


ABSTRACT
Lifestyle factors remain the bedrock of atherosclerotic cardiovascular disease (ASCVD) prevention. Statins remain the first-line therapy for primary and secondary prevention of ASCVD. Physicians are encouraged to discuss the risks and benefits of statins with patients before beginning therapy. Nonstatins and proprotein convertase subtilisin-kexin type 9 inhibitors are recommended for secondary prevention in patients with clinical ASCVD. For patients at intermediate risk of ASCVD, new risk-enhancing factors, including chronic inflammatory conditions and ethnicity, should be considered to better risk stratify these patients.
Lifestyle factors are the cornerstone of preventing ASCVD.
High low-density lipoprotein cholesterol (LDL-C) levels warrant intervention.
Statins are the first-line therapy for lowering LDL-C and preventing ASCVD.
Calcium score and risk-enhancing factors help stratify risk in patients of intermediate risk.
Nonstatin agents are warranted in patients not achieving LDL-C reduction goals despite maximum statin therapy or in primary prevention for patients at very-high risk and not achieving LDL-C reduction goals.
INTRODUCTION
Maintaining healthy cholesterol levels is essential to primary and secondary prevention of atherosclerotic cardiovascular disease (ASCVD). High cholesterol raises the risk of heart disease, which is the leading cause of death in the United States.1 Just over 50% of US adults who would benefit from cholesterol-lowering medication are taking it.2
2018 CHOLESTEROL GUIDELINES
The recent 2018 cholesterol guidelines for prevention of ASCVD again stress the importance of lifestyle and role of statins as first-line therapy in primary and secondary prevention. The guidelines affirm the need to aggressively treat patients with high cholesterol and particularly patients at high risk of ASCVD.
Table 1 highlights key updates to the cholesterol guidelines with respect to a clinician-patient risk discussion before beginning statins, tailoring treatment using a more extensive list or risk modifiers, additional testing for patients of intermediate risk, and use of nonstatin agents in secondary prevention.3,4
Key updates (in bold) to the cholesterol guidelines
WHAT REMAINS THE SAME
Like the 2013 cholesterol guidelines, the new 2018 guidelines stress lifestyle, such as diet and exercise, statin therapy as the first-line drug for treating for atherosclerosis risk reduction, and risk assessment using the Pooled Cohort Equation in primary prevention of ASCVD.
Lifestyle: Cornerstone of ASCVD prevention
Lifestyle factors such as tobacco cessation, diet, exercise, weight management, and blood pressure management remain the cornerstone of primary and secondary prevention of ASCVD. A healthy diet that ensures the best nutritional value for caloric intake is recommended, such as a Mediterranean-style diet including whole grains and limiting red meat.
Unfortunately, the reality is that the lifestyle of very few Americans meets the lifestyle factor guide lines. The average American gets about 16 grams of fiber a day5 as opposed to the recommended 30 grams.6 Total animal consumption per capita in the United States has steadily increased and currently stands at 225 pounds of meat.7
For exercise, the American Heart Association recommends 30 minutes or more of moderate-intensity aerobic activity at least 5 days a week and high-intensity strengthening at least 2 days a week.8 As with diet, Americans fall short of exercise recommendations with 39% considered sedentary, 60% get no regular exercise, and of those who exercise, 80% are not exercising effectively. Rates of sedentary lifestyle also increase with age.9
These data are clear that most patients do not meet lifestyle recommendations for diet and exercise to prevent ASCVD.
Patient factors that warrant treatment
As stated, adherence to a healthy lifestyle is the primary prevention of ASCVD for all patients (Figure 1). Treatment to maintain healthy cholesterol and prevent cardiovascular disease is warranted in patients who have had clinical ASCVD (Figure 2); for everyone else, treatment is based on a calculation of risk, including other conditions such as hypercholesterolemia and diabetes:
Primary hypercholesterolemia (low-density lipoprotein cholesterol [LDL-C] > 190 mg/dL)
Diabetes and age 40 to 75
Others factors based on calculated risk (Pooled Cohort Equation, coronary artery calcium [CAC], risk-enhancers)
ASCVD including myocardial infraction, coronary artery disease, percutaneous coronary intervention/coronary artery bypass grafting, other arterial revascularization, transient ischemic attack, and stroke.

