


A 70-year-old man with dyslipidemia and new-onset hypertension presented to the emergency room with nausea, fatigue, and confusion. His blood pressure was 148/87 mm Hg. Computed tomography (CT) without contrast was performed as part of the evaluation of his acute-onset altered mental status, and showed no acute intracranial abnormalities (Figure 1).
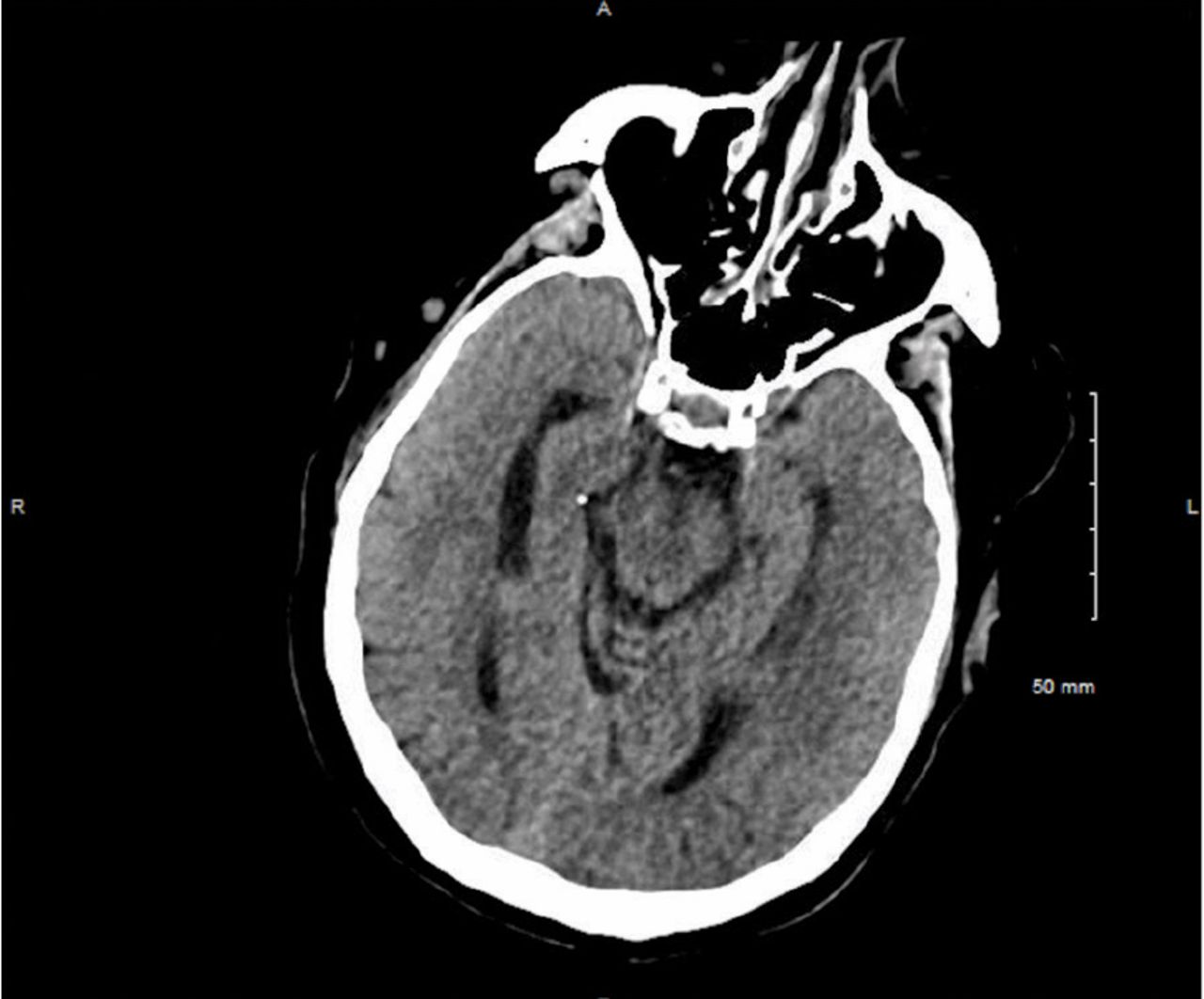
On presentation, noncontrast computed tomography (CT) was normal.
