


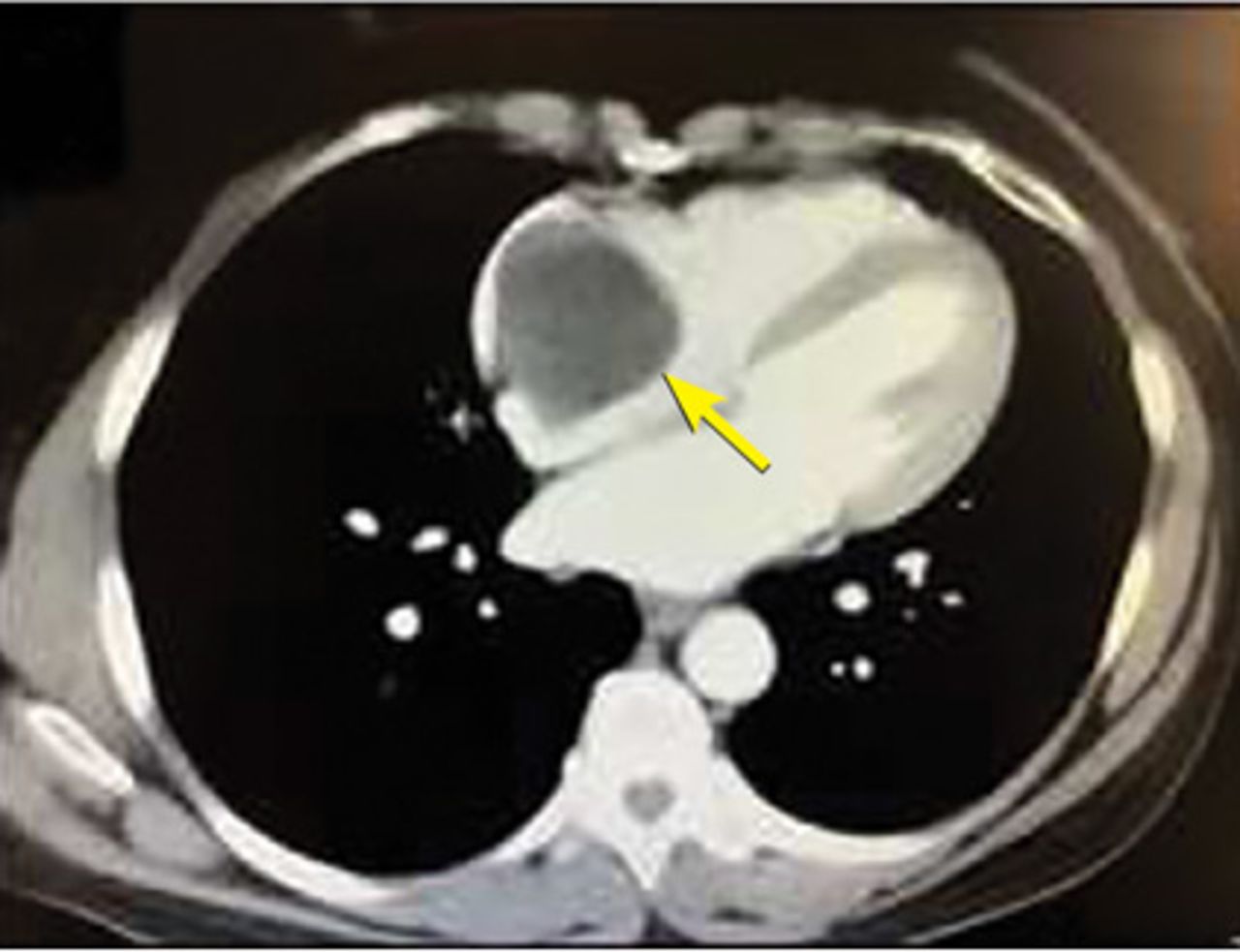
A 55-year-old woman with hypertension, hyperthyroidism, and endometrial adenocarcinoma treated 5 years earlier presented with occasional shortness of breath and dizziness. To rule out pulmonary embolism, computed tomography of the chest was done and showed a high-density lesion in the right atrium of the heart, measuring up to 4.5 cm (Figure 1).
