


Introduction
Inhalation is the standard route of administration for drugs used to treat chronic obstructive pulmonary disease (COPD) and asthma.1 Inhalation is a quick drug delivery method that offers both efficacy and safety.2,3 Inhaled administration allows targeted delivery of the active drug to the site of action, enabling lower doses and resulting in fewer systemic adverse events than oral therapy.3 There are 4 main types of devices used to deliver inhaled medication: pressurized metered-dose inhalers (pMDIs), dry powder inhalers (DPIs), soft mist inhalers (SMIs), and nebulizers. Each type of inhaler device is associated with advantages and limitations that determine their suitability for any given patient with COPD4,5 (TABLE 1).3,6,7 Understanding those advantages and limitations helps clinicians in choosing the proper device for the individual patient’s clinical needs and preferences. However, with the wide range of permutations of drug combinations now possible, inhaler selection remains challenging.4 For all inhaler devices, adequate training for patients on how to use their device is required to achieve optimal therapeutic benefits.1
Device considerations
Examples of the different inhaler devices available for COPD treatments are provided in FIGURE 1, and their key characteristics are summarized in TABLE 2.3,7 Traditional pMDIs require actuation of the device at the beginning of a slow, deep inhalation to optimize drug delivery. This technique requires hand–breath coordination, which can be difficult for some patients, particularly those who are elderly or severely short of breath; spacers can be used in combination with pMDIs to help to overcome some technique issues (FIGURE 1).3,8 Breath-actuated (BA) pMDIs may also be used in some countries (though are not currently licensed in the United States); these devices release the dose on inhalation, removing the need for hand–breath coordination.3

Examples of different inhaler device and spacer types
DPIs are also breath-actuated, with the patient providing the force necessary to deliver the drug on inhalation; drug delivery with DPIs is therefore dependent on patients achieving a high enough peak inspiratory flow (PIF) rate to disperse the drug, in contrast to BA pMDIs, which are activated at a lower PIF rate.3,8 Generating the inspiratory flow required for effective function of DPIs can be problematic for some patients with COPD.9 Suboptimal PIF rates have been associated with age (≥60 years), female gender, shorter height, and lower values for forced vital capacity and inspiratory capacity as percentage predicted in stable patients with severe COPD10; in addition, patients with COPD can have a temporarily reduced PIF rate after hospitalization for an acute exacerbation.11,12 There is a range of DPIs available in three main categories: single-dose, multi-dose, and power-assisted devices.7 It is important to protect DPI devices from the effects of humidity, which can increase particle adhesion and therefore reduce efficacy.13
