


Article Figures & Data
Figures


Tables
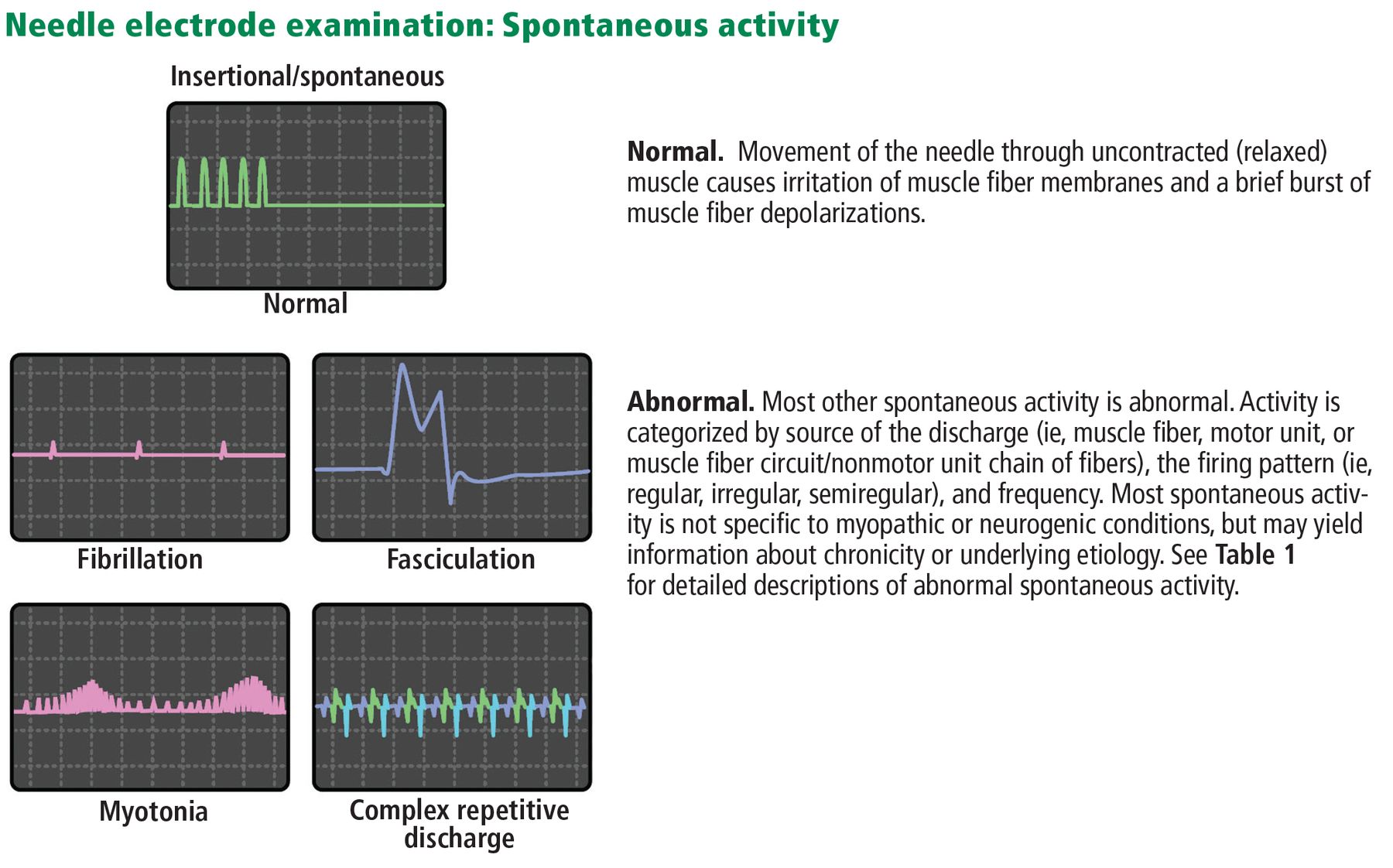
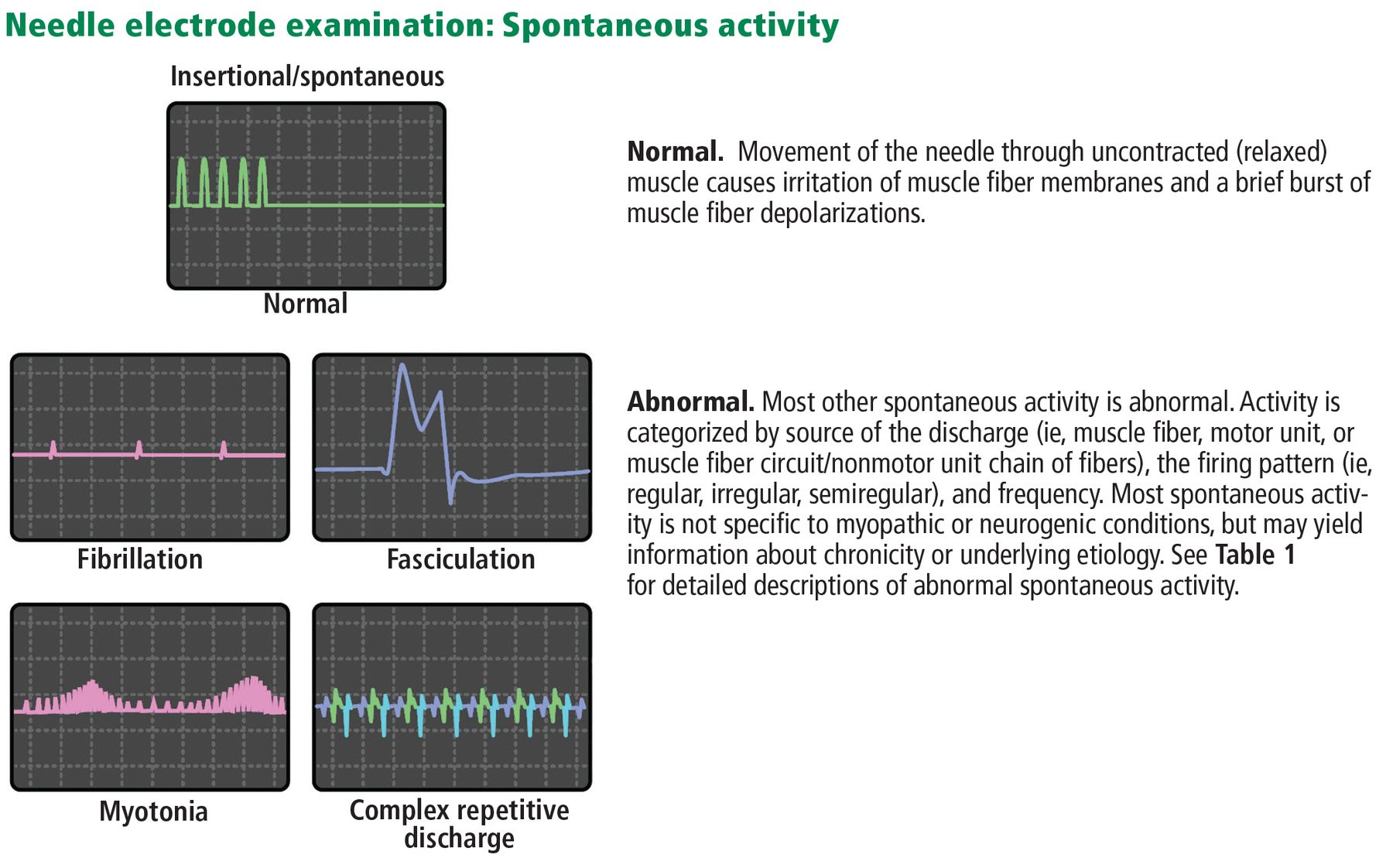
Term Description Clinical significance Fibrillation potentials and positive sharp waves Spontaneous muscle fiber potentials recorded during rest; morphology and firing regularity determine categorization as fibrillation potentials or positive sharp waves Muscle fibers are remaining without innervation, generally a sign of recent or ongoing denervation in neurogenic conditions
In myopathic conditions, they may indicate inflammatory or necrotizing myopathiesFasciculation potentials Spontaneous, irregularly firing motor unit discharges May be seen occasionally in chronic neurogenic conditions of any kind, but are seen more diffusely in disorders of the anterior horn cell and motor neuron disease Myotonic discharges Single muscle fiber firing repetitively in a waxing andwaning pattern at high frequency When diffuse and prominent, indicates a myotonic disorder
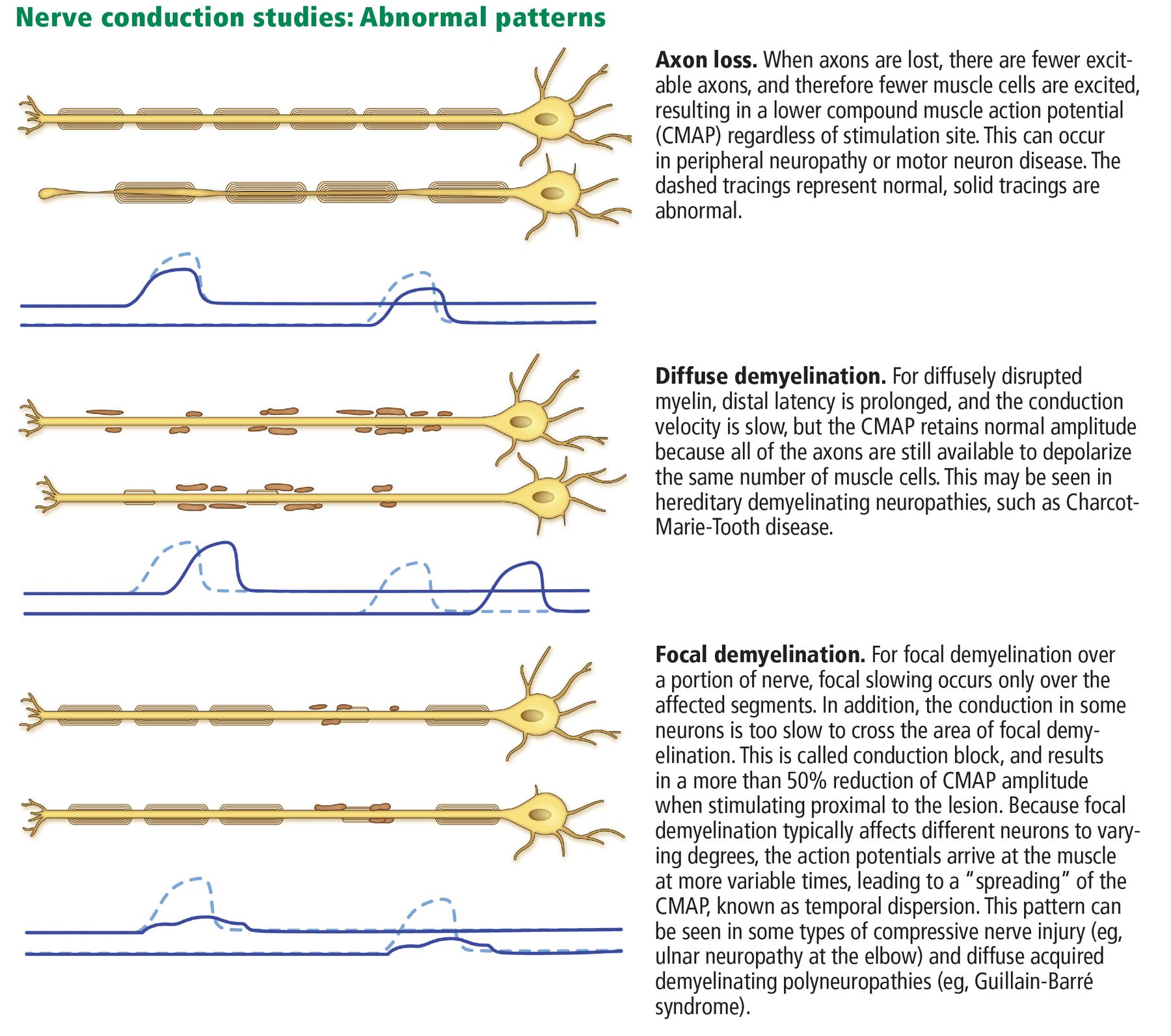
Can also rarely be seen in any chronic neurogenic or myopathic conditionComplex repetitive discharges Time-locked repetitive firing of a group of muscle fibers, with sudden start and stop of bursts Very chronic neurogenic or myopathic conditions Neuromyotonic discharges Single motor unit firing repetitively at a very high frequency Typically, disorders of voltage-gated potassium channels Myokymic discharges