


ABSTRACT
For patients with decompensated cirrhosis, health maintenance is critical to improve survival rates and prevent adverse outcomes. We review the primary care management of cirrhosis and its complications, such as esophageal varices, hepatocellular carcinoma, and chemical or medication exposures. We also highlight specific immunizations and lifestyle modifications to prevent decompensation, and we summarize current screening guidelines.
The 2-year mortality rate for decompensated cirrhosis is as high as 26.4%, and the 5-year rate is as high as 85%.
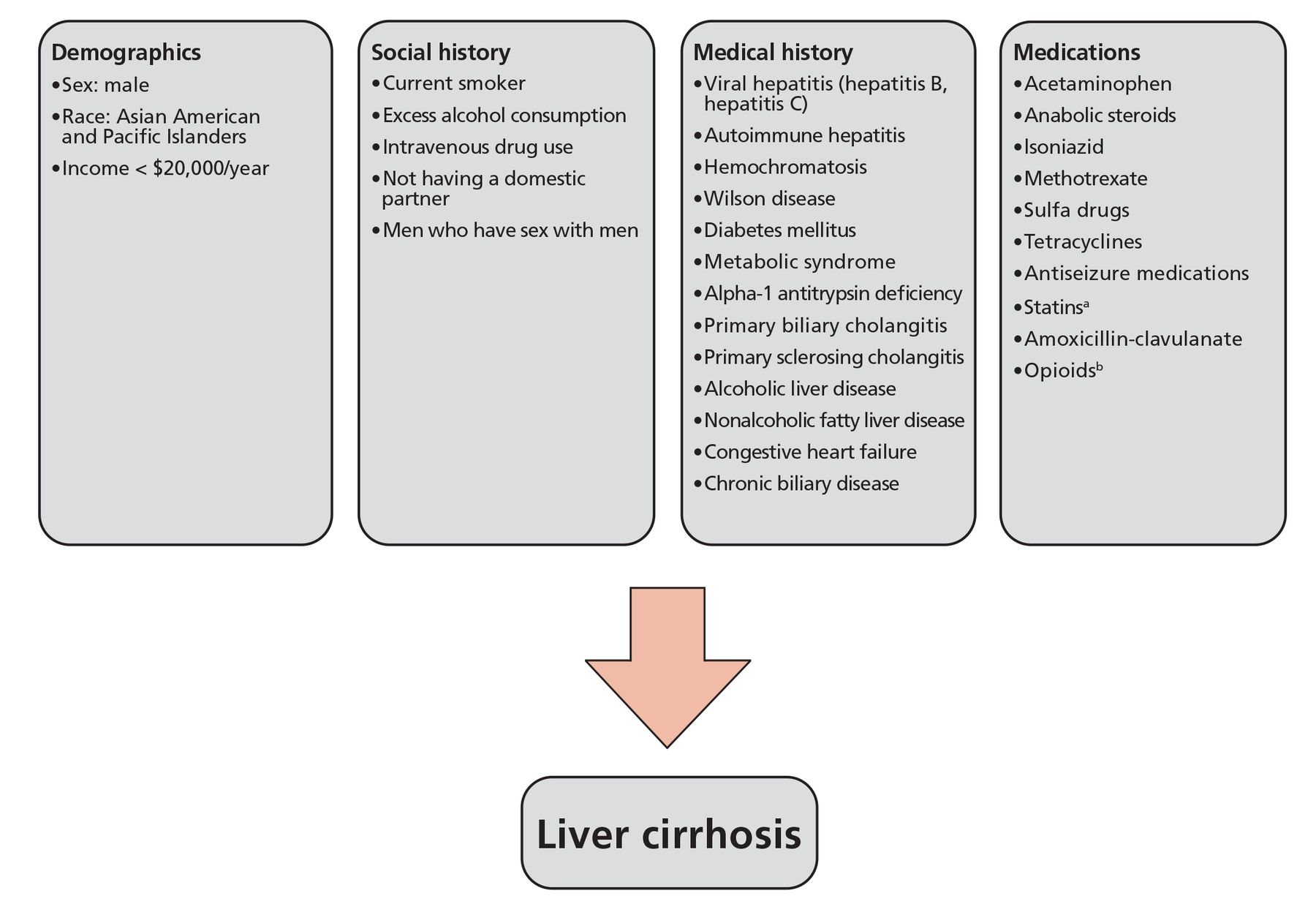
Factors independently associated with cirrhosis include diabetes, alcohol abuse, hepatitis B virus, hepatitis C virus, men who have sex with men, and older age.
