


ABSTRACT
Cutaneous manifestations, a well-known effect of viral infections, are beginning to be reported in patients with COVID-19 disease. These manifestations most often are morbilliform rash, urticaria, vesicular eruptions, acral lesions, and livedoid eruptions. Some of these cutaneous manifestations arise before the signs and symptoms more commonly associated with COVID-19, suggesting that they could be presenting signs of COVID-19.
INTRODUCTION
Cutaneous manifestations are well known to occur in the setting of viral illnesses, and occasionally these manifestations have diagnostic or prognostic value. With COVID-19, although we are at a relatively early point in the pandemic, cutaneous manifestations in infected patients are beginning to emerge from around the world. In this article, we describe some of the current cutaneous abnormalities observed in patients with COVID-19.
MORBILLIFORM RASH
A morbilliform rash is a common morphology seen with viral exanthems. In an Italian cohort of 18 patients with COVID-19 who developed cutaneous abnormalities, 14 of them (77.8%) had an erythematous/ morbilliform eruption.1 Several Spanish groups have also reported COVID-19 patients who developed nonspecific maculopapular/morbilliform eruptions, with at least 1 case also accompanied by focal purpura.2,3
URTICARIA
Urticarial eruptions are emerging as a potential COVID-19 skin manifestation. In the Italian cohort study described above, 3 of the 18 patients with cuta neous eruptions developed widespread urticarial.1 Physicians from Spain reported a 32-year-old woman with a pruritic urticarial eruption in the setting of COVID-19 that occurred several days after starting hydroxychloroquine and azithromycin and which symptomatically responded to antihistamine therapy.2 Finally, a 27-year-old woman in France developed an urticarial eruption along with odynophagia and diffuse arthralgias 48 hours before onset of fever and chills and COVID-19 diagnosis.4 The temporal onset of urticaria before the more well-known symptoms develop raises the possibility that cutaneous eruptions can be a presenting sign of COVID-19.
VESICULAR ERUPTIONS
Varicella-like vesicular eruptions have been described in COVID-19 patients.5,6 Italian researchers described 22 patients with scattered or diffuse varicella-like vesiculopapular eruptions, representing the largest cohort of COVID-19 patients published thus far with similar cutaneous eruptions.6 The authors concluded that these vesiculopapular eruptions were specific to COVID-19, stressing that no patient in their cohort had been exposed to new medications in the 15 days before eruption onset. Median latency time from COVID-19 systemic symptoms to the rash was 3 days, and the median duration of skin manifestations was 8 days. There was no significant association with the severity of COVID-19 disease and the cutaneous eruption. Fewer than 50% of the eruptions were biopsied, but histopathologic features included interface dermatitis with apoptotic keratinocytes, which is similar to findings in many other viral exanthems.
ACRAL LESIONS (“COVID TOES”)
Acral cutaneous lesions have been reported in patients with COVID-19, and they may take different forms. In a report from Kuwait, 2 asymptomatic patients diagnosed with COVID-19 were described as having perniosis-like acral lesions.7 Alternatively, Spanish researchers reported a 28-year-old woman who developed pruritic erythematous papules specifically on her heels.8
LIVEDOID ERUPTIONS
There have been several reported cases of livedo reticularis-like eruptions in US patients with COVID-19.9,10 The livedoid changes may be unilateral in nature. Of potential importance is that these lesions are thought to be secondary to COVID-19-induced thrombotic vasculopathy. If livedoid eruptions are eventually noted to occur in COVID-19 patients with systemic thrombotic vasculopathy, it will be particularly important to recognize these eruptions clinically, and they may have prognostic value in these patients. At least 1 of the described patients with a livedoid eruption was hospitalized and required supplemental oxygen, but his or her eventual outcome is unknown.9
OTHER CUTANEOUS ERUPTIONS
There have been several reports of COVID-19 patients presenting with unusual cutaneous eruptions. For example, a 64-year-old woman in France with COVID-19 who developed a rash consistent with Symmetrical Drug-Related Intertriginous and Flexural Exanthema (SDRIFE) 4 days after she became febrile was recently reported.5 Although SDRIFE is usually a medication-induced eruption, the authors were unable to attribute this case to a culprit medication. Additionally, Joob and colleagues11 reported a petechial rash in a COVID-19 patient that mimicked the cutaneous eruption seen in Dengue fever.