The SMI delivers the aerosol as a fine mist with slow velocity lasting >1 second, which is considerably slower than spray delivery with pMDIs.14 The aim of this design is to make it easier for patients to coordinate actuation with inhalation, but it is important to note that some coordination is still required for SMI devices to function correctly.14 In addition, the SMI is not dependent on a patient’s ability to generate sufficient PIF for effective drug delivery. A limitation of the SMI is the need to assemble the device, as patients with poor manual dexterity may encounter difficulty when attempting to load the drug cartridge.15
Nebulizers deliver aerosolized drug in a fine mist. Newer-generation portable vibrating mesh nebulizers can deliver a dose over a period of ~2 minutes, compared with 10 minutes for conventional pneumatic devices.16 Patients find them effective and easy to use, and the newer generation devices overcome problems with portability and length of treatment, which may be an issue during the daytime for ambulatory patients, along with the requirement for cleaning after each dose.4,8 However, drug delivery may be somewhat compromised with nebulizers compared with other inhalation devices, as medication can be dispersed into the atmosphere and lost, rather than inhaled.7 An additional point to consider is medication availability; some medications, particularly fixed-dose combination maintenance therapies, are currently unavailable in a nebulized format.16
The most important device-related factors influencing the site of deposition within the lungs are aerosol velocity and particle size of the inhaled drug.3,7,17 To maximize clinical effectiveness, adequate distribution throughout the lung is required to reach target sites of action for β2-agonists, anticholinergics, and corticosteroids.17 Particle size differs between inhaler device types, but all available devices generate drug particles sufficient for deposition throughout the lower airways and lung periphery, ie, within the range of 1–5 microns.3,18–21 Extra fine particles of <1 micron (or “sub-micron particles”) can be deposited deeper in the pulmonary acinus, but a higher fraction of such particles may be exhaled compared with particles 1–5 microns in size.3,20,22 In contrast, particles >5 microns deposit in the oropharynx and may be swallowed, potentially leading to systemic adverse effects.3,20,22