Primary care clinicians are often the first to diagnose and manage patients with liver cirrhosis.
Cirrhosis is the 12th most common cause of death worldwide and the eighth highest cost-to-treat illness worldwide.1,2 In the United States, the prevalence of cirrhosis is 0.27%, corresponding to approximately 633,323 adults.3 There are few comprehensive resources available that outline primary care management of patients with liver cirrhosis. Hence, this review discusses management in the primary care setting, screening for complications, immunizations, exposure reduction, and lifestyle modifications in patients with liver cirrhosis.
DIAGNOSIS
Cirrhosis of the liver is both a pathologic and clinical diagnosis. Pathologically, it is defined as the histologic disruption of the architecture of the liver owing to fibrous replacement of normal liver tissue, and leads to portal hypertension and end-stage liver disease that is typically irreversible in advanced stages.4,5
Clinically, a patient is usually diagnosed when presenting with decompensation, or clinical decline, showing evidence of variceal bleeding, renal failure, spontaneous bacterial peritonitis, hepatic encephalopathy, or ascites.4 It is essential to recognize and diagnose decompensated cirrhosis early, as it has a high mortality rate without transplant, with a 2-year mortality rate as high as 26.4%, and 5-year mortality as high as 85%.3,4
DIAGNOSTIC TESTING
Cirrhosis is often clinically asymptomatic and insidious in the initial stages. It has been reported that up to 20% of patients with hepatitis C virus infection may develop cirrhosis before clinical signs are present.4 As many as 10% of patients with nonalcoholic steatohepatitis may develop cirrhosis with no clinical signs or symptoms.4 In asymptomatic patients, incidental detection of elevated aminotransferases or imaging suspicious for hepatic disease should stimulate further workup to determine the likelihood of liver disease.5 This includes a thorough history to screen for cirrhosis risk factors, as described in Figure 1.3–6

In addition, laboratory tests to evaluate for liver injury should be ordered for patients with a high suspicion of liver disease.5 These tests include a complete blood cell count (platelet count < 150 × 109/L), aspartate aminotransferase, alanine aminotransferase, albumin, alkaline phosphatase, gamma-glutamyl transferase, total bilirubin, prothrombin time, and international normalized ratio (INR) (Table 1).4,5
Initial laboratory tests when evaluating for chronic liver disease
Once the presence of liver disease is evident, patients should undergo a complete evaluation to determine disease course and potential etiology, as these are essential prognostically. For instance, patients with hepatitis C virus-induced cirrhosis have a lower annual decompensation rate than those with hepatitis B virus, ie, 4% compared with 10%.4 Patients with alcohol-induced liver cirrhosis have higher decompensation rates than patients with other forms of cirrhosis.7
Interpreting results of aminotransferase testing
The American College of Gastroenterology recommends that if aminotransferases are elevated during routine testing, additional laboratory testing is required, including hepatitis B surface antigen, hepatitis B core antibody, hepatitis B surface antibody, hepatitis C virus antibodies, and iron studies (Table 2).4,6 Because alanine aminotransferase is found in cells other than hepatocytes, testing creatine kinase and determining the ratio of creatine kinase to alanine aminotransferase is important.
Diagnostic tests for evaluation of the etiology of liver cirrhosis
Age also plays a key role in the interpretation of elevated aminotransferases. For example, in a young individual with significantly elevated aminotransferases, genetic disorders such as Wilson disease or hemochromatosis should be on the list of differential diagnoses and require additional workup. Furthermore, abdominal ultrasonography, with particular focus on the right upper quadrant (liver), should also be ordered to rule out an acute or structural disease process.