OUR EXPERIENCE
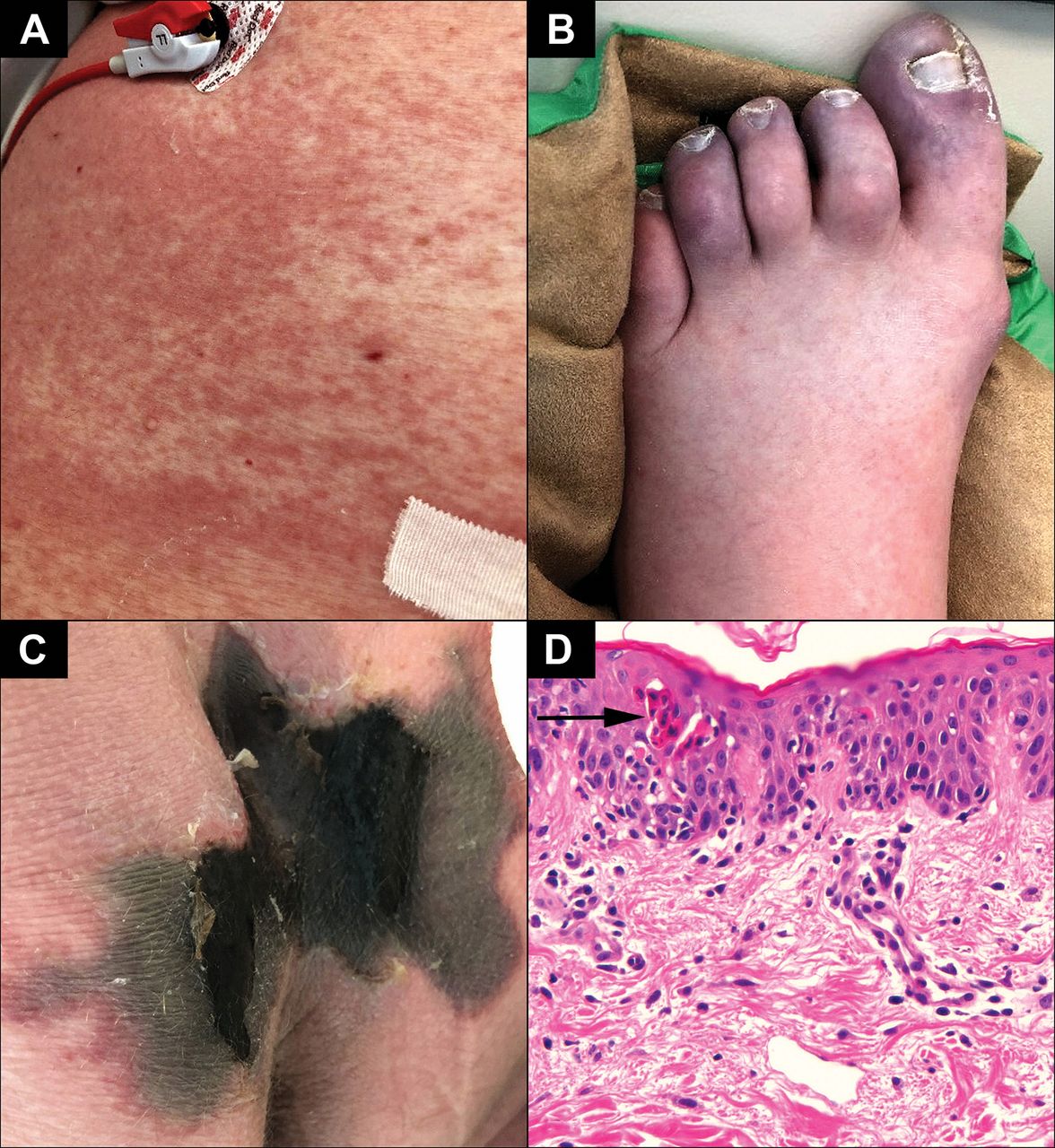
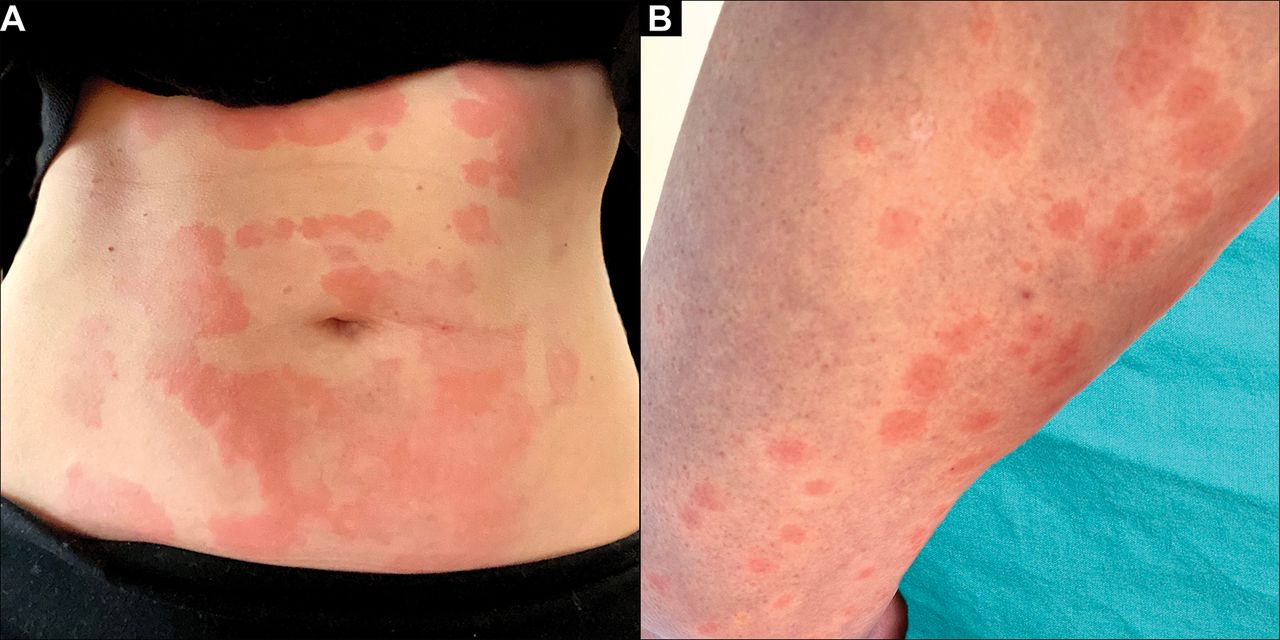
At Cleveland Clinic, patients we have seen with cutaneous eruptions while suffering from COVID-19 have had cutaneous morphologies that align with those reported above. Importantly, an individual patient may present with multiple simultaneous cutaneous abnormalities that differ in morphology. Recently, we treated a 68-year-old critically ill man with COVID-19 who had a morbilliform rash on his trunk (Figure 1A), acral purpura reminiscent of perniosis (Figure 1B), and an ulcerated, purpuric plaque with retiform/ livedoid borders on his buttocks (Figure 1C). A biopsy (Figure 1D) from the abdomen shows groups of apoptotic keratinocytes in the epidermis, suggestive of a viral exanthema (Figure 1D). A biopsy from the buttocks (not shown) showed features consistent with a thrombotic vasculopathy. We have also seen a 39-year-old woman who developed an urticarial rash (Figure 2) just prior to onset of fever and then COVID-19 diagnosis, further suggesting that this may be a presenting sign of the disease. Importantly, the patient had taken no new medications prior to urticarial onset, supporting the concept that it was related to SARS-CoV-2 infection.

Cutaneous abnormalities on a 68-year-old critically ill man with COVID-19 including a morbilliform rash on the abdomen (A), acral purpura (B), and plaque-like cutaneous purpura and necrosis with livedoid borders (C). A biopsy from the abdomen (D) shows groups of apoptotic keratinocytes in the epidermis (arrow), suggestive of a viral exanthem.
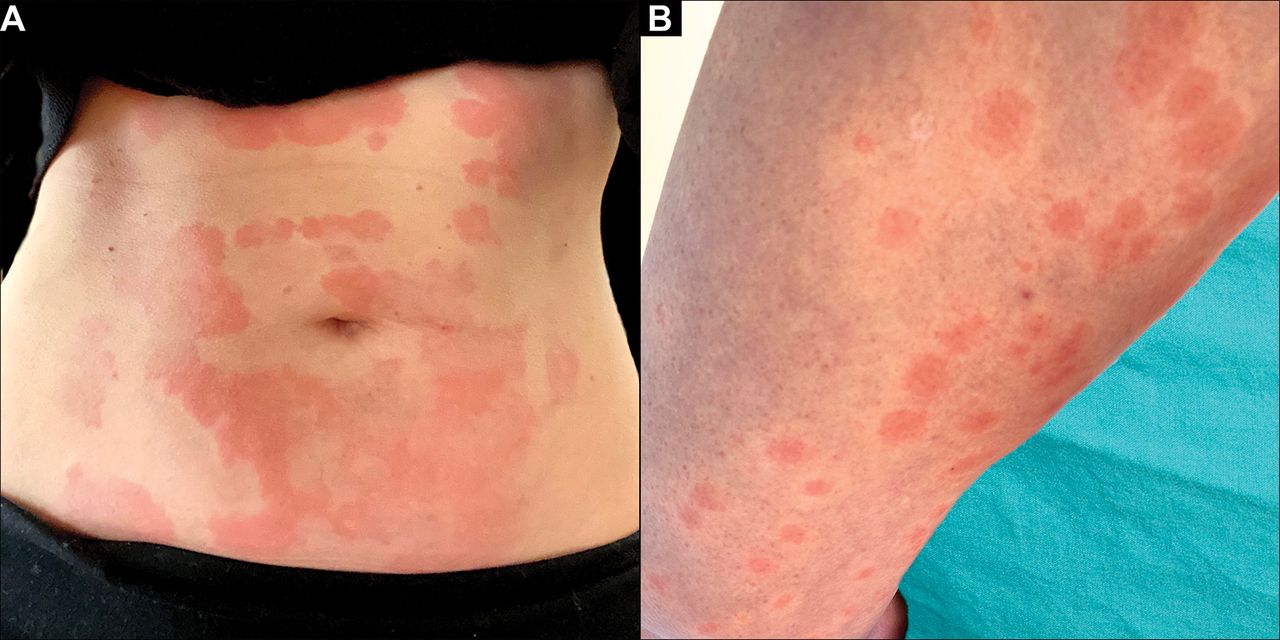
A 39-year-old woman with urticarial involving her (A) trunk, (B) thigh, and other areas. Her urticaria began 1 day after onset of anosmia and 1 day prior to onset of fever. Shortly thereafter, she was diagnosed with COVID-19 and, thus far, has had a relatively mild disease course.
