR without having to obtain a burdensome 24-hour urine collection or inject an exogenous substance to better refine this relationship.

Nonlinear relationship of serum creatinine to the glomerular filtration rate.
The 1976 Cockcroft-Gault equation for creatinine clearance
Published in 1976, the Cockcroft-Gault equation was derived from a study in 249 men whose race or ethnicity was not reported.25 Using simple arithmetic, it estimates creatinine clearance (not GFR) based on age, lean body weight, and serum creatinine concentration. It is not adjusted for body surface area, and it presumes that women have 15% less muscle mass. Therefore, for women, the results are multiplied by 0.85. The Cockcroft-Gault equation remained in clinical use until newer equations were released and is still used in drug development and dosing.
The 1999 Modification of Diet in Renal Disease equation
The Modification of Diet in Renal Disease (MDRD) study26 assessed the impact of protein restriction and blood pressure control on the progression of chronic kidney disease. Unfortunately, the benefit of a low-protein diet was small, but the study served as the data source for the development of the future set of GFR equations. Patients had serial blood samples, 24-hour urine collections, and 125I-iothalamate testing to accurately measure the GFR. The post hoc analysis included 1,628 patients from the United States (80.1% White, 12.1% Black, 39.6% female, 6% patients with diabetes, mean age 51, mean weight 79.6 kg, and mean body surface area 1.91 kg/m2).19 One-third of the population was randomized to be the training sample, while the remaining group was the validation sample.
The MDRD investigators developed several equations to estimate the GFR, including a 6-variable equation based on urinary laboratory values, and a 7-variable equation based on expanded serum laboratory values. However, a simplified 4-variable equation based on age, sex, race (Black or non-Black), and serum creatinine concentration became the most widely used.19
Criticisms of the MDRD equations included poor precision (variability between multiple measurements), poor performance if the GFR is higher than 60 mL/min/1.73 m2 (since the parent study enrolled only patients who already had chronic kidney disease), and underrepresentation of Black, Asian, and Latino populations.
The 2009 and 2012 Chronic Kidney Disease Epidemiology Collaboration equations
Results of the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) study—funded by the National Institute of Diabetes and Digestive and Kidney Disease to develop a new equation to improve shortcomings of the MDRD equation—were published in 2009.20 Investigators used 10 studies involving 8,254 patients from North America and Europe and randomized them into an equation-development group (n = 5,504) and an internal validation group (n = 2,750). Another 3,896 patients in 16 other studies served as an external validation group. All patients underwent iothalamate GFR measurement. In the development group, the mean age was 47, 43% were women, 32% were Black, 5% were Hispanic, 1% were Asian, and the mean GFR was 68 mL/min/1.73 m2.20
The 2009 CKD-EPI equation performed better than the MDRD equation in all GFR ranges (including those higher than 60 mL/min/1.73 m2, though precision was still limited at this range), and it was recommended as a replacement for the MDRD equation. Similar to the MDRD equation, the 2009 CKD-EPI creatinine-based equation included age, sex, and a race coefficient (Black or non-Black).20
In 2012, the CKD-EPI investigators published an equation based on cystatin C alone and another one based on cystatin C and creatinine combined.27 Although 40% of the 5,352 participants in the development and internal validation cohort were Black, only 3% were Black in the external validation group. The cystatin C equation did not include a race coefficient, although the combined equation did, and the combined equation outperformed the CKD-EPI equations that used either cystatin C or creatinine alone.27
Major nephrology societies supported the use of the CKD-EPI equations,28 but because few laboratories could measure cystatin C, the equations incorporating this marker were infrequently used.
The 2021 CKD-EPI creatinine equations remove the race coefficient
America’s social justice movement led the nephrology community to reexamine the universal use of estimated GFR equations incorporating a race coefficient. The leading US organizations for patient advocacy (the NKF) and healthcare professionals (the ASN) partnered to create a task force to address this issue. The NKF-ASN task force undertook an exhaustive review of the medical literature and expert and patient-advocacy testimony and concluded that race-based equations should be replaced.13 Included in the review of equations by the NKF-ASN task force were new equations developed by the CKD-EPI workgroup that did not include race coefficients.29
The 2021 CKD-EPI equations were developed using methods similar to those of the 2009 and 2012 CKD-EPI equations and included versions based on creatinine alone, cystatin C alone, and combined creatinine and cystatin C. Black participants made up 31.5% of the development group for the creatinine-based equation and 39.7% of the development group for the combined creatinine-cystatin C equation, which was comparable to their representation in the 2009-2012 CKD-EPI study (40%). Black patients also accounted for 14.3% of the external validation group for the creatinine equation, whereas in the 2009 and 2012 studies they accounted for only 3%.20,27,29
The NKF-ASN task force endorsed the adoption of the 2021 CKD-EPI equations and encouraged clinicians to use the combined creatinine-cystatin C equation.28,29 Many laboratories have incorporated the new equations and report the estimated GFR based on them, and on-line calculators are readily available (https://www.kidney.org/professionals/kdoqi/gfr_calculator).
CLINICAL CONSEQUENCES
The CKD-EPI 2021 equations may have clinical consequences. For example, many drugs that are excreted by the kidneys (eg, sodium-glucose transporter 2 inhibitors, metformin, bisphosphonates, and some antibiotics and chemotherapeutic agents) come with warnings that they should be avoided, given in lower doses, or stopped if the GFR is below certain thresholds. What if a patient’s GFR results, if calculated by different equations, differ enough to affect their medication recommendations?
Will the change help or hurt Black patients?
