


Article Figures & Data
Figures
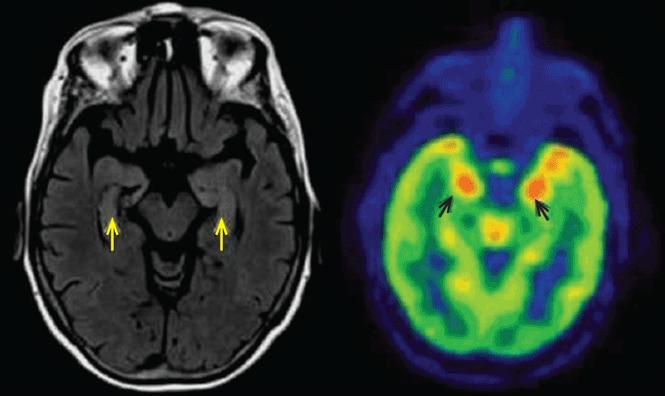
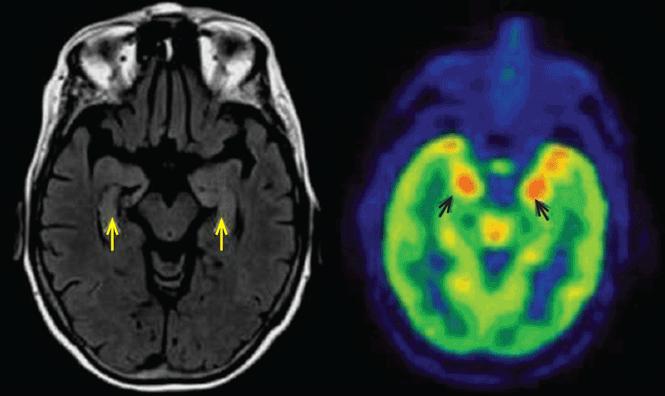
- FIGURE 1
Left, axial fluid-attenuated inversion recovery magnetic resonance imaging shows increased signal in the hippocampus bilaterally (yellow arrows). Right, fluorodeoxyglucose positron-emission tomography shows hypermetabolism in the hippocampi (black arrows).

Tables
Antigen location Antibody Frequency of tumor occurrence Tumor association Responsiveness to treatment Intracellular ANNA1 (anti-Hu) > 75% Small cell lung cancer Poor Anti-CV2 (CRMP) > 75% Small cell lung cancer, thymoma Poor, but longer survival than with ANNA1 Anti-Ma2 ~ 90% Testicular germ cell tumor Better than with ANNA1; prognosis is worse with co-occurrence of anti-Ma1 Anti-GAD65 < 33% None Seizure outcome inferior to that in anti-VGKC limbic encephalitis Cell surface (common)6,7 Anti-NMDA receptor 38% Ovarian teratoma Very good, but slow recovery Anti-LGI1 0 None Very good, quicker recovery than with NMDA receptor encephalitis Cell surface (rare)8,9 Anti-AMPA receptor 70% Thymoma, breast, lung Good Anti-GABAB receptor 47% Small cell lung cancer Good AMPA = alpha-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid; ANNA1 = antineuronal nuclear antibody 1; CRMP = collapsin-responsive mediated protein; GABAB = gamma-aminobutyric acid; GAD = glutamic acid decarboxylase; LGI1 = leucine-rich glioma-inactivated protein 1; NMDA = N-methyl-d-aspartate; VGKC = voltage-gated potassium channel
Syndrome Antigen location Antibody Tumor association Prognosis Brainstem Intracellular Anti-Hu (ANNA1) Small-cell lung cancer Poor Anti-Ri (ANNA2) Breast, lung Poor Anti-Ma2 Testicular germ cell tumor Good Cell surface Anti-NMDA (second stage disease) Ovarian teratoma Very good Anti-GQ1b None Very good Anti-NMO (antiaquaporin 4) None Good Cerebellar Intracellular Anti-Yo Ovarian, breast Poor Anti-Ri Breast, lung Good Anti-Tr Hodgkin lymphoma Fair Anti-GAD None Good Cell surface Anti-VGCC Small-cell lung cancer Fair Anti-mGluR1 Hodgkin lymphoma in remission Good (three cases re- ported, two improved) ANNA = antineuronal nuclear antibody; GAD = glutamic acid decarboxylase; GQ1b = ganglioside GQ1b; mGLuR1 = metabotropic glutamate receptor type 1; NMDA = N-methyl-d-aspartate; NMO = neuromyelitis optica; VGCC = voltage-gated calcium channel
Antigen location Antibody Characteristic neurologic syndrome Intracellular Anti-Yo (Purkinje cell cytoplasmic antibody type 1) Paraneoplastic cerebellar degeneration Anti-glutamic acid decarboxylase Stiff person syndrome (progressive encephalomyelitis with rigidity, myoclonus) Anti-Hu (ANNA1) Multiple, including paraneoplastic sensory neuropathy, paraneoplastic encephalomyelitis Anti-Ma2 Encephalitis, limbic or upper brainstem Antiamphiphysin Stiff person syndrome, paraneoplastic encephalomyelitis, limbic encephalitis Anti-CV2 (CRMP) Multiple, including uveitis, optic neuritis, retinitis, paraneoplastic cerebellar degeneration Cell surface Anti-NMDA receptor Multistage syndrome, starting with limbic encephalitis and psychiatric changes followed by brainstem dysfunction Anti-CASPR2 Encephalitis or peripheral nerve hyperexcitability (if both, Morvan syndrome) Anti-LGI1 Limbic encephalitis with faciobrachial dystonic seizures Anti-AMPA receptor Limbic encephalitis, isolated psychiatric disturbances Anti-GABAB receptor Limbic encephalitis, early prominent seizures Anti-glycine receptor Stiff person syndrome AMPA = alpha-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid; ANNA = antineuronal nuclear antibody; CASPR2 = contactin-associated protein 2; CRMP = collapsin-responsive mediated protein; GABAB = gamma-aminobutyric acid B; LGI1 = leucine-rich glioma-inactivated protein 1; NMDA = N-methyl-d-aspartate




{kind=link}
{kind=link}
Jump to section
- Article
- ABSTRACT
- NEWLY RECOGNIZED DISEASES
- CLASSIFIED ANATOMICALLY, IMMUNOLOGICALLY, OR EPONYMOUSLY
- SYNDROMES DEFINED BY BRAIN AREA AFFECTED
- LIMBIC ENCEPHALITIS
- BRAINSTEM ENCEPHALITIS
- CEREBELLAR SYNDROME
- SYNDROMES ASSOCIATED WITH SPECIFIC ANTIBODIES
- VGKC COMPLEX ANTIBODY-MEDIATED LIMBIC ENCEPHALITIS
- ANTI-NMDA RECEPTOR ENCEPHALITIS
- DIAGNOSIS OF AUTOANTIBODY-MEDIATED ENCEPHALITIS
- TREATMENT
- REFERENCES
- Figures & Data
- Info & Metrics