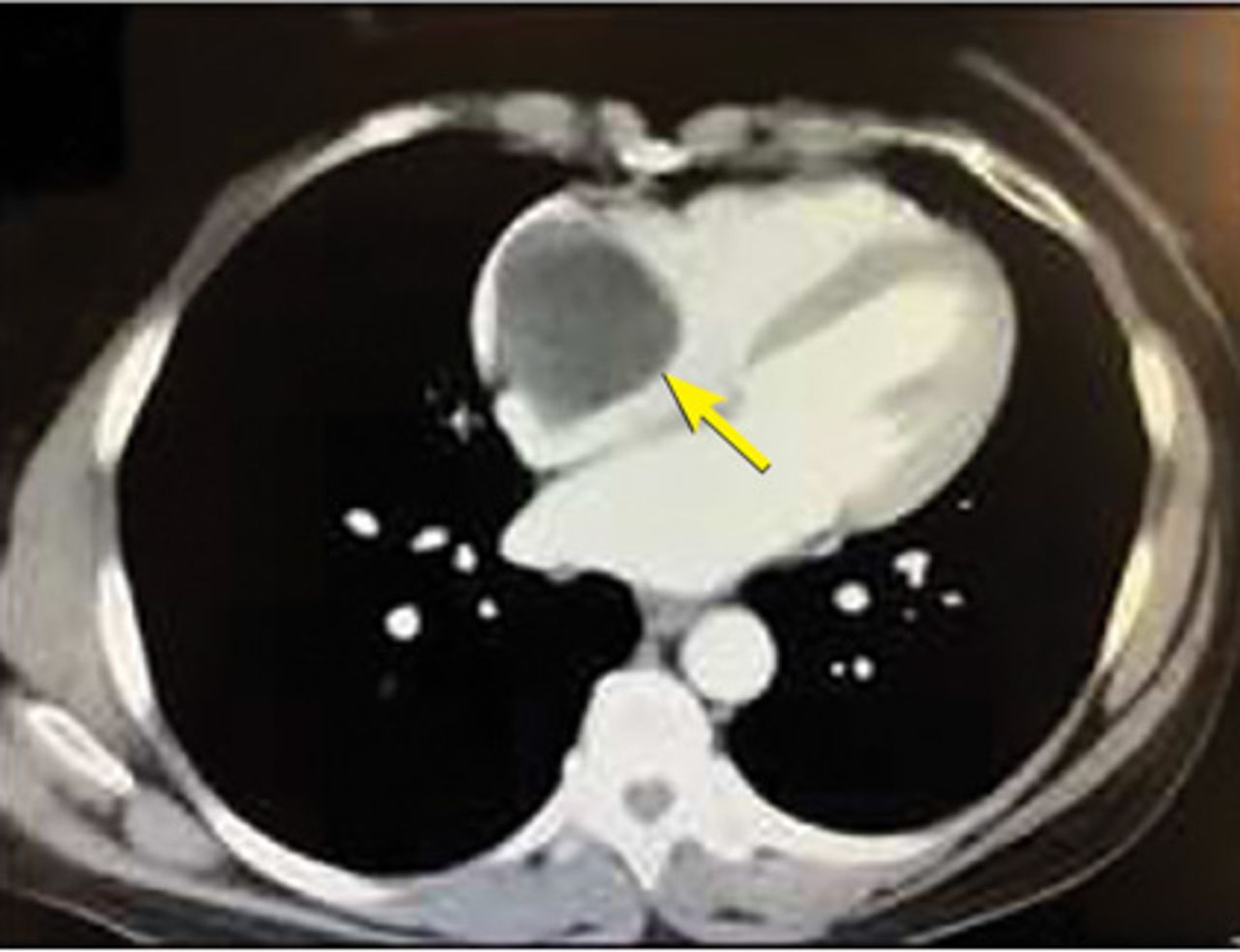
Computed tomography of the chest. An arrow points to the mass in the right atrium.