The Black population is disproportionately affected by chronic kidney disease.1 From a population-health perspective, the change to the 2021 CKD-EPI creatinine equation will shift estimated GFR values lower in Black patients, which will increase the prevalence and severity of CKD staging. Inker et al29 reported that compared with direct measurement, the new creatinine-based equation underestimated the GFR in Black patients by a median of 3.6 mL/min/1.73 m2, and it overestimated it in non-Black patients by a median of 3.9 mL/min/1.73 m2. In contrast, when the race coefficient was omitted from the previous 2009 CKD-EPI creatinine-based equation, it overestimated the GFR for Black patients by 3.7 mL/min/1.73 m2 and underestimated it for non-Black patients by 0.5 mL/min/1.73 m2.20,29
This shift in estimated GFR has potential benefits for Black patients, including earlier detection and treatment of kidney disease to reduce its progression, earlier referral to nephrologists, and more transplant referrals and listings (Table 2). Black patients are more likely than White patients to develop kidney failure but are less likely to be put on transplant waiting lists or receive transplants.11,30 The typical threshold for referral for transplant evaluation is an estimated GFR of 20 mL/min/1.73 m2 or lower, so with the newer, lower estimated GFRs, Black patients may be referred earlier.
Potential patient impacts of the 2021 CKD-EPI equations
Conversely, there may be unintended negative consequences as a result of “renalism,” a term used to describe the therapeutic nihilism that requires patients suffering with kidney disease to have to wait longer for effective interventions.31 More Black patients may be excluded from clinical trials because of a GFR cutoff or a diagnosis of chronic kidney disease or may be excluded as living kidney donors.32 Owing to strict GFR cutoffs, more Black patients may be denied non-kidney solid-organ transplants (lung, heart, intestine, bone marrow) and advanced heart therapies such as ventricular assist devices.
The lowering of GFR in Black patients may make patients ineligible for first-line cancer treatments, antiviral medications, or disease-modifying diabetic drugs such as sodium-glucose cotransporter 2 inhibitors. A retrospective study comparing dosing and eligibility of anticancer drugs in Black patients when comparing estimated GFR equations with and without race reported that 18% of patients would have been given discordant recommendations.33
Additional concerns include inferior drug therapy due to dose reductions in chemotherapy, antivirals (for influenza, hepatitis C, human immunodeficiency virus), and lifesaving antibiotics. Moreover, inferior enhancement of radiographic images due to avoidance or reduction of intravenous contrast (eg, for computed tomography) or intra-arterial contrast (angiography) may lead to inappropriate therapy, delays in diagnosis, and adverse clinical outcomes. Also, the shift in estimated GFR may lead to a new diagnosis (increase in prevalence) or reclassification to a more advanced stage of chronic kidney disease, causing anxiety, as we have seen in patients in our clinics (Table 2). Contrarily, the new equations overestimate GFR in non-Black patients by a median of 3.9 mL/min/1.73 m2.
We suspect that these changes may also have unintended consequences in the non-Black population with respect to nephrology care, drug therapy and dosing, choice of imaging, and eligibility in transplant.
Follow estimated GFR over time
The imprecision of these equations must be considered when interpreting a single creatinine value. We therefore suggest that clinicians follow the general trend in estimated GFR over time.
Precision is measured by the P30—the percent of estimated GFR values that are within 30% of the measured GFR. The 2021 CKD-EPI equations have P30 values of 87% for the creatinine-only equation, 85% for the cystatin C-only equation, and 91% for the creatinine-cystatin C equation.22,29 These values are higher than those of the earlier equations (80.6% for the MDRD equation, 84.1% for the CKD-EPI 2009 equation).19,20
Nevertheless, a patient with an estimated GFR of 50 mL/min/1.73 m2 could have a measured GFR between 35 and 65 mL/min/1.73 m2. With this limited precision, it is possible for these estimated GFR equations to assign patients into an inaccurate stage of chronic kidney disease. In fact, the new equations have only slightly greater than 60% accuracy at assigning chronic kidney disease stage.29 Therefore, several measurements over time should be obtained to better access the accuracy of GFR. Additional research is needed for better markers to improve the precision and overall assessment of kidney health.
TAKE-HOME POINTS
Recently, calls to reevaluate the basis for using a race coefficient in GFR-estimating questions prompted a reevaluation of GFR estimation.
Currently, creatinine is the most widely used biomarker to estimate GFR, but serum creatinine levels are influenced by factors other than GFR.
Over the last several decades, a coefficient for race has been used in GFR equations in an attempt to account for these non-GFR determinants. However, this practice introduces a bias between Black and non-Black patients in GFR estimation.
The new CKD-EPI 2021 equations were developed without a race coefficient and perform with improved precision compared with previous equations. The NKF-ASN task force called for the immediate implementation of these equations and an increased focus on using cystatin C to assist with GFR estimation.
The change in these GFR-estimating equations will have important clinical impacts on chronic kidney disease prevalence estimates, access to transplant, and drug dosing for individual patients.
These creatinine-based and cystatin C-based equations have significant limitations in their precision. We believe that additional research and focus is needed to improve the assessment of kidney function, given the increasing prevalence of kidney disease.34
DISCLOSURES
Dr. Mehdi has disclosed teaching and speaking for AstraZeneca and serving as advisor or review panel participant for Fresenius. Dr. Nakhoul has disclosed consulting for Amgen, ChemoCentryx, GSK, and Otsuka Pharmaceuticals; and teaching and speaking for ChemoCentryx. Dr. Taliercio has disclosed serving as advisor or review panel participant for Otsuka America Pharmaceuticals, GSK, Boehringer Ingelheim. The other authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
- Copyright © 2023 The Cleveland Clinic Foundation. All Rights Reserved.
REFERENCES
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.
Commentary