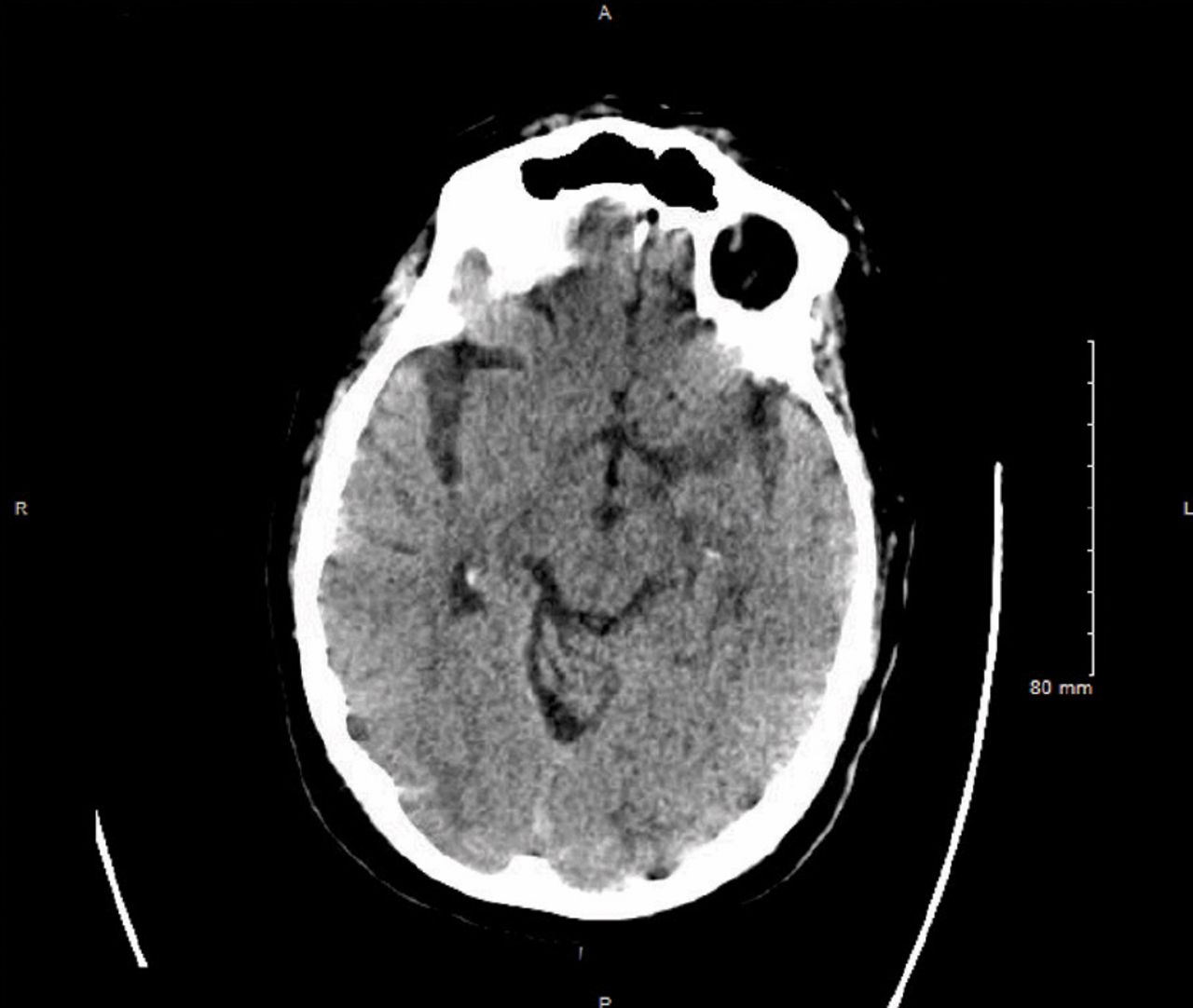
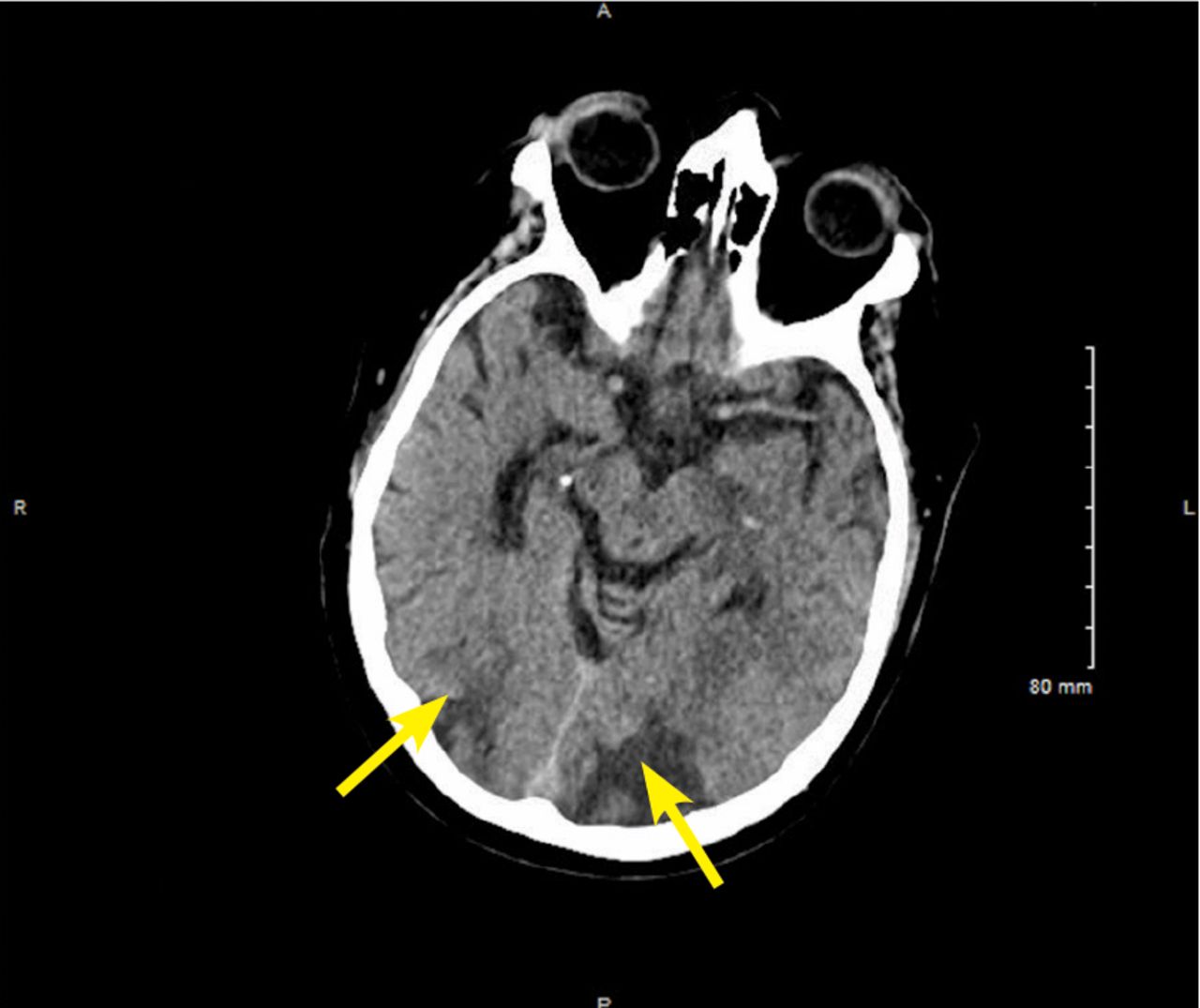
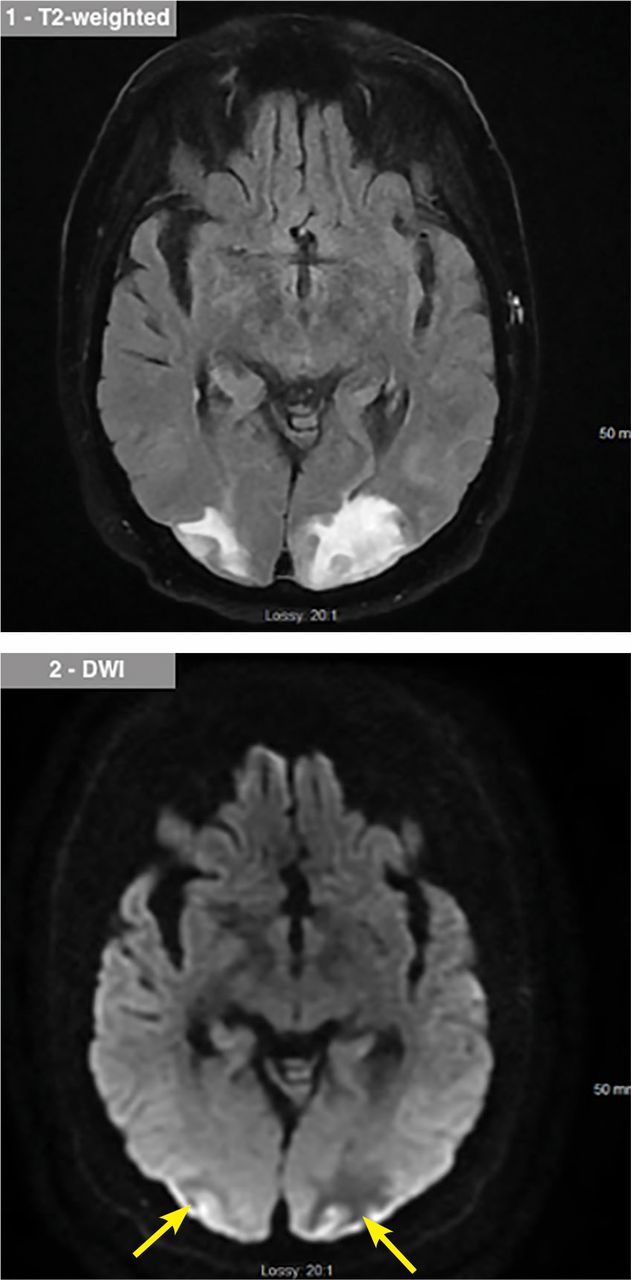
The patient was admitted to the hospital for observation. His blood pressure remained poorly controlled. On hospital day 4, he developed severe right occipital headache and blurred vision, and his blood pressure was noted to be 209/93 mm Hg. Repeat noncontrast CT showed hypodensities (vasogenic edema) in both occipital lobes (Figure 2), which, along with his symptoms, raised the suspicion of posterior reversible encephalopathy syndrome. The findings were confirmed on magnetic resonance imaging (MRI) (Figure 3).

On hospital day 4, repeat CT imaging showed areas of hypodensity in both occipital lobes (arrows), indicating vasogenic edema.

