


ABSTRACT
The stenosis or occlusion of extremities defining peripheral artery disease (PAD) is a risk factor for adverse cardiovascular events and adverse limb events including amputation. PAD is common, can occur without symptoms or with claudication, and is easily diagnosed. Proper diagnosis and adherence to guideline-directed therapy can reduce the morbidity and potential mortality associated with PAD.
PAD is stenosis or occlusion of the upper or lower extremities caused by atherosclerotic plaque.
PAD is common, often overlooked because it is frequently asymptomatic, but easily diagnosed by obtaining an ankle-brachial index.
Management and medical therapies for PAD include lifestyle measures, optimal blood pressure and cholesterol control, antithrombotic agents to manage the risk of thrombotic events, and claudication therapy.
INTRODUCTION
Peripheral artery disease (PAD) is characterized by stenosis or occlusion of the arteries of the upper or lower limbs due to atherosclerotic plaque in the vessel walls.1 PAD is common but often overlooked. A public awareness survey found 74% of respondents (N = 2,501) were not aware of PAD.2 Unfortunately, many physicians also lack awareness of PAD or fail to consider it when evaluating patients.
PAD is easily diagnosed in any office setting by obtaining an ankle-brachial index, which is the ratio calculated by the measured lower extremity (ankle) systolic pressure divided by the brachial artery (arm) systolic pressure.3 An ankle-brachial index of 0.91 to 1.4 is normal, 0.90 or less is diagnostic for PAD, and less than 0.40 is diagnostic for severe PAD. Patients may experience leg pain (claudication), rest pain, or leg ulcerations. The ankle-brachial index is 95% sensitive and 99% specific for PAD.3 With greater awareness and screening for PAD, significant patient morbidity can be avoided.
EPIDEMIOLOGY AND PATHOPHYSIOLOGY
Over 200 million people worldwide have PAD and it occurs in men and women equally. The prevalence of PAD increases with age occurring in about 30% of people over 70 and in people 50 to 69 with diabetes or those who smoke.4 Both mortality and disability from PAD have increased over the last several decades. Patients with PAD are at high risk for major adverse cardiovascular events and major adverse limb events, the most dreaded complication being amputation.
SIGN AND SYMPTOMS
Failure to recognize PAD is largely due to the absence of symptoms. In the ambulatory setting, about 50% of individuals with PAD have no leg symptoms whatsoever.5 Only about 15% of those with PAD have typical claudication, 30% have atypical limb symptoms, and about 3% have critical limb ischemia.
The 5-year outcome for patients with PAD includes stable claudication in 70% to 80% of patients; 10% to 20% will require lower extremity revascularization, and about 1% to 2% will go on to have chronic limb ischemias (Table 1).6 Amputation rates are as high as 25% in patients with chronic limb ischemia. It is important to note that for patients with PAD, 20% will have a myocardial infarction or stroke, and death can occur in 15% to 30% over a 5-year period. As these data make clear, PAD is not a benign condition.
Natural history of peripheral artery disease
MEDICAL THERAPIES AND MANAGEMENT
As stated, PAD is routinely underdiagnosed but even with proper diagnosis, patients with PAD are less frequently treated with guideline-directed therapies compared with patients with coronary artery disease.4 Medical therapies for, and the management of PAD revolve around preventing myocardial infarction, stroke, and death; improving function and quality of life; and protecting the feet to avoid and prevent amputation.
Diet, exercise, tobacco cessation
Patients with PAD should be counseled about maintaining a healthy diet, exercise, and complete cessation of tobacco use. Recommended exercise programs for patients with PAD have been established and are covered services for older patients by US Centers for Medicare & Medicaid Services.7 A 12-week supervised treadmill exercise program consists of 3 weekly sessions that begin at 15 minutes and increase to 45 to 50 minutes a session. A home-based walking exercise program or a supervised ergometry exercise program are also recommended and may be better suited to some patients.