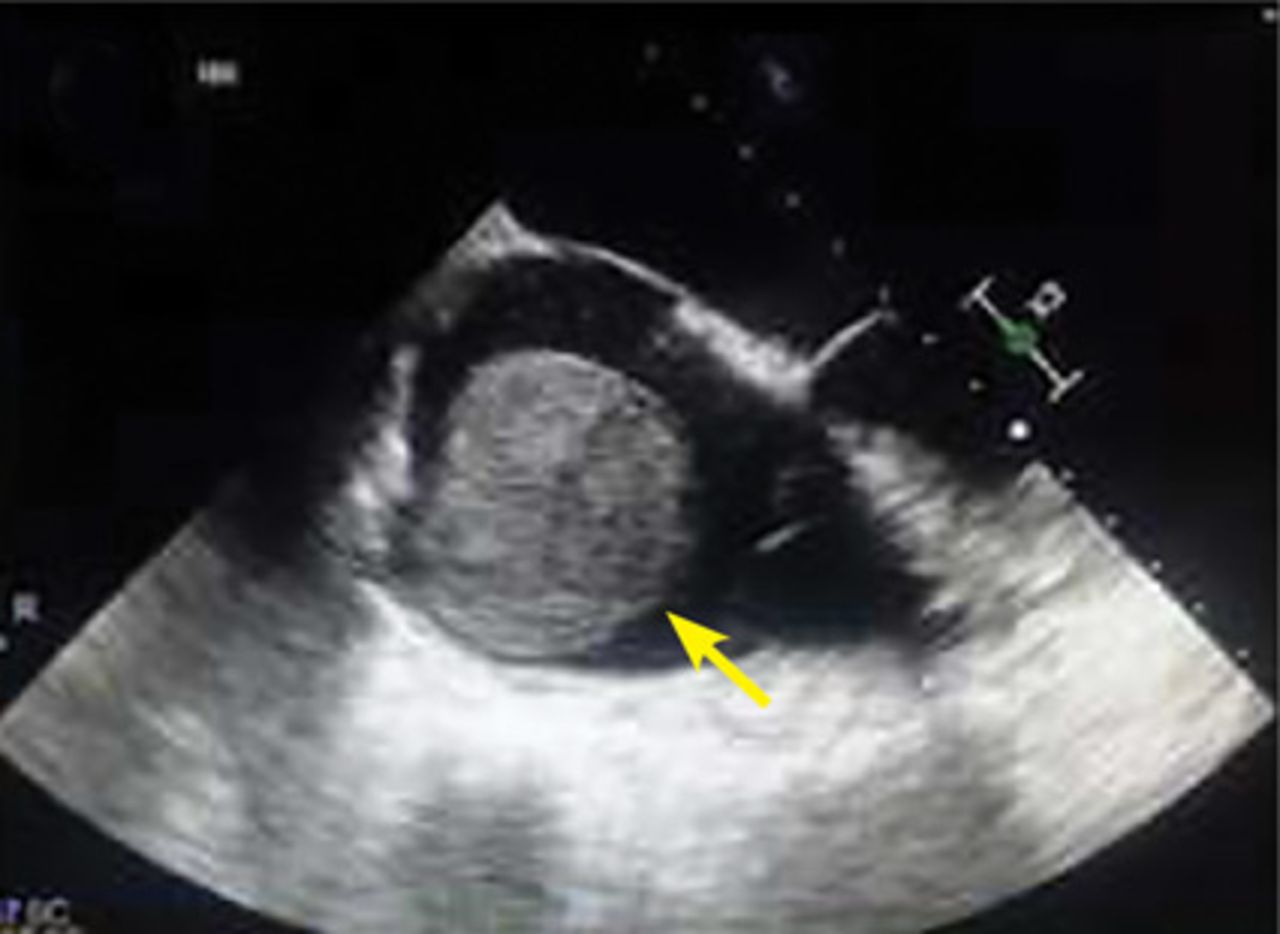
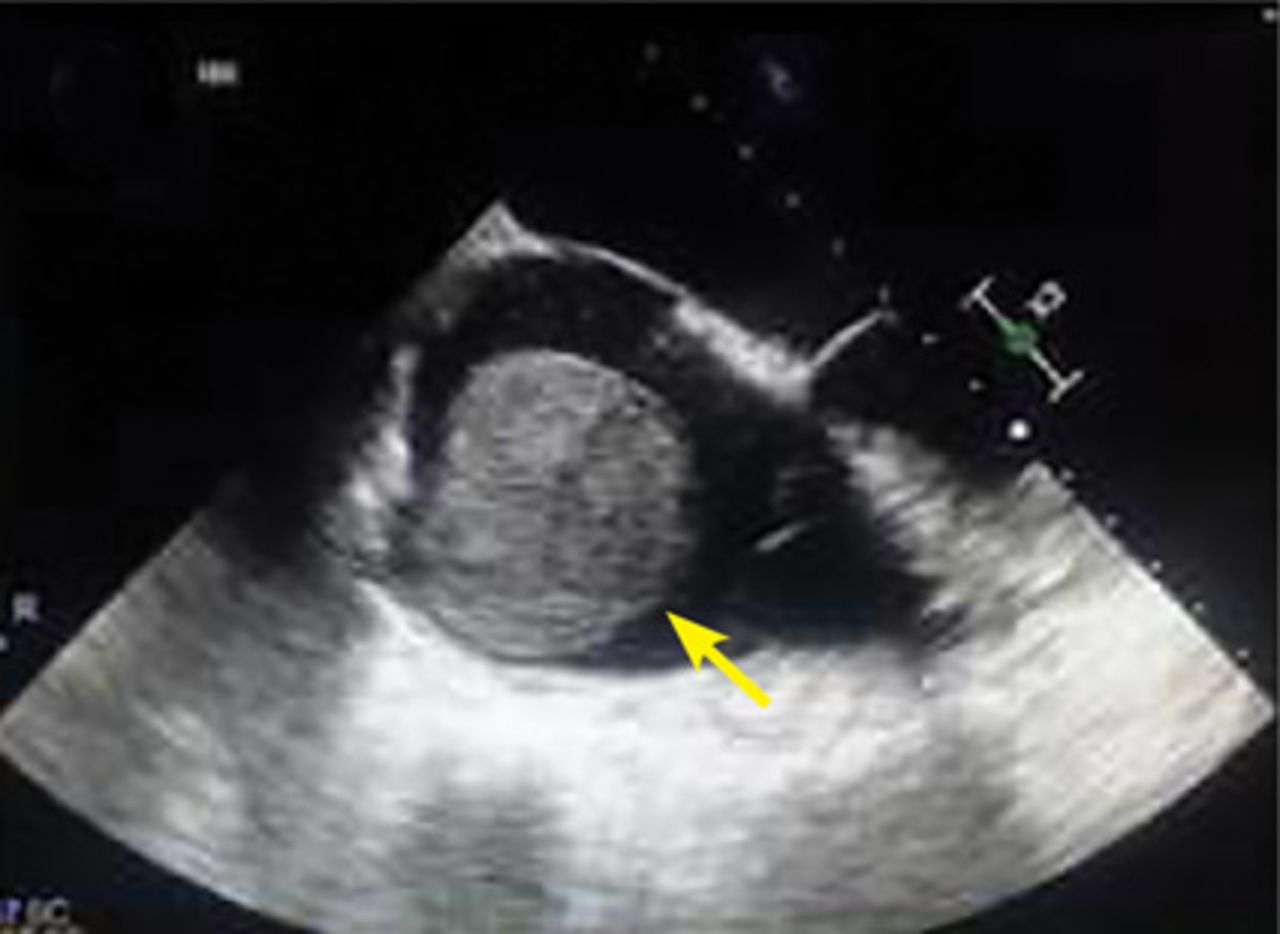
Transthoracic echocardiography confirmed a large round echogenic right atrial mass measuring 4.5 by 4.3 cm (Figure 2). The mass appeared to encroach into the tricuspid valve orifice, but there was no evidence of functional obstruction or stenosis.

Transthoracic echocardiography.
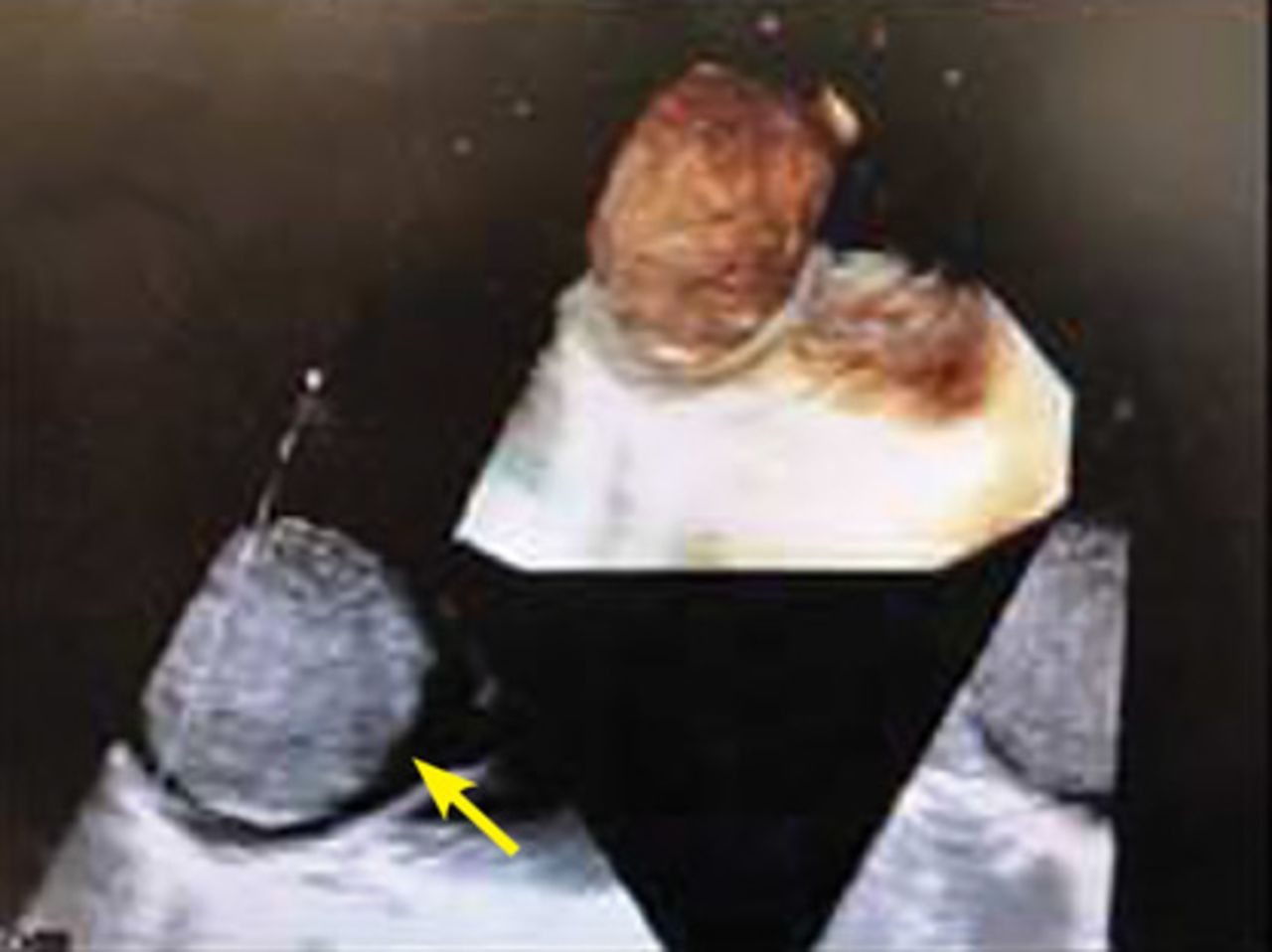
Transesophageal echocardiography showed a large globular echogenic mass measuring 5.5 by 4.6 cm with a stalk originating from the right atrial appendage (Figures 3 and 4). The mass was minimally mobile and did not obstruct the superior vena cava or the tricuspid orifice.
Transesophageal echocardiography.

Transesophageal echocardiography.