Magnetic resonance imaging on hospital day 4 noted hyperintensities on T2 (top) and diffusion-weighted images (bottom), confirming findings on tomography.
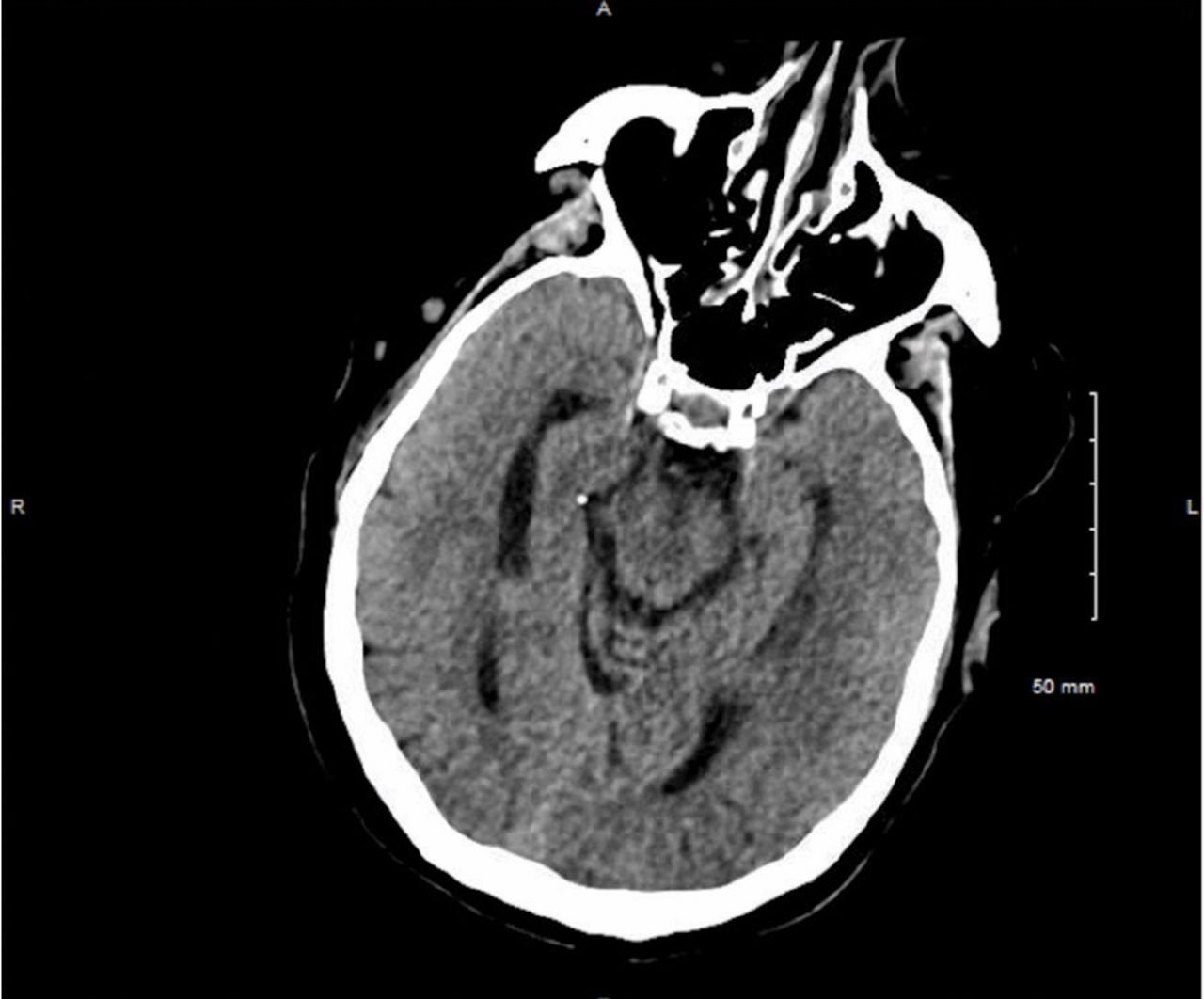
The patient’s symptoms were better the next day, after his blood pressure had been brought under control with intravenous hydralazine. On day 10, repeat noncontrast CT showed the vasogenic edema had nearly resolved (Figure 4), and his visual complaints had completely resolved.
On hospital day 10, the vasogenic edema had nearly resolved.
EPIDEMIOLOGY AND PATHOPHYSIOLOGY