When more than one drug is required, it may be preferable to deliver them via a single device where possible to facilitate patient compliance with correct technique, and decrease confusion about how to use different inhalers.23 The inhaler device ideally serves as a platform on which many treatments are available; the greater the number of devices employed by the patient, the greater the likelihood of making an error with the usage of each device.24
Importance of proper inhaler technique
Errors relating to device handling are common in patients with COPD. The results of a meta-analysis by Chrystyn et al reported that overall error rates were high across all devices in patients with COPD and asthma, ranging from 50%–100%25; the reported frequencies of patients with at least one error were 86.8% and 60.9% for pMDIs and DPIs, respectively. However, the authors note that heterogeneity between the studies used in the analysis was high, and suggest that future investigations should look to use a more standardized approach in assessment of inhaler device errors.25 Moreover, further studies to investigate the frequency of errors in SMI devices, and to establish the relationship between critical errors in device handling and device efficacy, are warranted.
Handling errors are directly linked to compromised drug delivery and reduced treatment efficacy.3 This may lead to more frequent or inappropriate medication use that, in turn, could result in unnecessary dose increases by the physician due to perceived lack of efficacy, and subsequently more adverse effects.3,26–28 However, these errors can be addressed through proper training and demonstration.29–32
Common device-handling errors include4,26,27,32,33:
pMDIs: not shaking the inhaler (for suspensions), not exhaling fully before actuation, inhaling too forcefully, and not holding their breath for long enough after inhalation.
DPIs: exhaling into the device mouthpiece, not exhaling fully before inhalation, not inhaling deeply or forcefully enough, and not holding their breath after inhalation.
SMIs: not rotating the inhaler with mouth cap facing upwards, rotating the inhaler while looking into the spray nozzle with the cap open (before inhalation), and not maintaining inhalation with drug spray.
Critical inhaler use errors (where an error results in no or an insufficient amount of medicine being delivered to the lungs, thereby leading to suboptimal disease control25) are less common; the frequencies of these errors for pMDIs and DPIs are summarized in TABLE 3.26
Critical errors and their reported frequencies for pressurized metered-dose inhalers and dry powder inhalers26