Given her history, the intracardiac mass strongly suggested metastatic adenocarcinoma. Other possibilities in the differential diagnosis were thrombus, myxoma, lipoma, angiosarcoma, and lymphoma.1,2
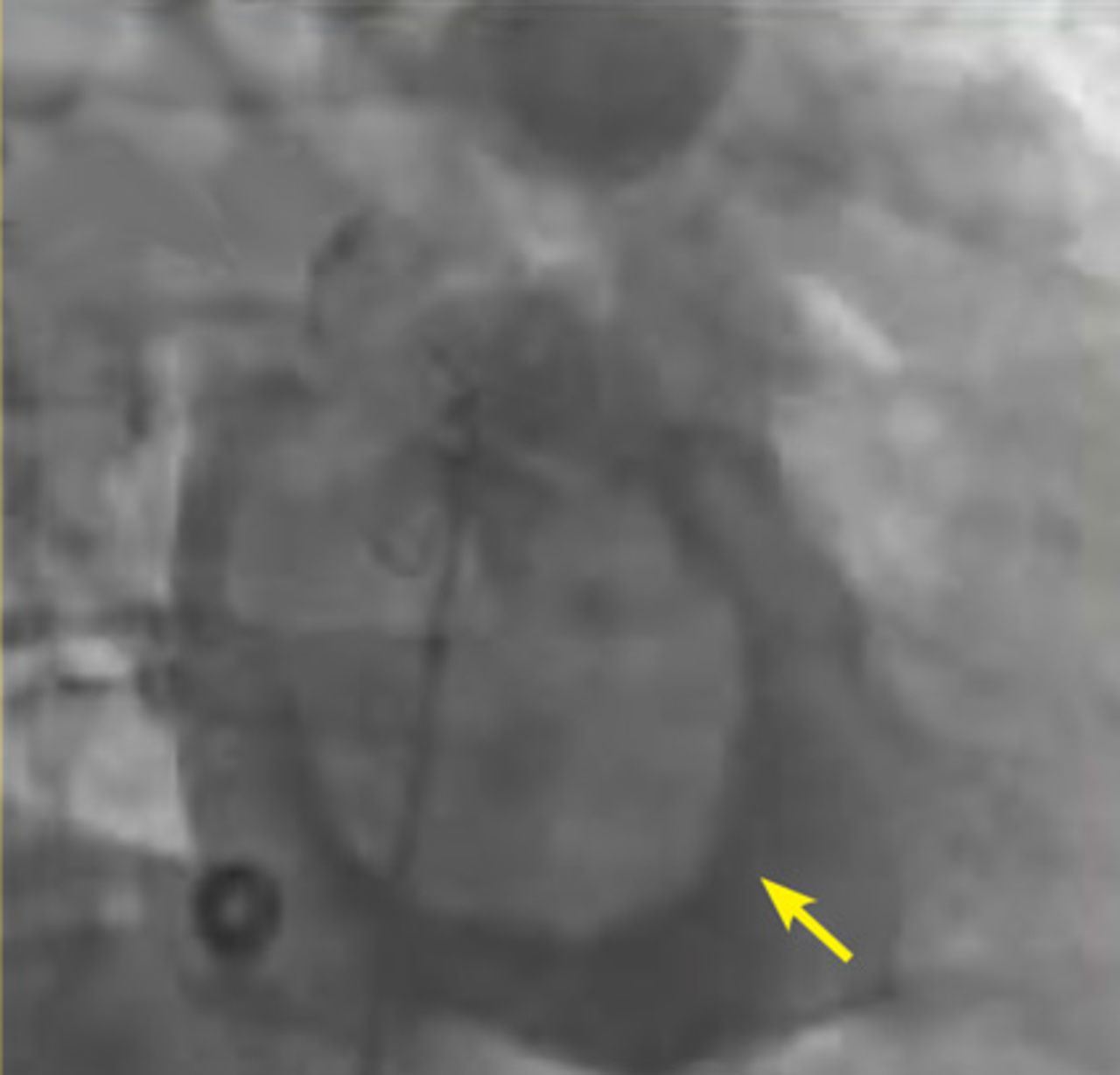
The cardiovascular team was consulted, and they recommended proceeding with open heart surgery and resection of the mass. In preparation for the surgery, cardiac catheterization was performed, and did not show any significant coronary artery disease. However, using a pigtail catheter, right atrial angiography demonstrated a large, round, mobile mass attached to the wall of the right atrium (Figure 5).
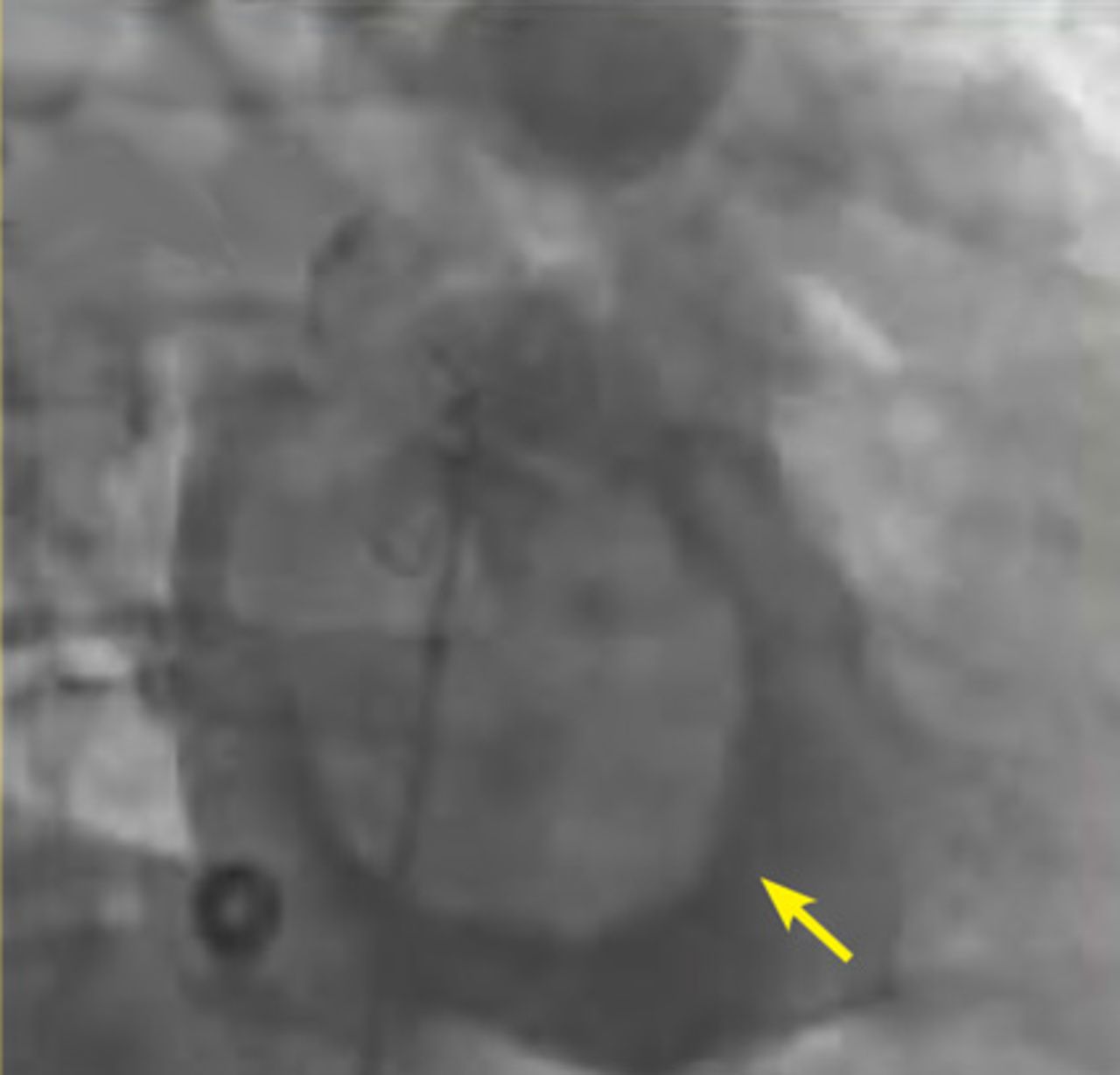
Angiography with pigtail catheter.