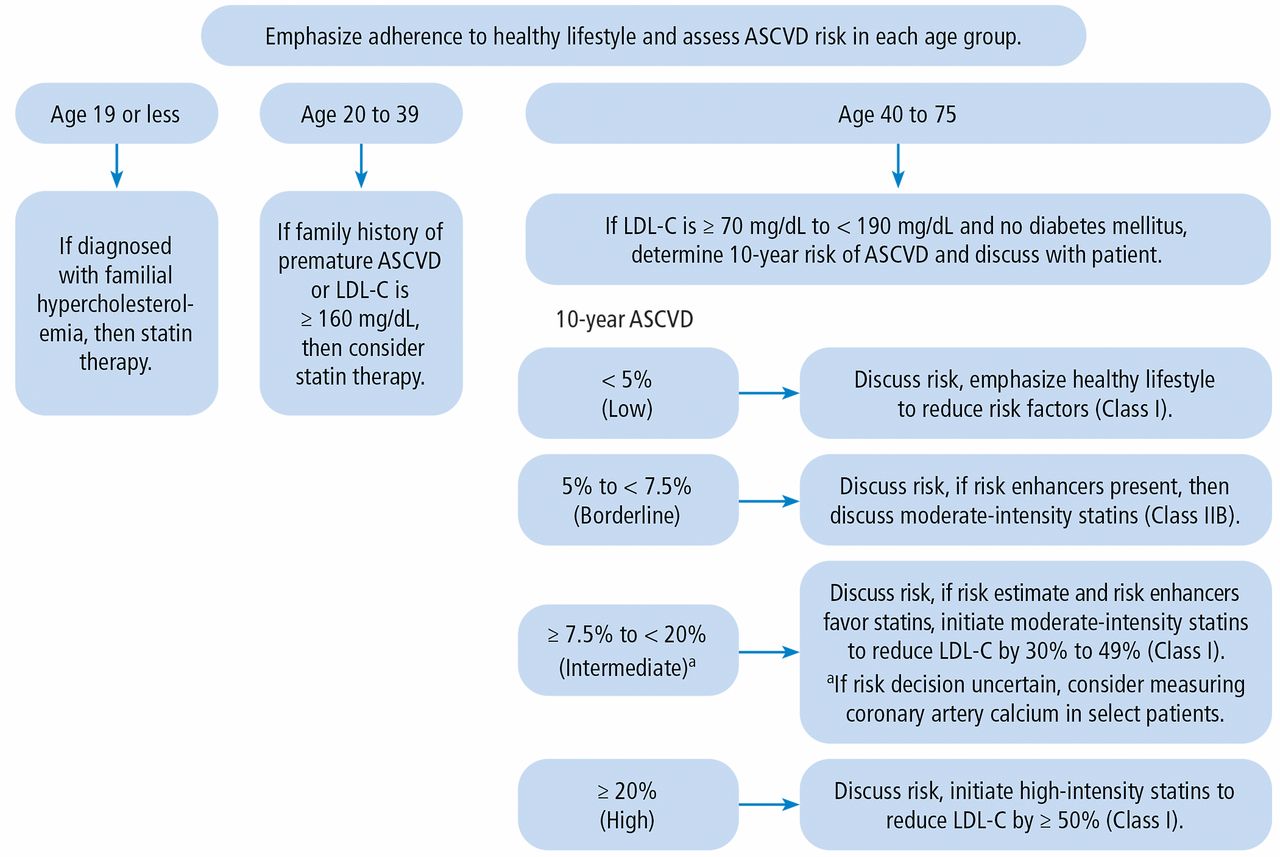
Primary prevention for atherosclerotic cardiovascular disease (ASCVD).
LDL-C = low-density lipoprotein cholesterol
Source: Data from reference 4.