Incorrect inhaler use is a common cause of secondary nonadherence (ie, relating to incorrect medication use) among patients with COPD.4,34 Compromised inhaler technique and medication nonadherence jeopardize health outcomes and add to the economic burden of COPD.8,12,26 A 2005 study estimated that over 20% of the $25 billion spent on inhalers annually in the United States is wasted as a direct consequence of incorrect device handling.35
Failing to inhale correctly to achieve the optimal inspiratory flow for the specific device being used—deep and slow for pMDIs, or forceful, quick and deep for DPIs—is a critical handling error for inhaler devices.26 Significant associations between critical errors and clinical outcomes (hospitalization, emergency department visits, antibiotic courses, and corticosteroid courses) have been reported in COPD patients.26 In a retrospective analysis of COPD inpatients, suboptimal PIF rates with DPIs were associated with worse scores on the COPD Assessment Test, higher COPD and all-cause readmission rates, and shorter time to next COPD exacerbation.12
Patient considerations
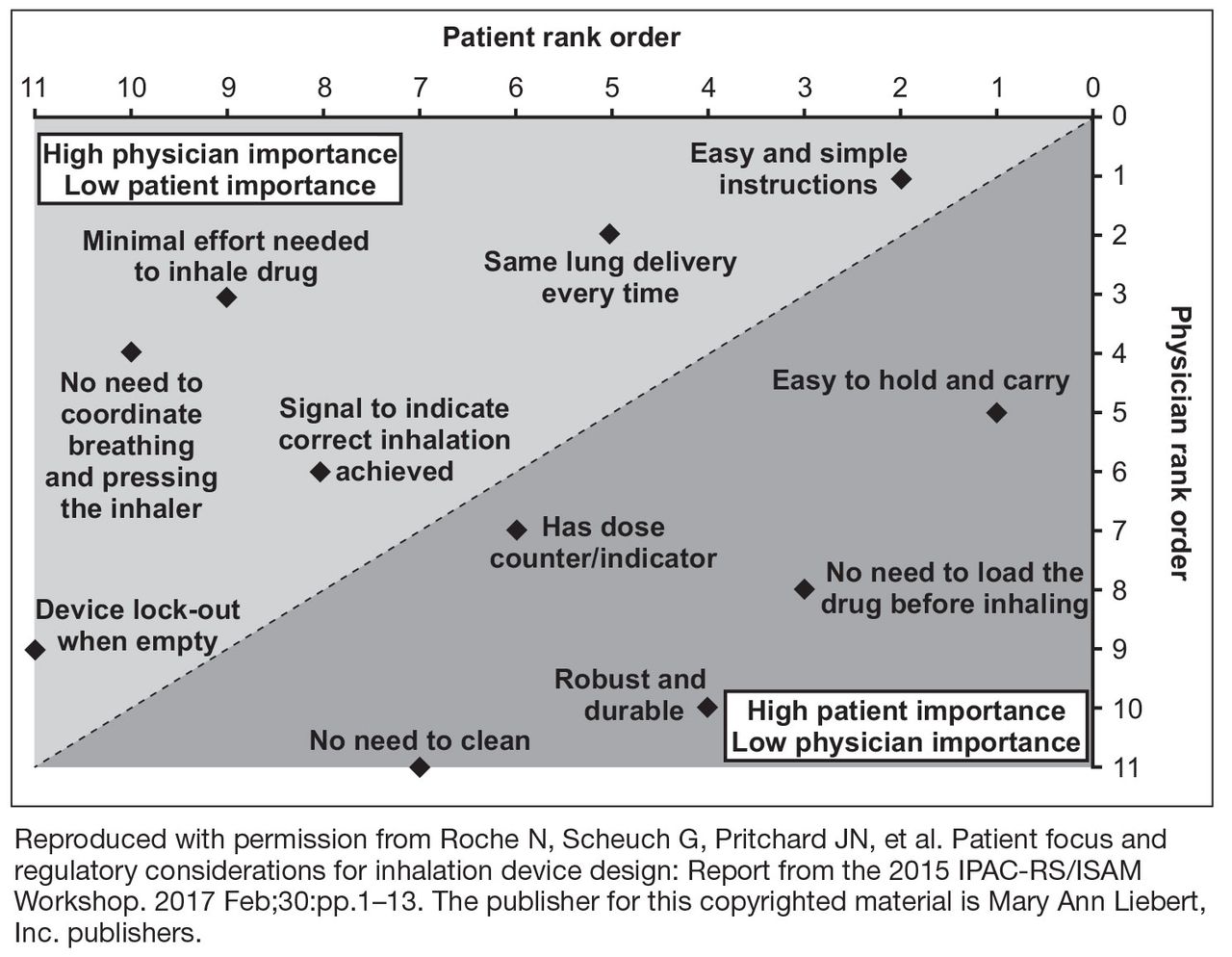
While various inhaled medications for COPD are available in different device types (TABLE 4), it is important to consider a patient’s perspective as part of treatment and device selection. For example, the effectiveness of an inhaled drug is dependent on the patient’s ability to use their prescribed inhaler correctly, which may be affected by physical issues (eg, poor manual dexterity, tremors, inspiratory flow rate) and cognitive or psychiatric issues (eg, poor memory/learning, depression).36 It is also important to consider that patient preferences for inhaler devices may differ from the perspective of a physician (FIGURE 2).4,23,37,38
Inhaled drugs by device type (with current FDA approval for patients with COPD)
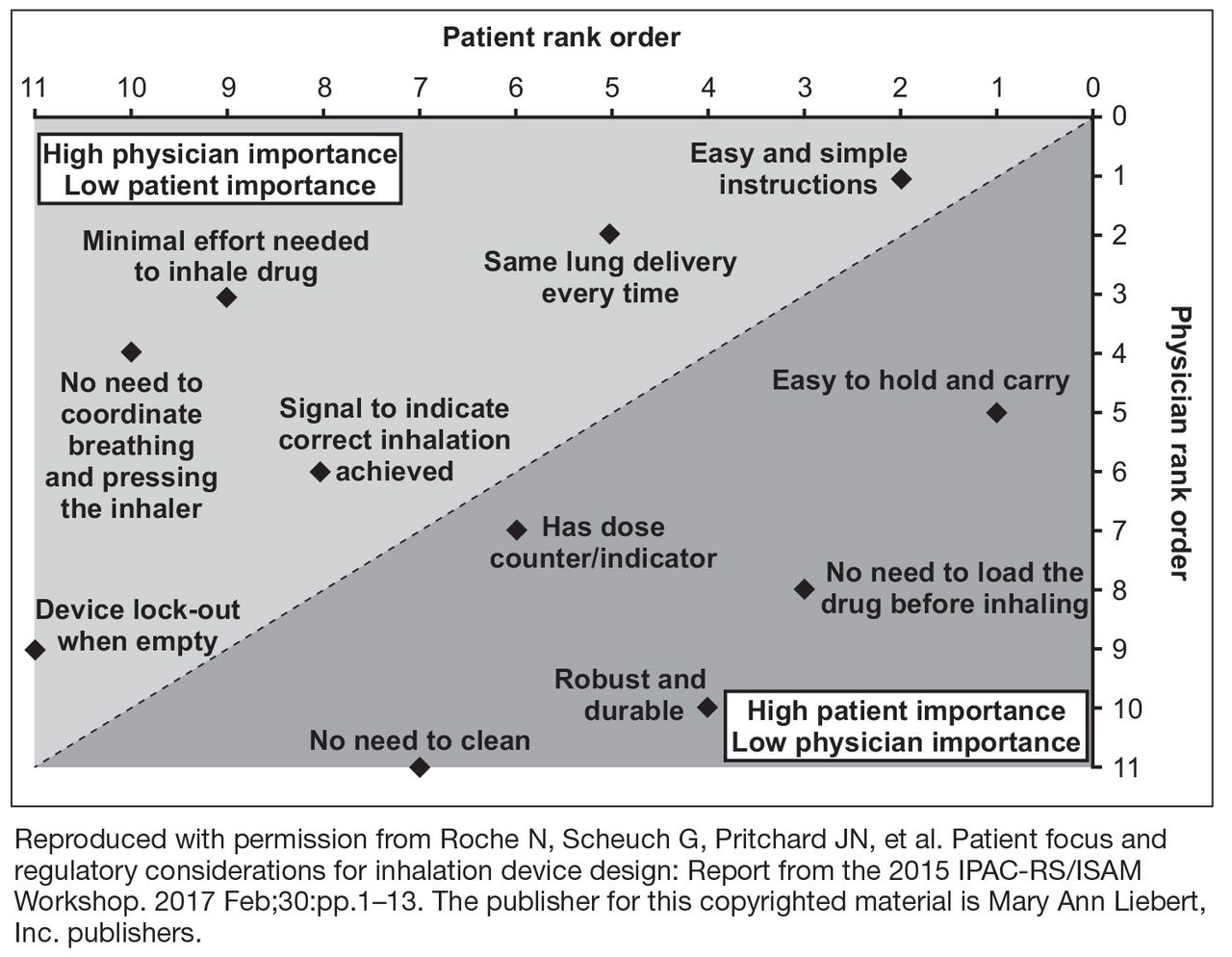
Preferences of patients and physicians regarding different aspects of inhaler device design38
One of the key factors affecting optimal drug delivery via an inhaler is whether the patient can generate a sufficient or appropriate PIF rate.3,9,12,39–42 Inhalation flow rates required for optimal drug deposition in the lungs differ between device types: for pMDIs, slow and deep inhalation at a flow rate of <90 L/min is generally recommended, whereas most DPIs require a minimum flow rate of 30 L/min, and a flow rate of >60 L/min to function optimally.3,39,43,44 DPIs with higher resistance allow for lower inhalation flow rates since the device-generated turbulence results in better drug disaggregation and microdispersion. However, patients with weaker or less efficient respiratory muscles may still struggle to attain an adequate PIF rate.39,40 For this reason, it may be preferential for patients with a PIF rate of <30 L/min to use a pMDI or SMI device, rather than a DPI.