The patient underwent surgery, and the tumor was resected (Figures 6 and 7). Pathologic study confirmed the diagnosis of cardiac benign myxoma. The patient recovered and was eventually discharged to her home.

Operative photograph.
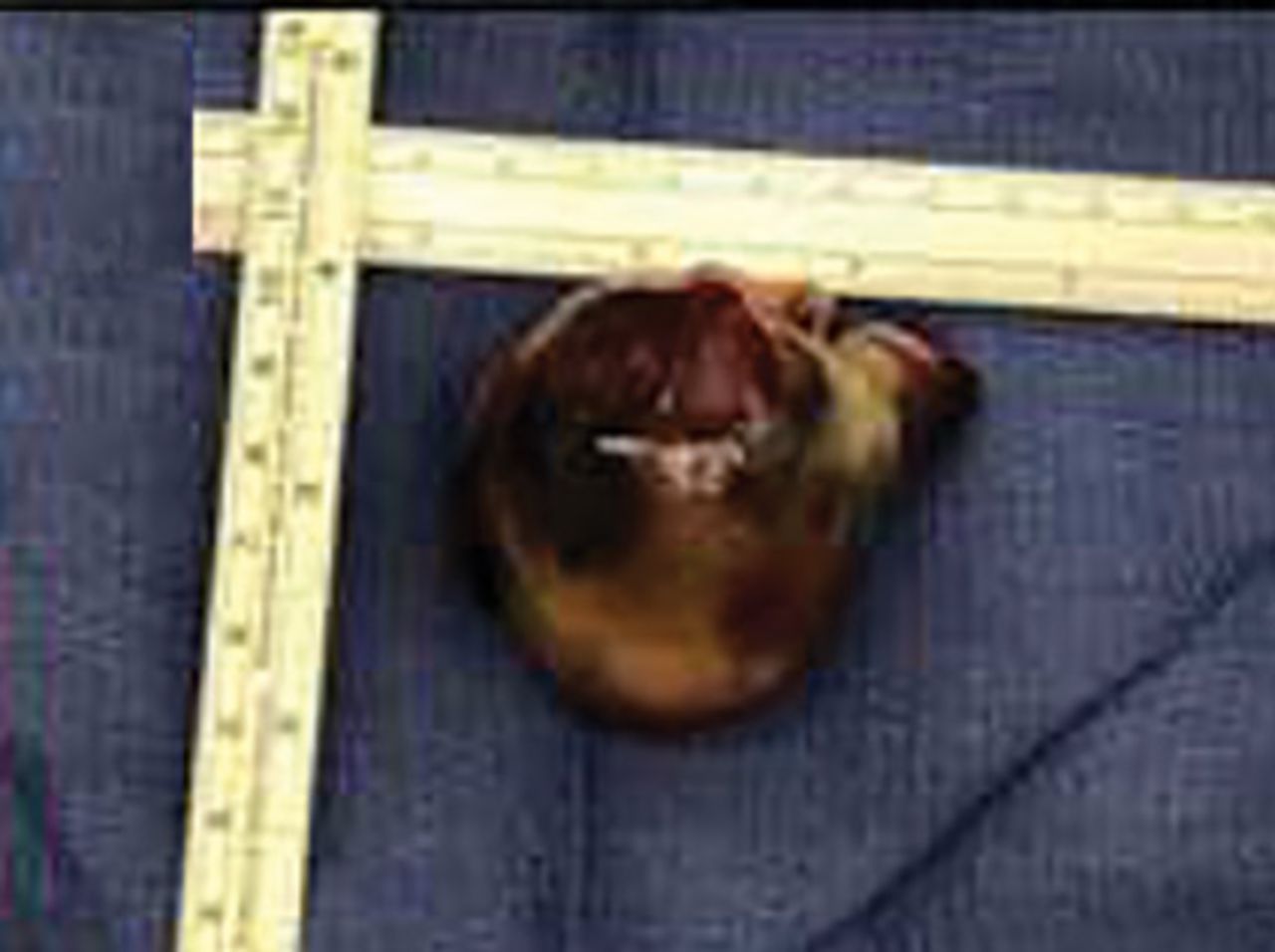
Gross section.
PRIMARY HEART TUMORS ARE RARE
Metastatic cardiac tumors are more common than primary cardiac tumors. On autopsy, between 0.01% and 0.1% of people in the general population have primary cardiac tumors, while 0.7% to 3.5% have metastatic tumors.3 About 75% of primary cardiac tumors are benign. In autopsies of patients with malignant neoplasms, cardiac metastasis has been found in 6% to 20%.4 Further, right-sided masses typically raise the concern of metastatic disease, whereas benign masses are more commonly found on the left side.