If the laboratory tests are unremarkable and aminotransferases remain elevated after a period of 3 to 6 months, further investigation with antinuclear antibody and antismooth-muscle antibody, gamma-globulin, ceruloplasmin, and alpha-1 antitrypsin phenotype should be ordered to evaluate for additional causes.6
Biopsy and noninvasive testing
The diagnostic test for liver cirrhosis is biopsy.4,5 Noninvasive testing modalities to evaluate for liver cirrhosis include vibration-controlled transient elastography and magnetic resonance elastography. It should be noted that noninvasive measures, especially transient elastography, are replacing biopsy as the preferred tests for fibrosis staging.5 Transient elastography determines liver stiffness by measuring the velocity of low-frequency ultrasound waves traveling through the liver.5 It is both sensitive and specific to establish the diagnosis of liver cirrhosis.8 In fact, guidelines from the National Institute for Health and Care Excellence (NICE) recommend that liver biopsy be performed if elastography is unsuitable or inconclusive.9
SCORING SYSTEMS FOR THE DEGREE OF LIVER INJURY
Several classification systems aim to predict the degree of liver injury and the prognosis. The Child-Pugh-Turcotte scoring system (Table 3) is among the most widely used, with an excellent predictive value that uses albumin, total bilirubin, INR, and degree of ascites and encephalopathy to assess the severity of cirrhosis.10,11 Additionally, NICE recommends using the Model for End-Stage Liver Disease (MELD) score every 6 months, as it predicts 3-month mortality in patients with end-stage liver disease.9,12 The MELD score, initially created to predict the survival of patients undergoing transjugular intrahepatic portosystemic shunts, uses creatinine, bilirubin, and INR.12
Child-Pugh-Turcotte score
The Child-Pugh-Turcotte and MELD scoring systems are commonly used together in clinical practice because studies of the discriminative ability of Child-Pugh-Turcotte vs that of MELD have had variable results.12 A systematic review of observational studies found that Child-Pugh-Turcotte had a higher sensitivity than MELD in predicting outcomes in patients with acute-on-chronic liver failure (0.81 vs 0.63), but MELD had higher sensitivity (0.77 vs 0.51).12 However, the MELD score was found to have better discriminative ability to predict outcomes in intensive care unit patients. Moreover, in patients undergoing surgery, the Child-Pugh-Turcotte had higher specificity (0.82 vs 0.71).12 It should be noted that no significant difference was found when comparing sensitivity and specificity in predicting 12-month mortality between the 2 scores. For this reason, we recommend using the clinical context to decide which classification system to use in clinical practice.
ESOPHAGEAL VARICES: SCREENING AND PREVENTION
One of the most important and fatal complications of liver cirrhosis is the rupture of gastroesophageal varices secondary to portal hypertension.13–15 Studies have demonstrated cumulative incidence of the development of esophageal varices in patients with cirrhosis to be 5% at 1 year and 28% at 3 years, progression was 12% at 1 year and 31% at 3 years, and the 2-year risk of bleeding was 12% vs 2% with small varices vs none at baseline.13
Esophageal varices can be diagnosed with esophagogastroduodenoscopy, which is usually recommended in high-risk varices.14,15 Initial screening may be performed by platelet count and liver elastography (Table 4).9,16–18 Patients with compensated cirrhosis who are not candidates for nonselective beta-blocker for prevention of decompensation should undergo esophagogastroduodenoscopy for variceal screening if liver stiffness measurement is less than 20 kPa or the platelet count is less than 150 × 109/L.15 Patients avoiding screening endoscopy can be followed every year by repetition of transient elastography and platelet count. If liver stiffness measurement increases (< 20 kPa) or platelet count declines (< 150 × 109/L), these patients should undergo screening endoscopy.15
Screening recommendations for patients with liver cirrhosis