Poor inhaler technique is frequently reported in patients with COPD or asthma, irrespective of the device used and with considerable variability in handling error rates for each individual device.25,26,35,45 Although clinical evidence is limited,25 research to date indicates that some DPIs may require less training than pMDIs.23,29,45,46 Therefore, DPI devices may be viewed as a more appropriate option for patients who encounter difficulty in coordinating the inhalation and actuation required for effective operation of a pMDI device. Alternatively, use of a spacer with pMDIs appears to reduce handling errors compared with pMDIs alone, but whether a pMDI plus spacer improves technique versus DPIs remains unclear.25,46,47 Lack of device training appears to be a key reason for inhaler handling errors across device types.26
Elderly patients need special consideration when selecting an inhaler and ensuring it is used correctly.48 Reduced physical ability and cognitive function due to age-related conditions (eg, dementia, depression, neuromuscular and cerebrovascular diseases) are the main reasons for suboptimal inhaler use in older patients, but other factors may also contribute (eg, multiple comorbid conditions, consequent complicated medication regimens).15 Older age is strongly associated with inhaler misuse,26 and has also been shown to have a negative correlation with PIF, independent of COPD severity.41 When compared with younger patients, older patients make more attempts before mastering the inhalation technique for a specific device, and need longer instruction time from trained health care professionals to correct inhaler mishandling.49,50 In elderly patients with adequate cognitive and manual ability, the most important factors in selecting a device are availability, convenience, ease of use, patient preference, and cost.8,23
Device continuity is a key consideration when multiple inhaled medications are needed.23 Lack of continuity of device type for different clinical needs means that patients may need to master the different techniques for each device.3 For instance, a patient may have a pMDI rescue medication, one or more DPIs for their maintenance therapy, and a nebulizer for additional bronchodilation, which may lead to confusion and incorrect device usage. Device continuity has been shown to improve disease control compared with using multiple inhalers in patients with asthma.51
Economic factors, particularly cost reimbursement in the United States, may influence a patient’s ability to access certain treatments and devices.8 Unfortunately, reasonably-priced, effective medication is not currently available for COPD, unlike other conditions such as diabetes. Medication cost has been shown to have a detrimental effect on adherence in patients with COPD.34
A full summary of patient-and physician-related considerations for device selection, along with suggestions for how these can be addressed, is provided in TABLE 5.