The most common neoplasms that metastasize to the heart are malignant melanoma, lymphoma, leukemia, breast, and lung cancers. The layers of the heart affected by malignant neoplasms in order of frequency from highest to lowest are the pericardium, epicardium, myocardium, and endocardium.3
MYXOMA: A PRIMARY CARDIAC TUMOR
The most common type of primary cardiac tumor is myxoma. Most—75% to 80%—occur in the left atrium, while 15% to 20% occur in the right atrium.5 Right atrial myxomas are usually found in the intraatrial septum at the border of the fossa ovalis.6 Myxomas can occur at any age, but are most common in women between the third and sixth decades.2
The cause of atrial myxomas is currently unknown. Most cases are sporadic. However, 10% are familial, with an autosomal-dominant pattern.7
The clinical symptoms of right atrial myxoma depend on the tumor’s size, location, and mobility and on the patient’s physical activity and body position.4 Common presenting symptoms include shortness of breath, pulmonary edema, cough, hemoptysis, and fatigue. Thirty percent of patients present with constitutional symptoms.4
Auscultation may reveal a characteristic “tumor plop” early in diastole.4,7 About 35% of patients have laboratory abnormalities such as elevations in erythrocyte sedimentation rate, C-reactive protein, and globulin levels and anemia. Our patient did not.
Embolization occurs in about 10% of cases of right-sided myxoma and can result in pulmonary artery embolism or a stroke. Pulmonary artery embolism occurs with myxoma embolization to the lungs. Strokes can occur in patients who have a patent foramen ovale or atrial septal defect, through which embolism to the systemic arterial circulation can occur.
The primary treatment for myxoma is complete resection of the tumor and its base with wide safety margins. This is particularly important to prevent recurrence of the myxoma and need for repeat operations, with their risk of surgical complications.9
- Copyright © 2019 The Cleveland Clinic Foundation. All Rights Reserved.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.