FUTURE PROSPECTS
We still have a tremendous amount to learn about the cutaneous manifestations of this disease, and there are currently more questions than answers. For one, it is still unclear what percentage of COVID-19 patients develops cutaneous eruptions. Although 20.4% of patients (18 of 88) in the Italian cohort developed cutaneous abnormalities, they were present in only 1.8% (2 of 1099 patients) in a Chinese cohort.1,12 Additionally, many of these patients are critically ill and have received numerous medications to help them survive their disease. Thus, as some authors point out in their reports, it can be challenging to determine when the cause of cutaneous eruptions are medication induced as opposed to truly being COVID-19 manifestations. For example, acral purpura can arise in the setting of treatment with vasopressors, and morbilliform eruptions are common manifestations of adverse reactions to drugs.
Several of the medications most actively being studied and used to treat patient with COVID-19 are also known to cause various cutaneous eruptions (Table 1). Furthermore, as many viral illnesses have associated exanthems and only a few COVID-19 patients with cutaneous abnormalities have been reported, it is not known if any of these are truly specific to infection with SARS-CoV-2. Many more cases are needed to resolve these dilemmas.
Cutaneous adverse reactions of medications currently being studied to treat patients with COVID-19
If there are specific COVID-19 cutaneous manifestations, it will be important to determine if any have clinical value. For example, are there specific early cutaneous abnormalities that may suggest a patient has been infected with SARS-CoV-2? If there are cutaneous manifestations that are pathognomonic for infection, these may be sufficient for diagnosis in lieu of testing in geographic areas