Posterior reversible encephalopathy syndrome is a rare condition most often seen in hypertensive emergencies but also in sepsis, preeclampsia, eclampsia, and with the use of cytotoxic medications such as cyclosporine and tacrolimus.1 It is thought to occur secondary to derangement in cerebral autoregulation with subsequent hyperperfusion, resulting in endothelial damage and vasogenic edema.2 In a series of 70 patients admitted to the intensive care unit, 11 (16%) died within 90 days, but 33 (47%) had a good recovery.3
CLINICAL PRESENTATION AND TREATMENT
The diagnosis is often missed. The clinical presentation typically consists of headaches, visual disturbances, seizures, and altered mental status.4 Features most commonly observed on CT or MRI are edema or swelling in the parieto-occipital white matter. On MRI, the syndrome usually manifests as a T2 hyperintensity with normal diffusion-weighted imaging.
Clinical symptoms and radiologic findings can improve rapidly with management of blood pressure. Late diagnosis or inadequate therapy may contribute to long-term sequelae such as permanent neurologic disability or death from progressive cerebral edema and intracranial hemorrhage.5
TAKE-HOME POINTS
Posterior reversible encephalopathy syndrome is usually reversible, and many patients recover fully.
Clinical and radiologic manifestations resolve rapidly with blood pressure management.
- Copyright © 2020 The Cleveland Clinic Foundation. All Rights Reserved.




{kind=link}
{kind=link}
{kind=link}
{kind=link}