For patients with no varices or small varices, controlling the underlying cause and managing the complications of cirrhosis effectively prevents the progression of variceal rupture.14 For example, keeping hepatitis viral load low to prevent worsening fibrosis can prevent worsening variceal engorgement. For patients with large varices, nonselective beta-blocker therapy (carvedilol [preferred], nadolol, or propranolol) dramatically reduces risk of variceal bleeding from 30% to 14%.14,19 For those with medium or large varices, NICE recommends endoscopic variceal band ligation to prevent bleeding.9
HEPATOCELLULAR CARCINOMA
One of the most feared complications of cirrhosis is the development of hepatocellular carcinoma, with an annual incidence as high as 8% in patients with liver cirrhosis.20,21 Risk factors in the development of hepatocellular carcinoma include hepatitis B or C virus infection, aflatoxin exposure, alcohol use, tobacco use, and obesity.22 The risk of developing hepatocellular carcinoma is also higher in patients age 55 and older, patients with 75% or less prothrombin activity, and patients with platelet counts below 75 × 109/L.22
The role of imaging
Owing to relatively low cost, ultrasonography is most commonly used as an initial imaging tool compared with computed tomography (CT) or magnetic resonance imaging (MRI) for screening of hepatocellular carcinoma. As such, current guidelines from NICE and the American Association for the Study of Liver Diseases recommend that patients with cirrhosis undergo routine imaging every 6 months to screen for hepatocellular carcinoma.9,21 This recommendation is based on low-quality evidence from several studies suggesting a benefit of at least 3 months of life-years gained in patients undergoing surveillance with ultrasonography every 6 months.21
CT and MRI are alternate options as they have a higher sensitivity and specificity than ultrasonog-raphy.16 However, they have limited availability and higher associated costs. Therefore, only in select cases where ultrasonography results are challenging to interpret (patients with morbid obesity, those with fatty liver, or those with advanced liver disease), CT and MRI can be considered.23 Ultrasonography only shows a sensitivity of 47% when detecting early-stage hepatocellular carcinoma in patients with cirrhosis, so a negative imaging result should not dismiss high clinical suspicion or replace serial ultrasonography.24 If ultrasonography detects a mass under 10 mm, repeat ultrasonography is warranted in 3 months to monitor the growth.24 For lesions greater than 10 mm, further imaging with CT or MRI and the risks and benefits of biopsy should be discussed with a specialist.19 However, it should be noted that biopsy of suspected hepatocellular carcinoma is generally avoided for fear of tumor seeding, thereby making localized disease more widespread.
Use of tumor markers
In addition to imaging, tumor markers such as serum alpha-fetoprotein can also be used to screen for hepatocellular carcinoma.19,25 Generally, alpha-fetoprotein levels greater than 20 ng/mL are considered a positive test. Patients with evidence of a 10-mm or larger lesion and a serum alpha-fetoprotein level greater than 20 ng/mL should undergo diagnostic testing with a contrast-enhanced multiphase CT or MRI.19 In addition, clinicians should remember that although elevated alpha-fetoprotein levels are expected in patients with liver cirrhosis, even in the absence of hepatocellular carcinoma, alpha-fetoprotein levels greater than 400 ng/mL warrant additional workup to rule out hepatocellular carcinoma.25
Decreasing the risk of hepatocellular carcinoma
Chemopreventive strategies and dietary agents have been proposed to decrease the risk and delay the onset of hepatocellular carcinoma.26 Universal immunization and antiviral therapy for patients with hepatitis B and hepatitis C virus infection reduce the risk of hepatocellular carcinoma development.
Aspirin and statins have antineoplastic and anti-inflammatory properties that may have a protective effect on hepatocellular carcinoma development.27 However, there is still a substantial lack of data on aspirin and statin use in hepatocellular carcinoma, and additional studies are needed to determine benefit in this patient subset.
