


To the Editor: We read with great interest the article by Mgbokikwe et al about newer and more sophisticated imaging modalities for the evaluation of infective endocarditis.1 As outlined in Table 1 of the article, each imaging method has its advantages and limitations. One further imaging modality that should not be overlooked in select patients, however, is intracardiac echocardiography (ICE).
ICE is performed in the cardiac catheterization laboratory and requires an 8- to 10-Fr sheath in the femoral or jugular vein. Through this, the ICE catheter is advanced to the right heart, where imaging can be performed, not only of the right-sided valves, but also of the aortic and mitral valves.2,3
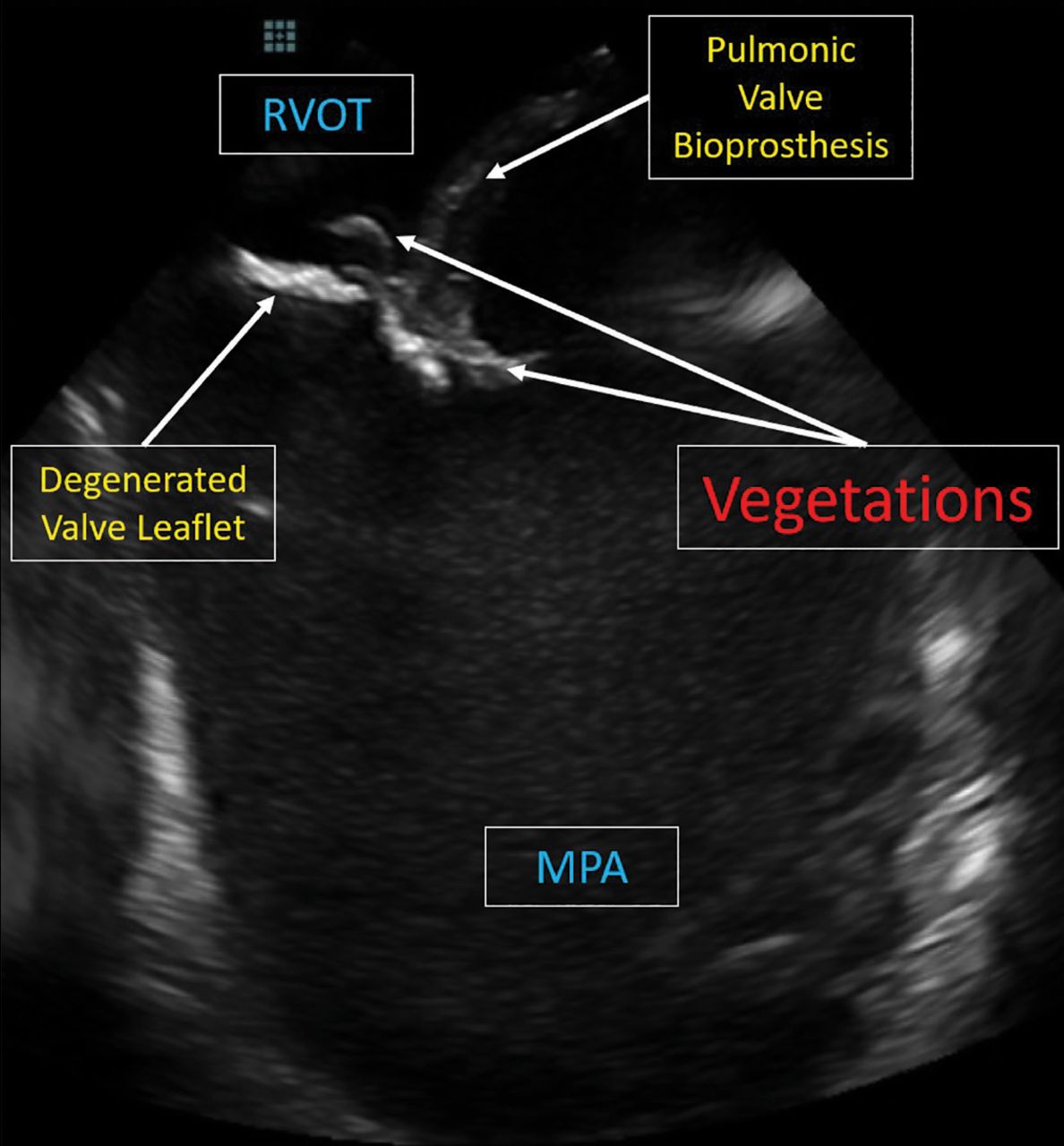
In certain cases, ICE avoids the use of sedation or general anesthesia and is an option for those with oropharyngeal or esophageal structural abnormalities for which transesophageal echocardiography (TEE) is contraindicated. ICE has been shown to be helpful in the evaluation of cardiac device and prosthetic valve endocarditis