where test availability is problematic. Also, are there cutaneous manifestations that can predict a more severe course and potentially encourage early aggressive intervention? Moreover, if effective medications emerge, are there certain cutaneous manifestations that may support specific treatment algorithms?
To answer such questions, it will be crucial to document the cutaneous abnormalities present at diagnosis and during the course of COVID-19 in as many patients as possible. Although this can be challenging in face of an obvious need to urgently address more critical clinical abnormalities, doing so may eventually reveal clinical clues to help guide diagnosis and treatment.
One possible protocol to collect cutaneous abnormality data could involve having nurses and other front-line healthcare workers photograph skin eruptions in COVID-19 patients when present. Dermatologists could examine these and collect clinical data virtually to optimize patient care and research efforts, which would also conserve personal protective equipment and minimize human exposure to SARS-CoV-2. At least one Italian group is adopting this practice. They also have enlisted front-line practitioners to use zip-lock transparent bags to transport their mobile phones or other photographic devices into COVID-19 patient rooms in order to minimize viral contamination.2
Acknowledgement
The authors would like to thank Janine Sot, MBA, for her expertise in creating figures 1 and 2.
Footnotes
The statements and opinions expressed in COVID-19 Curbside Consults are based on experience and the available literature as of the date posted. While we try to regularly update this content, any offered recommendations cannot be substituted for the clinical judgment of clinicians caring for individual patients.
- Copyright © 2020 The Cleveland Clinic Foundation. All Rights Reserved.




{kind=link}
{kind=link}