SCREEN FOR HEPATOTOXIC MEDICATIONS
Although no specific recommendations have been published regarding the use of medications in patients with cirrhosis, it can be generalized that hepatotoxic medications should be prescribed with caution.28 A list of drugs that should be avoided or prescribed with caution is summarized in Table 5.5,29–32
Medications to use cautiously in patients with liver cirrhosis
OFFICE EVALUATION OF HEPATIC ENCEPHALOPATHY
Hepatic encephalopathy refers to cognitive dysfunction resulting from liver disease that manifests as a broad spectrum of neurocognitive symptoms ranging from subclinical abnormalities to coma.33 Hepatic encephalopathy is a major cause of morbidity, mortality, and healthcare spending in the United States.34 Primary care clinicians can play a key role in recognizing the signs and symptoms of hepatic encephalopathy and initiating early treatment before the need for hospitalization.
The clinical presentation of hepatic encephalopathy varies widely. Patients with minimal disease may have few symptoms, such as subtle personality changes or abnormal psychometric tests.18,33 Testing of patients for minimal hepatic encephalopathy or covert hepatic encephalopathy is important because these conditions are reported to be as high as 50% in patients with chronic liver disease.35 Early diagnosis of minimal hepatic encephalopathy can help predict the likelihood of the development of overt hepatic encephalopathy and can allow for the initiation of treatment and lifestyle modifications to slow or prevent disease progression.
The International Society for Hepatic Encephalopathy and Nitrogen Metabolism has suggested that patients undergo testing using two separate psychometric tests, as each test may evaluate different components of cognitive functioning, and impairment in patients with minimal hepatic encephalopathy may vary from patient to patient.35 Some available testing strategies include the Animal Naming Test, Psychometric Hepatic Encephalopathy Score, Critical Flicker Frequency test, Continuous Reaction Time test, Inhibitory Control Test, Stroop Test, Trail Making Test, the computerized Scan test, and examination using electroencephalography.35 Some of these tests are time-consuming and require specialized equipment and staff training. Hence, they cannot be performed in a busy outpatient primary care setting. However, the Animal Naming Test has a high degree of accuracy, can be administered quickly, and is feasible in an outpatient setting.
Symptoms of overt hepatic encephalopathy are more apparent and include personality changes, irritability, disinhibition, sleep disturbances, sleep cycle alteration or excessive daytime sleepiness, disorientation, inappropriate behavior, confusion, stupor, and coma.35 Additionally, motor symptoms such as hypertonia and hyperreflexia, in addition to extrapyramidal signs such as muscular rigidity, bradykinesia, hypokinesia, slowed speech, Parkinson-like tremor, and dyskinesia are expected.35 Finally, asterixis is usually seen in patients in early to middle stages of the disease.
The diagnosis of overt hepatic encephalopathy is primarily based on findings of a clinical examination and is made only after excluding other causes of brain dysfunction.17 A key test to determine the clinical severity of hepatic encephalopathy is the West Haven criteria, which help stratify patients into the following grades based on clinical presentation and neuropsychiatric state:
Unimpaired: normal, no subclinical or clinical impairment of mental state
Covert: minimal encephalopathy and lack of disorientation and asterixis (ie, grade I)
Overt (grades II–IV).35
It should be noted that high blood ammonia levels are not diagnostic for hepatic encephalopathy, nor are they helpful in determining prognosis or staging.17,35 Hence, they should not be used to follow hepatic encephalopathy.
IMMUNIZATION AND EXPOSURE REDUCTION
For healthcare clinicians, it is essential to ensure that patients with liver cirrhosis receive proper vaccinations to ensure health.36 According to the US Centers for Disease Control and Prevention guidelines, patients with chronic liver disease should receive the following vaccinations: influenza vaccine annually, hepatitis A and hepatitis B vaccine, herpes zoster vaccine, Tdap vaccine, and 1 dose of pneumococcal conjugate vaccine (PCV15, PCV20) if age 65 or older, or age 19 to 64 after a diagnosis of liver disease is established.36 If PCV15 is used, it should be followed by a dose of pneumococcal polysaccharide vaccine 23.