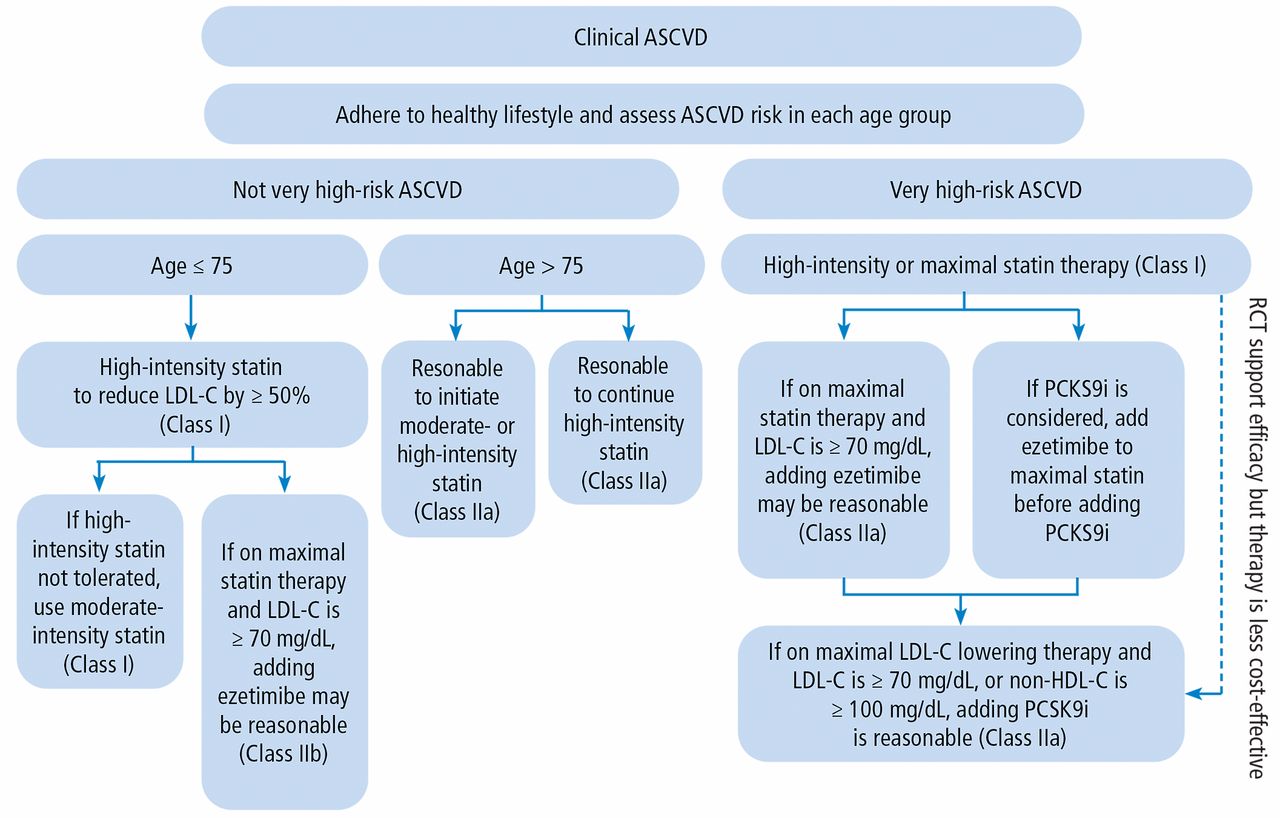
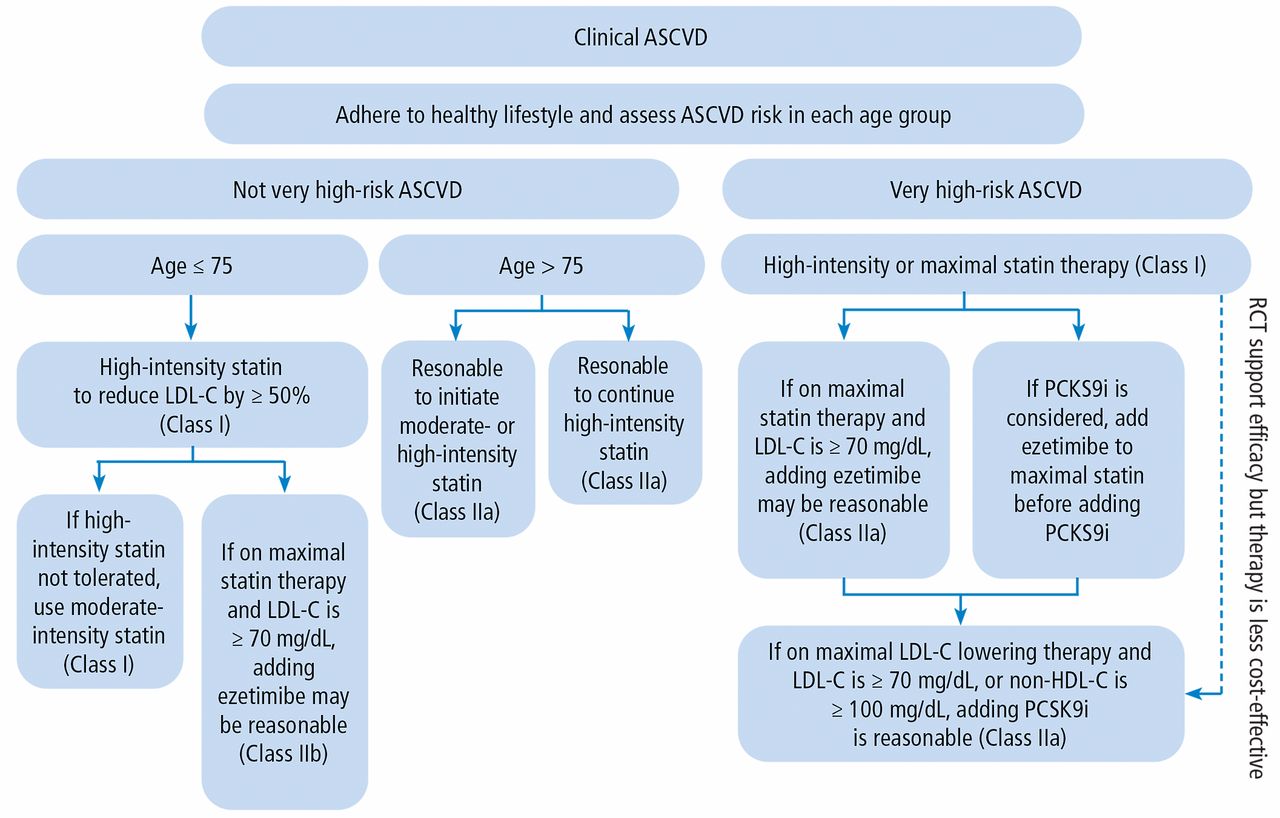
Secondary prevention for atherosclerotic cardiovascular disease (ASCVD).
HDL-C = high-density lipoprotein cholesterol; LDL-C = low-density lipoprotein cholesterol; PCKS9i = proprotein convertase subtilisin-kexin type 9 inhibitors; RCT = randomized controlled trial
Source: Data from reference 4.
High LDL-C warrants statin therapy. In addition to unfavorable lifestyle factors, high LDL-C is a known risk factor for ASCVD and it warrants intervention. Regardless of age, patients with LDL-C greater than 190 mg/dL should be started on a statin therapy. The latest guidelines now encourage a discussion of ASCVD risk between the clinician and patient before beginning statin therapy.4
The selection and use of statin therapy is based on the LDL-C reduction goals as discussed below.
Calculated risk. In the absence of prior ASCVD, determining a patient’s 10-year risk of ASCVD starts with a risk calculation such as the Pooled Cohort Equation. Risk calculation is based on age, sex, race, blood pressure, cholesterol, tobacco use, history of diabetes, and treatment with a statin or aspirin or for hypertension. A result of 5% to 7.4% indicates moderate 10-year risk of ASCVD and 7.5% or greater indicates a high 10-year risk (http://tools.acc.org/ASCVD-Risk-Estimator-Plus/#!/calculate/estimate/).
For patients with a calculated risk of ASCVD in the moderate range, the new guidelines contain several new important risk enhancers to consider, as discussed below.
WHAT IS NEW
In addition to a patient-physician discussion before beginning statins, the biggest changes in the new cholesterol guidelines relate to identifying patients at intermediate risk of ASCVD and how best to stratify their level of risk.
Intermediate risk
The 2018 guidelines recommend new tools to further stratify patients at intermediate risk for ASCVD using CAC scoring and other new risk-enhancing factors.
CAC scoring. CAC score measures the amount of calcium in the artery walls of the heart and arterial plaque and can help further stratify patients with an intermediate risk for ASCVD. For patients at moderate risk and unsure about use of statin therapy, a CAC score may help inform risk-benefit treatment decisions. A CAC score of:
A 0 indicates lower risk and favors continued dietary and lifestyle modifications and no statin therapy unless diabetes, family history of premature coronary heart disease, or cigarette smoking are present
1 to 99 indicates elevated risk and favors use of statin therapy especially after age 55
100 or greater or the 75th percentile or greater, indicates the need to initiate statin therapy.