Factors affecting inhaler device selection and solutions
Inhaler device training for patients and physicians
Comprehensive instruction, including practical demonstration, is important for ensuring patients with COPD use the correct inhaler technique, with regular review and repeated instruction generally needed for continued correct use.1,23,32,42 Lack of instruction is significantly associated with inhaler misuse in patients with COPD or asthma.26 Verbal training on inhalation technique increased the number of patients achieving the minimum inhalation flow rate required for a range of different DPIs.39 Similarly, training helped patients using a pMDI to slow their inhalation rate to <90 L/min, as recommended for this type of device.39 The ‘teach-back’ method, where patients are asked to demonstrate correct usage of their inhaler after instruction from a health care professional,52 has shown to be particularly effective in pharmacist-led patient device training.53 Educational interventions that incorporated a physical demonstration significantly improved inhaler technique in patients with COPD and asthma compared with patients receiving written and verbal information alone.53 Proper device training in primary care settings should also include education about why the inhaler is needed.3
Face-to-face instruction from trained caregivers for approximately 5 to 10 minutes improves the use of MDIs and DPIs by patients.49 However, clinical research indicates that learning correct handling and use may be easier and quicker for some devices than for others.31,49 For example, patients naïve to the PulmoJet (a DPI device not currently available in the United States) were found to have fewer serious errors after training than those using Diskus or Turbuhaler devices.24 In another study, it took less time to correct errors in inhaler use with the Diskus compared with the Handi-Haler.44 Health care professionals themselves may lack training or knowledge on correct use of inhaler devices,35,36,54 with 1 study finding that up to 67% of nurses, doctors, and respiratory therapists were unable to describe or perform critical steps for using inhalers.35
A range of resources is available to aid in training patients and health care professionals in inhaler techniques:
Tools such as the In-Check DIAL inspiratory flow meter (Clement Clarke International Ltd, Harlow, UK), TurbuHaler Trainer (AstraZeneca, Lund, Sweden), Diskus/Accuhaler Training Device (Vitalograph, Ennis, Ireland), and 2Tone Trainer (Canday Medical Ltd, Newmarket, UK) can be used to evaluate a patient’s physical ability to use a specific inhaler.55
The emergence of electronic monitoring devices, such as SmartTrack, SmartTurbo, and SmartMat (all developed by Adherium Ltd, Auckland New Zealand), can provide objective and detailed adherence data to support clinical decision-making.56
It is essential that patients and physicians alike utilize the instructions and video demonstrations available online to understand how to use a device correctly, and avoid errors. These resources can be found on a number of organizations’ websites (eg, COPD Foundation, Allergy and Asthma Network, Centers for Disease Control and Prevention, National Jewish Health, Asthma UK, Centre for Pharmacy Postgraduate Education) and on manufacturers’ websites for individual inhalers or treatments (eg, https://www.advair.com/how-to-use-advair.html, https://www.incruse.com/how-to-use-incruse.html, https://www.mysymbicort.com/ copd/taking-symbicort/how-to-use-the-inhaler.html, https://www.tudorzahcp.com/tudorza-instructions-dosing.html, www.us.respimat.com (“How to Use the RESPIMAT Inhaler”), https://www.utibron.com/how-to-use.html).
Conclusions
A number of inhalation devices are available for the treatment of COPD. However, incorrect usage or a poor match between the patient and the device may lead to confusion, suboptimal treatment, and increased cost to the patient and health care system. Considering both patient-and health care system-related factors can ensure that appropriate inhaler section and usage can be optimized.
Footnotes
DISCLOSURES
Dr. Dhand has participated on advisory boards for AstraZeneca, Bayer Healthcare, Cipla Limited, and GlaxoSmithKline, and has received honoraria from AstraZeneca, Cipla Limited, and Sunovion Pharmaceuticals Inc.
Dr. Cavanaugh has no financial interests to declare.
Dr. Skolnik has participated on advisory boards for AstraZeneca; Boehringer Ingelheim GmbH; Eli Lilly and Company; Intarcia Therapeutics, Inc.; Janssen Pharmaceuticals, Inc.; sanofiaventis U.S. LLC; and Teva Pharmaceutical Industries, Ltd.; as a speaker for AstraZeneca and Boehringer Ingelheim GmbH; and has received research support from AstraZeneca and sanofiaventis U.S. LLC.
Funding for this article was provided by AstraZeneca LP (Wilmington, DE, USA). Medical writing support was provided by Hannah Burke, BSc, of Core (London, UK) and editorial support was provided by Maryam Vahdat, PGDip, of Core (London, UK), which were funded by AstraZeneca LP (Wilmington, DE, USA), in accordance with Good Publication Practice guidelines (Battisti WP et al. Ann Intern Med. 2015;163:461–464. doi: 10.7326/M15-0288).
This article is being co-published in The Journal of Family Practice and Cleveland Clinic Journal of Medicine.
- © 2019 The Cleveland Clinic Foundation. All Rights Reserved.
REFERENCES
In this issue



{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.