Single motor unit firing in regularly recurring bursts Most commonly associated with chronic demyelination and radiation plexopathy Term Description Clinical pearls Chronic denervation Remote axon loss identified by long-duration, high-amplitude motor units firing with a reduced recruitment pattern Generally denotes a process that started at least several months before the examination Active or ongoing denervation A muscle exhibiting positive sharp waves or fibrillation potentials, reflecting a subacute (or more long-standing but uncompensated) neurogenic or axon-loss process Does not always imply a truly active process. Fibrillation potentials and positive sharp waves are observed whenever a muscle fiber is awaiting reinnervation. These findings generally appear by about 3 weeks after the onset of injury and resolve within a few months, but may persist for longer in distal muscles and when reinnervation mechanisms are not fully successful or complete Intraspinal canal lesion or process Electrodiagnostic testing characterized by neurogenic or axon-loss changes in muscles of 1 or more specific myotomes (eg, a spinal root or segment derivative) without sensory findings The lesion is proximal to the dorsal root ganglion. Most of these lesions are compressive radiculopathies; but infrequently; other lesions such as motor neuron disease produce similar findings Neurogenic Electrodiagnostic features resulting from lesions of the anterior horn cell, nerve root, plexus, or nerve Neurogenic findings are further refined by distribution and the presence or absence of sensory findings Myopathic Electrodiagnostic features of muscle disease, including low amplitude, short duration, and polyphasic motor units Electrodiagnostic testing may be less sensitive in many myopathies than in neurogenic conditions Irritable myopathy When myopathic features are accompanied by diffuse fibrillation potentials, positive sharp waves, or both Suggestive of inflammatory or necrotizing etiologies, but not pathognomonic Motor unit instability The same motor unit on needle electrode examination varies in morphology from one firing to the next Indicates dysfunction at the neuromuscular junction, but it can be seen in neurogenic conditions during early reinnervation, when neuromuscular junctions are immature Reduced activation Suboptimal voluntary activation of a muscle resulting from central nervous system causes Can result from pain, cognitive dysfunction, poor effort, or upper motor neuron pathology, and indicates that the data may be of lower yield Conduction block Motor response in a nerve conduction study has > 50% reduced response when stimulating at a more proximal location Indicates focal demyelination When occurring at noncompression sites or in multiple nerves, can suggest acquired demyelinating polyneuropathies
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.