Risk-enhancing factors. The latest cholesterol guidelines include an extensive list of risk-enhancing factors (Table 2). Family history is a risk factor, as in the past, in addition to metabolic disease, primary hypercholesterolemia, and chronic kidney disease.
Risk-enhancing factors for ASCVD
Notably, chronic inflammatory conditions, such as psoriasis, rheumatoid arthritis, and lupus, are now considered risk-enhancing factors. Research indicates that autoimmune disease increases the risk for atherosclerosis by 300% to 500%.10
The risk factors related to autoimmune disease are particularly relevant to women because 80% of autoimmune disease occurs in women. Additional risk enhancers unique to women are premature menopause, menopause before the age of 40 regardless of whether surgically or naturally, preeclampsia, gestational diabetes, and polycystic ovary syndrome.
Another novel factor included in the new guidelines is high-risk ethnicity among South Asians. Lipid and biomarker factors include high-sensitive C-reactive protein, lipoprotein(a), apolipoprotein B, and ankle-brachial index. Lipoprotein(a) is a genetic disorder occurring in 20% of the population and it increases the risk of early MI and stroke.11 A randomized, phase 3 trial in 8,000 patients of an antisense oligonucleotide drug for cardiovascular disease and lipoprotein(a) is underway (NCT04023552 available at clinicaltrials.gov).
The new extensive list of risk enhancers should be considered to risk stratify and tailor treatment in patients with an intermediate risk of ASCVD.
Very high risk/secondary prevention: Nonstatins and PCSK9 inhibitors
Finally, there is new guidance about the role of non-statin agents, such as ezetimibe and proprotein convertase subtilisin-kexin type 9 (PCSK9) inhibitors, in secondary prevention. Very high risk of ASCVD exists in patients with a clinical history of a major atherosclerotic event, recent ASCVD, myocardial infarction, or ischemic stroke. These high-risk patients should have an LDL-C less than 70 mg/dL, though the Endocrine Society recommends LDL-C less than 55 mg/dL in patients diabetes and high-risk features for ASCVD. 12
There are 3 nonstatin drugs currently available for LDL-C reduction (Table 3). Ezetimibe is a cholesterol absorption inhibitor shown to lower LDL-C by 18% taken as monotherapy and 25% taken as combination therapy.4
Nonstatin therapy for reduction of LDL-C
The 2 available PCSK9 inhibitors, alirocumab and evolocumab, inhibit LDL-C receptors from breaking down.4 Reduction of LDL-C is reportedly similar at 45% to 58% for alirocumab and 58% to 64% evolocumab depending on the dose.4
A very interesting finding about PCSK9 inhibitors is that unlike statins, no matter how low LDL-C levels go, there is no increased in the risk of diabetes.13
STATINS
Important updates to the 2018 cholesterol guidelines include an emphasis on a risk-benefit discussion between the clinician and patient before beginning statin therapy.
Statins remain the first-line drugs for lowering cholesterol and ASCVD risk reduction. The type of statin and dose depends on the intensity or degree of reduction of LDL-C desired (Table 4).
Statin therapy for reduction of LDL-C
SUMMARY
With so much awareness and talk about the importance of cholesterol, many have the false impression that patients are being over treated for it. In fact, a very small percentage of patients take 2 lipid-lowering drugs and much of the patient population at high risk for ASCVD is not under control, especially women. The data are robust that patients at high clinical risk for ASCVD should be treated aggressively. For patients at intermediate risk, calcium scoring and attention to risk-enhancing factors can help stratify ASCVD risk, as well as present an opportunity for discussion and shared decision-making.
Footnotes
Dr. Cho reported research trial support from Amgen, Novartis, and Esperion and consulting/advisory fees from Amgen, Esperion, and AstraZeneca.
This article is based on Dr. Cho’s presentation at the Sones/Favaloro Scientific Program, “Multidisciplinary Management of Acute and Chronic Conditions: Yielding Exceptional Outcomes,” held in Cleveland, OH, November 8, 2019. The article was drafted by Cleveland Clinic Journal of Medicine and was then reviewed, revised, and approved by Dr. Cho.
- Copyright © 2020 The Cleveland Clinic Foundation. All Rights Reserved.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.