Medical therapy
In addition to lifestyle measures, medical therapies for PAD should be employed to:
Optimize blood pressure preferably using an angiotensin-converting-enzyme inhibitor
Lower and maintain low-density lipoprotein cholesterol (LDL-C) to less than 70 mg/dL using a statin, ezetimibe, or a proprotein convertase subtilisin-kexin 9 inhibitor or combination.
Manage risk of thrombotic events with antithrombotic agents such as aspirin, clopidogrel, ticagrelor, vorapaxar, and rivaroxaban
Treat claudication pain in the extremities with cilostazol if no heart failure.
Several major clinical trials have evaluated antithrombotic agents in patients with PAD, especially symptomatic PAD (Table 2).8–25
Clinical trials of antithrombotic therapy for peripheral artery disease (PAD)
Among these trials, Cardiovascular Outcomes for People Using Anticoagulation Strategies (COMPASS) evaluated cardiovascular outcomes in 27,395 patients including 27% with PAD.20 Patients received 2.5 mg rivaroxaban twice daily plus 100 mg aspirin, or 5 mg rivaroxaban twice daily, or 100 mg aspirin daily. The cardiovascular outcomes in patients with stable atherosclerotic vascular disease were more favorable in the rivaroxaban-plus-aspirin cohort (hazard ratio = 0.76; 95% confidence interval [CI] 0.66–0.86; P = .001) compared with the rivaroxaban-alone cohort (hazard ratio = 0.90; 95% CI 0.79–1.03; P = .12), but more major bleeding events occurred in patients on rivaroxaban plus aspirin (3.1%) compared with rivaroxaban alone (1.9%). The secondary composite outcome of ischemic stroke, myocardial infarction, acute limb ischemia, or cardiovascular death also favored rivaroxaban-plus-aspirin therapy, with emphasis on screening for bleeding.
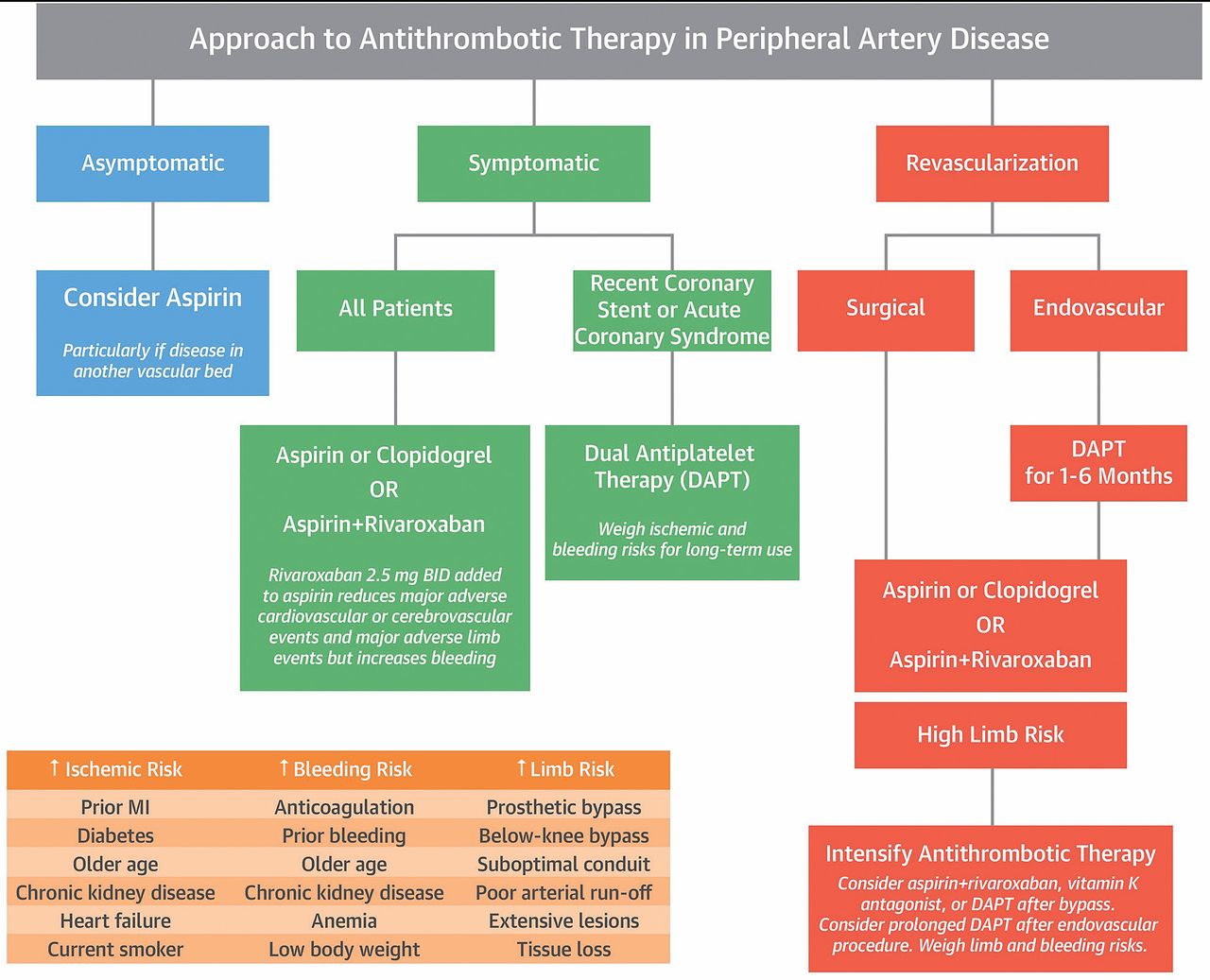
Figure 1 outlines a frequently used approach to antithrombotic therapy showing that all patients with symptomatic PAD should receive aspirin or clopidogrel or aspirin with rivaroxaban.8 In patients with asymptomatic PAD, aspirin should be considered especially if disease is present in another vascular bed.

Therapeutic approach for patients with peripheral artery disease.
BID = 2 times per day; MI = myocardial infarction