where TEE was unrevealing (Figure 1). Acoustic shadowing and artifacts from leads and prosthetic valves, in addition to the distance of the esophageal echo probe to the anterior right heart structures, limit the diagnostic capability of TEE compared with ICE. ICE is also useful for planning lead extraction and for monitoring for intraprocedural complications.4
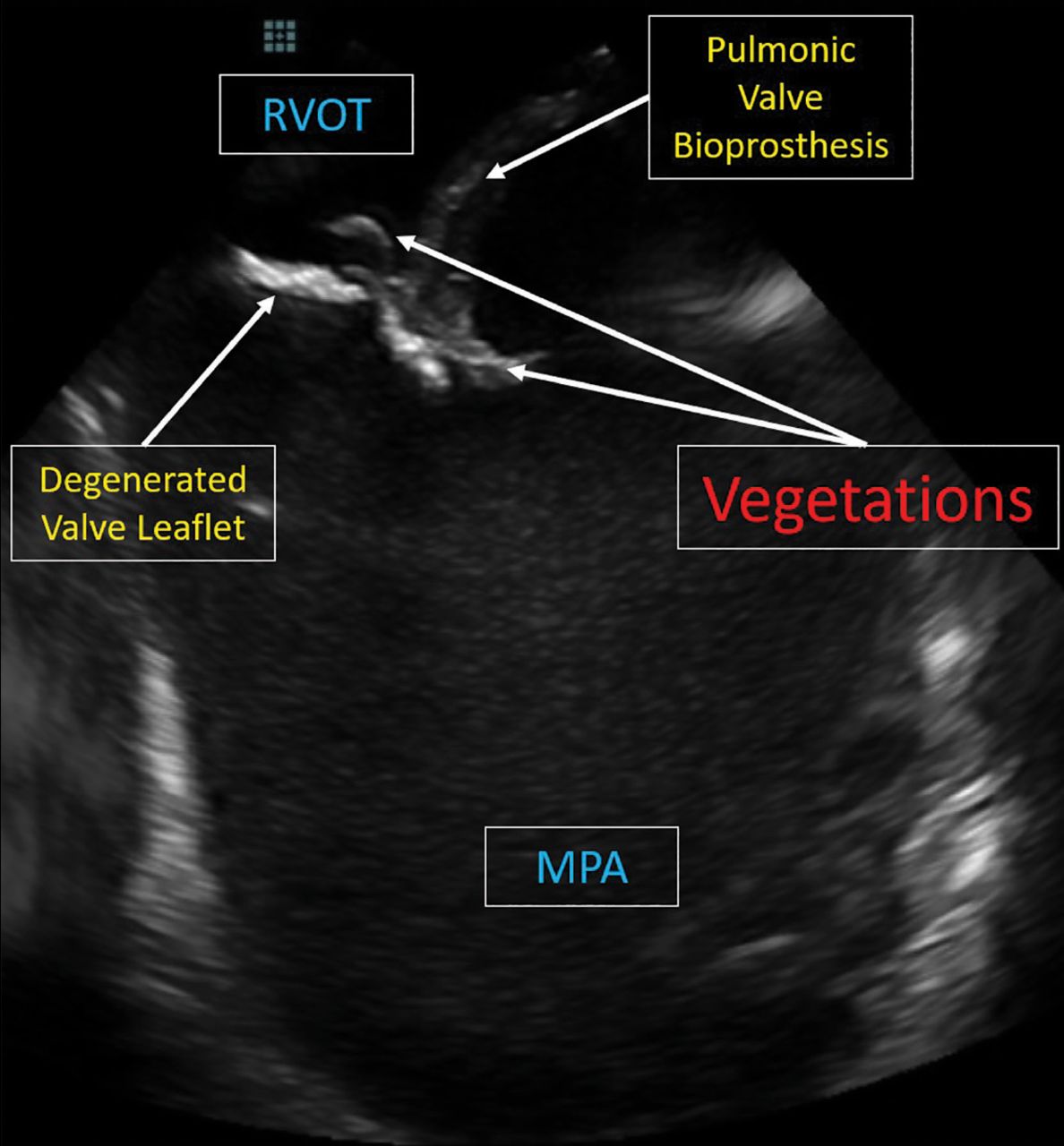
Intracardiac echocardiographic view of a pulmonic valve bioprosthesis in a 34-year-old man with repaired tetralogy of Fallot who presented with Streptococcus mitis bacteremia. Neither transthoracic nor transesophageal echocardiography could visualize valvular vegetations.
MPA = main pulmonary artery; RVOT = right ventricular outflow tract
Overall, risks of ICE are low and include transient atrial arrhythmias, cardiac chamber injury, and access site bleeding. Lastly, net procedural costs are not excessively higher than those of TEE.
- Copyright © 2020 The Cleveland Clinic Foundation. All Rights Reserved.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.