LIFESTYLE MODIFICATIONS
Diet and exercise
A Mediterranean diet and avoidance of red and processed meat, high-fructose corn syrup, and foods high in saturated fats have shown the most promising results in reducing the risk of nonalcoholic fatty liver disease (NAFLD) and preventing progression to nonalcoholic steatohepatitis and eventual cirrhosis.37 In a randomized clinical trial, patients with NAFLD who followed a low-glycemic-index Mediterranean diet with no caloric restrictions for 6 months were found to have reductions in their NAFLD score as determined by liver ultrasonography.38 Furthermore, patients who adhered to a Mediterranean diet showed more significant weight loss than a control group.37,38 Those who adhered to a Mediterranean diet and exercised at least 30 minutes a day (eg, aerobic exercise consisting of fast walking, slow or fast running, dancing) showed not only more significant weight loss, but also improvement in elevated aminotransferases and liver stiffness than in controls.37,38
In patients with cirrhosis, hyperammonemia, muscle autophagy, and low levels of branched-chain amino acids have been hypothesized to be the cause of sarcopenia.39 To prevent or reverse this catabolic state, high-protein diets can help maintain nitrogen levels needed to avoid sarcopenia.
The European Association for the Study of the Liver clinical practice guidelines recommend 1.2 to 1.5 g/kg/day of protein and at least 35 kcal/kg/day of calorie intake for patients with hepatic encephalopathy.40 Furthermore, the European Association for the Study of the Liver recommends avoiding fasting for longer than 6 hours, putting the patient at high risk of entering a catabolic state during the night. Meals should therefore be given in small, frequent amounts, with late-night snacks containing high amounts of carbohydrates and proteins to improve nitrogen balance throughout the night.39
Sodium and fluid restriction
For patients with liver cirrhosis and ascites, sodium restriction is a mainstay in managing symptoms.40 Sodium intake should be limited to less than 2 g/day or 88 mmol/day, as it has been noted that the development of ascites is secondary to renal retention of sodium.40 Patients can generally achieve this recommendation by avoiding added salt and pre-prepared meals that are often high in sodium.40 However, extreme restriction less than 2 g/day is not recommended as it can reduce food intake, worsening coexisting malnutrition and the catabolic state common in patients with cirrhosis.40 In addition, for patients taking diuretics, a marked reduction in sodium intake can exacerbate hyponatremia.41
Fluid restriction of 1 to 1.5 L/day should be reserved for patients with clinical hypervolemia and severe hyponatremia (serum sodium < 125 mmol/L).41 Fluid restriction is most effective when fluid intake is less than the urinary volume. However, urinary volume is usually low in patients with cirrhosis, so adequate fluid restriction is nearly impossible to achieve and is therefore not recommended.41
TAKE-HOME MESSAGES
The careful evaluation of patients with cirrhosis in the primary care setting includes identifying risk factors that can lead to decompensation, attention to proper immunization and exposure reduction, and counseling on lifestyle modifications, with a low threshold for referral to appropriate specialists. Primary care clinicians can play a key role in reducing the morbidity and mortality of liver cirrhosis, improving patient outcomes and survival rates.
DISCLOSURES
The authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
Acknowledgments
We thank Jeffrey Jackson, MD, MPH, from the Medical College of Wisconsin for critically reading and encouraging us during the preparation of this manuscript.
- Copyright © 2023 The Cleveland Clinic Foundation. All Rights Reserved.
REFERENCES
In this issue




{kind=link}
Jump to section
- Article
- ABSTRACT
- DIAGNOSIS
- DIAGNOSTIC TESTING
- SCORING SYSTEMS FOR THE DEGREE OF LIVER INJURY
- ESOPHAGEAL VARICES: SCREENING AND PREVENTION
- HEPATOCELLULAR CARCINOMA
- SCREEN FOR HEPATOTOXIC MEDICATIONS
- OFFICE EVALUATION OF HEPATIC ENCEPHALOPATHY
- IMMUNIZATION AND EXPOSURE REDUCTION
- LIFESTYLE MODIFICATIONS
- TAKE-HOME MESSAGES
- DISCLOSURES
- Acknowledgments
- REFERENCES
- Figures & Data
- Info & Metrics
Related Articles
Cited By...
- No citing articles found.