Reprinted from Hussain MA, et al. Antithrombotic therapy for peripheral artery disease: recent advances. J Am Coll Cardiol 2018; 71(21):2450–2467. Copyright 2018, with permission from The American College of Cardiology Foundation.
Summary of risk reduction therapy for patients with PAD
The American College of Cardiology/American Heart Association 2016 guidelines on the management of patients with lower extremity PAD advise that reduction of risk for major adverse limb events should include healthy lifestyle modifications, tobacco cessation, achieving target blood pressure goals, glucose lowering therapy, LDL-C lowering using a statin or ezetimibe or a PCSK9 agent, and antiplatelet therapy.4,5
The Further Cardiovascular Outcomes Research With PCSK8 Inhibition in Subjects With Elevated Risk (FOURIER) trial provides insight into LDL-C levels and outcomes in patients with PAD.26 Of the 27,564 patients in the FOURIER trial, 13.2% had PAD and by lowering LDL-C to a median of 31 mg/dL in patients with symptomatic PAD, major adverse cardiovascular events and major adverse limb events were reduced significantly. Evolocumab plus a statin to reduce LDL-C levels reduced the risk of major adverse limb events (ie, limb ischemia or loss of limb) by 42% in 2 study populations.26
For some patients with more advanced disease, aspirin together with rivaroxaban (2.5 mg twice daily) or ticagrelor (60 mg twice daily) or clopidogrel (75 mg once daily) with or without vorapaxar (2.08 mg once daily) is appropriate. Claudication therapy with cilostazol (100 mg twice daily) can be used for patients without heart failure.
Footnotes
The authors reported no financial interests or relationships that pose a potential conflict of interest with this article.
This article is based on Dr. Bartholomew’s presentation at the Sones/Favaloro Scientific Program, “Multidisciplinary Management of Acute and Chronic Conditions: Yielding Exceptional Outcomes,” held in Cleveland, OH, November 8, 2019. The article was drafted by Cleveland Clinic Journal of Medicine and was then reviewed, revised, and approved by Dr. Bartholomew.
- Copyright © 2020 The Cleveland Clinic Foundation. All Rights Reserved.
REFERENCES
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.